Imnci 10 marks
Reading File
Finding Sources
Searching the Web
IMNCI integrated management neonatal childhood illness 10 marks exam notes
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a complete, exam-ready 10-mark answer on IMNCI:
IMNCI - Integrated Management of Neonatal and Childhood Illness
Definition & Background
IMNCI is the Indian adaptation of the WHO/UNICEF strategy IMCI (Integrated Management of Childhood Illness). It was developed under the RCH II/NRHM framework and is the central pillar of child health interventions in India. The Indian version was specifically renamed IMNCI because it extends coverage to include the first 7 days of life (neonates), unlike the original IMCI which covered only 1 week to 5 years.
- Park's Textbook of Preventive and Social Medicine
Why IMNCI is Needed
Most sick children present with signs and symptoms of more than one condition simultaneously. A single diagnosis is often not possible or appropriate, making an integrated approach necessary. Common causes of childhood morbidity and mortality addressed by IMNCI include:
- Diarrhoea (13%)
- ARI / Pneumonia (17%)
- Fever / Malaria (27%)
- Malnutrition (43%)
- Measles, Ear infections
Three Main Components (Prongs) of IMNCI
| Component | Details |
|---|---|
| 1. Case Management Skills | Improvement in skills of health staff through locally adapted guidelines and training |
| 2. Health System Strengthening | Improvements in the health system required for effective management of childhood illness |
| 3. Family and Community Practices | Improvements in family health practices, caretaker counselling, and community engagement |
Indian Adaptations (Highlights)
Compared to the original IMCI, India's version includes:
- Inclusion of 0-7 days age (neonatal period) in the programme
- Incorporation of national guidelines on malaria, anaemia, Vitamin A supplementation and immunization schedule
- Training begins with sick young infants up to 2 months
- Equal proportion of training time devoted to sick young infants and sick children
- It is skill-based training
Target Age Groups
IMNCI guidelines cover two groups using two separate sets of charts:
- Young infants: Age 1 week up to 2 months
- Older children: Age 2 months up to 5 years
The IMNCI Case Management Process
The integrated case management process involves 6 steps:
a. ASSESS - Check for danger signs first, then assess main symptoms (cough/difficulty breathing, diarrhoea, fever, ear problems), nutrition status, immunization status, and other problems.
b. CLASSIFY - Using a colour-coded triage system:
| Colour | Action | Condition |
|---|---|---|
| Pink | Urgent referral | Severe/life-threatening illness |
| Yellow | Treatment at outpatient facility | Moderate illness; oral drugs, local infection treatment |
| Green | Home management | Mild illness; counsel caretaker |
c. IDENTIFY TREATMENT - Develop an integrated treatment plan; give first dose of drugs in clinic.
d. TREAT - Provide practical treatment instructions; teach caretaker how to give oral drugs, treat local infections at home.
e. COUNSEL - Advise on feeding, fluids, when to return immediately for follow-up.
f. FOLLOW-UP - When child returns, give follow-up care and reassess for new problems.
The Flowchart:
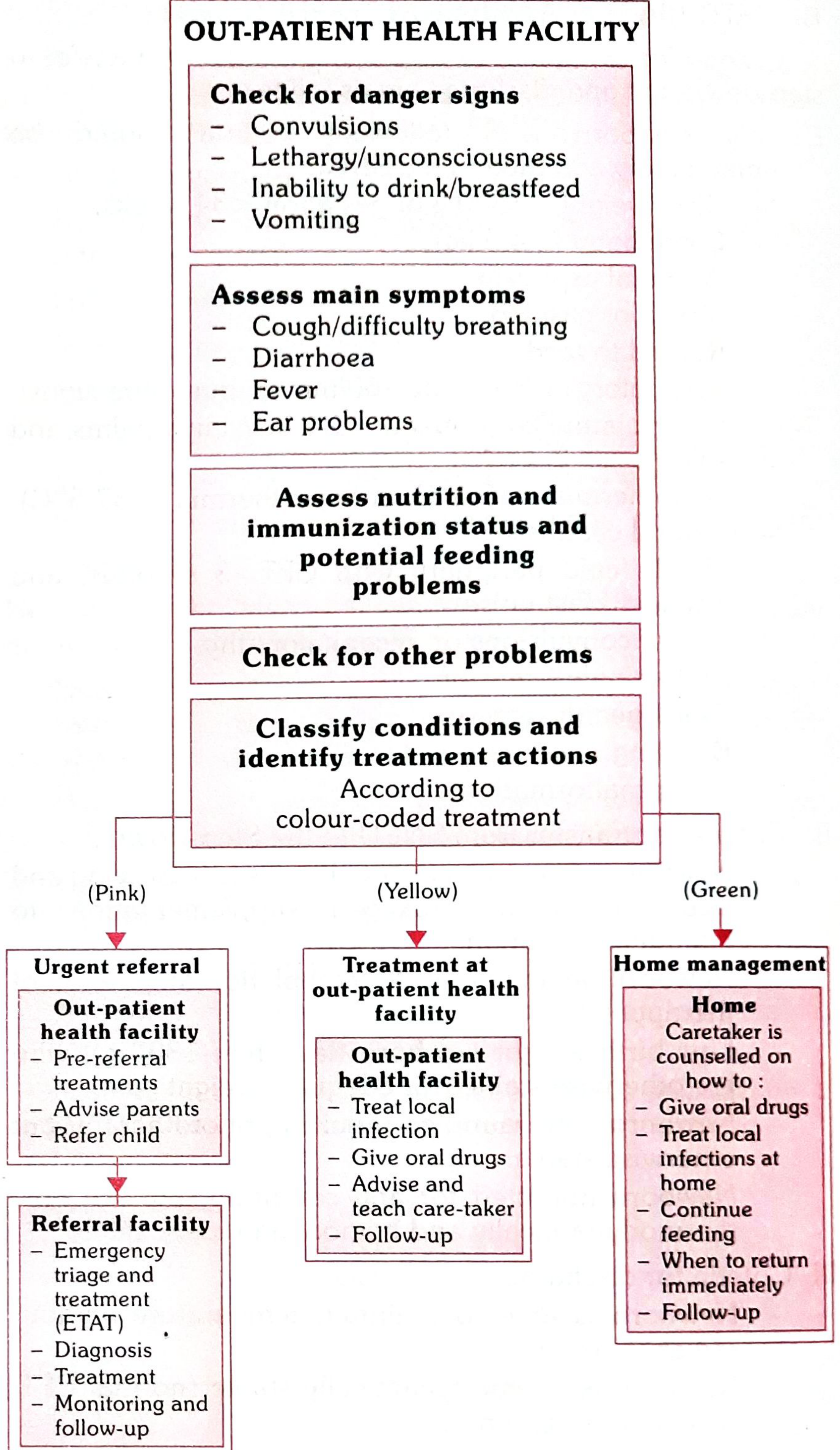
Danger Signs Checked in IMNCI
Four general danger signs requiring urgent referral (Pink):
- Convulsions
- Lethargy or unconsciousness
- Inability to drink or breastfeed
- Vomiting everything
Types/Forms of IMNCI
1. Community IMNCI
- Implemented at household level through ASHA workers
- ANMs at sub-centre level
- Medical officers, nurses, LHVs at PHC level
2. Pre-service IMNCI
- Included in the curriculum of medical colleges
- Helps build trained IMNCI manpower for public and private sectors
3. Facility-Based IMNCI (F-IMNCI)
- Integration of facility-based care with the IMNCI package
- Empowers health personnel to manage neonatal and childhood illness at both community and health facility levels
- Focuses on inpatient management of:
- Birth asphyxia, Sepsis, Low birth weight
- Pneumonia, Diarrhoea, Malaria
- Meningitis, Severe malnutrition
- Master trainers: Paediatricians from tertiary hospitals and medical colleges
Facility Infrastructure Under IMNCI
| Facility | Newborn Care |
|---|---|
| PHC/Sub-centre (MCH Level I) | Newborn Care Corner (NBCC) - mandatory |
| CHC/FRU (MCH Level II) | NBCC + Newborn Stabilization Unit (NBSU) - 4 bedded |
| District Hospital (MCH Level III) | NBCC + Special Newborn Care Unit (SNCU) |
Limitations of IMNCI Guidelines
- Do not cover trauma or acute emergencies due to accidents/injuries
- Do not specifically address AIDS (though diarrhoea and ARI in HIV children are managed the same way)
- Do not cover chronic problems or less common illnesses
- Effectiveness depends on timely presentation to a trained health worker by the family
Importance / Objectives
- Reduce child deaths and frequency/severity of illness
- Contribute to improved child growth and development
- Promote rational, effective, and affordable use of drugs (syndromic approach)
- Ensure quality care at first-level health facilities
- Empower families and communities in child health practices
Source: Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.