Anatomy of female reproductive system
Reading File
search_medical_text
anatomy of female reproductive system organs structure
search_medical_image
female reproductive system anatomy diagram
GradeResponse
GradeResponse
Anatomy of the Female Reproductive System
The female reproductive system consists of both internal and external organs, primarily located in the pelvic cavity. These structures develop embryologically from the Müllerian (paramesonephric) ducts, which form the uterus, fallopian tubes, cervix, and upper third of the vagina, while the urogenital sinus gives rise to the lower two-thirds of the vagina (Bailey & Love's Surgery, 28th Ed., p. 1596).
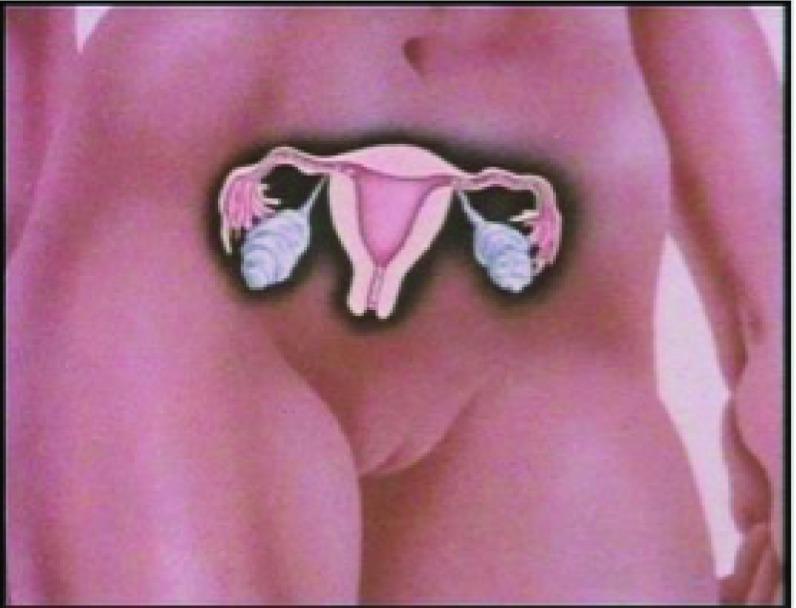
Internal Organs
1. Ovaries
- Paired gonads, almond-shaped, ~3 × 2 × 1 cm
- Located in the ovarian fossa on the lateral pelvic wall
- Attached to the uterus by the ovarian ligament and to the pelvic wall by the suspensory (infundibulopelvic) ligament
- Functions: Oogenesis (egg production) and secretion of estrogen and progesterone
- Cortex contains follicles at varying stages of development (primordial → mature Graafian follicle)
2. Fallopian Tubes (Uterine Tubes)
- Two muscular tubes, ~10 cm long, extending from the uterine cornua to the ovaries
- Parts (medial → lateral):
Segment Features Intramural (interstitial) Passes through uterine wall; narrowest part Isthmus Thick-walled, narrow lumen Ampulla Widest; usual site of fertilization Infundibulum Funnel-shaped; bears fimbriae that sweep the ovum - Lined by ciliated columnar epithelium that facilitates ovum transport
3. Uterus
- Hollow, pear-shaped muscular organ, ~7.5 × 5 × 2.5 cm (nulliparous)
- Parts:
- Fundus — dome above the fallopian tube openings
- Body (corpus) — main part; contains the triangular uterine cavity
- Isthmus — narrow junction between body and cervix
- Cervix — lower cylindrical part; projects into the vagina
- Layers of the uterine wall:
Layer Description Perimetrium Outer serosal (peritoneal) covering Myometrium Thick smooth muscle; contracts during labor Endometrium Inner glandular lining; undergoes cyclic changes - Supports: Held in place by the broad, round, cardinal (Mackenrodt's), and uterosacral ligaments; normal position is anteverted and anteflexed
- Blood supply: Uterine artery (branch of internal iliac)
4. Cervix
- Lower cylindrical segment, ~2.5–3 cm long
- Ectocervix: Covered by stratified squamous epithelium (visible on speculum exam)
- Endocervix: Lined by mucus-secreting columnar epithelium
- Transformation zone (squamocolumnar junction): Clinically important site where most cervical cancers arise
- Internal os opens into the uterine cavity; external os opens into the vagina
5. Vagina
- Fibromuscular canal, ~8–10 cm long, connecting cervix to the external genitalia
- Upper third from Müllerian ducts; lower two-thirds from urogenital sinus
- Lined by stratified squamous epithelium (non-keratinized)
- Forms fornices (anterior, posterior, and lateral) around the cervix — the posterior fornix is deepest and lies adjacent to the rectouterine pouch (Pouch of Douglas)
- Functions: Birth canal, menstrual outflow, copulation
External Genitalia (Vulva)
| Structure | Description |
|---|---|
| Mons pubis | Fatty eminence over the pubic symphysis |
| Labia majora | Two large fatty skin folds; homologous to the scrotum |
| Labia minora | Inner thin folds; no subcutaneous fat; enclose the vestibule |
| Clitoris | Erectile organ at the anterior junction of labia minora; homologous to the penis |
| Vestibule | Space between labia minora; contains urethral and vaginal openings |
| Bartholin's glands | (Vestibular glands) Secrete lubricating mucus during arousal |
| Skene's glands | (Paraurethral glands) Adjacent to the urethral orifice |
| Hymen | Thin membrane partially covering the vaginal opening |
Blood Supply Summary
| Organ | Artery |
|---|---|
| Uterus & fallopian tubes | Uterine artery (internal iliac) |
| Ovaries | Ovarian artery (directly from aorta at L2) |
| Vagina (upper) | Vaginal branches of uterine artery |
| Vagina (lower) | Internal pudendal artery |
| Vulva | Internal & external pudendal arteries |
Lymphatic Drainage
| Organ | Primary Drainage |
|---|---|
| Ovaries | Para-aortic (lumbar) nodes |
| Uterine body | Internal/external iliac & para-aortic nodes |
| Cervix | Internal iliac, obturator, parametrial nodes |
| Vagina (upper) | Iliac nodes |
| Vagina (lower) / Vulva | Superficial inguinal nodes |
Nerve Supply
- Sympathetic: T10–L2 (uterus, tubes, ovaries)
- Parasympathetic: S2–S4 (pelvic splanchnic nerves)
- Somatic: Pudendal nerve (S2–S4) — external genitalia
Key Anatomical Relations
- Anteriorly: Bladder and urethra
- Posteriorly: Rectum; Pouch of Douglas (rectouterine pouch) lies between uterus and rectum — clinically important for ectopic fluid/blood
- Laterally: Ureters run ~1 cm lateral to the cervix ("water under the bridge" — ureters pass beneath the uterine artery), making them vulnerable during hysterectomy
Chronic hypertension in pregnancy
search_medical_text
chronic hypertension in pregnancy definition classification diagnosis
search_medical_text
chronic hypertension pregnancy management treatment antihypertensive drugs
search_medical_image
chronic hypertension pregnancy complications management
GradeResponse
GradeResponse
GradeResponse
Chronic Hypertension in Pregnancy
Definition
Chronic hypertension in pregnancy is defined as:
- A pre-existing diagnosis of hypertension, OR
- SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg on 2 occasions at least 4 hours apart before 20 weeks' gestation
(ACC/AHA Guidelines on High Blood Pressure in Adults, p. 64)
It is distinguished from gestational hypertension and preeclampsia, which arise at or after 20 weeks.
Classification of Hypertensive Disorders of Pregnancy
| Disorder | Onset | Key Features |
|---|---|---|
| Chronic hypertension | < 20 weeks or pre-existing | No proteinuria required; persists postpartum |
| Gestational hypertension | ≥ 20 weeks | No proteinuria; resolves postpartum |
| Preeclampsia | ≥ 20 weeks | HTN + proteinuria or end-organ damage |
| Superimposed preeclampsia | ≥ 20 weeks in chronic HTN patient | Worsening HTN + new proteinuria/end-organ damage |
| Eclampsia | Any time | Preeclampsia + seizures |
Risks & Complications
Women with chronic hypertension face elevated maternal and fetal risks (Harrison's, 21st Ed., p. 13634):
Maternal:
- Superimposed preeclampsia (most important complication; risk 15–25%)
- Placental abruption
- Stroke / hypertensive crisis
- Renal deterioration
- Cardiac failure (in severe/long-standing HTN)
Fetal/Neonatal:
- Intrauterine growth restriction (IUGR)
- Preterm birth
- Placental insufficiency
- Perinatal mortality (increased)
Pre-pregnancy & Early Pregnancy Evaluation
A thorough assessment should include (Harrison's, 21st Ed., p. 13634):
- Identify secondary/remediable causes of hypertension
- End-organ assessment — renal function, proteinuria (baseline), cardiac evaluation, fundoscopy
- Transition off teratogenic antihypertensives (especially ACE inhibitors and ARBs) before conception or as soon as pregnancy is confirmed
- Baseline proteinuria — helps differentiate pre-existing renal disease from later-developing preeclampsia
Blood Pressure Targets in Pregnancy
| Parameter | Target |
|---|---|
| Systolic BP | 130–150 mmHg |
| Diastolic BP | 80–100 mmHg |
| Emergency threshold | SBP ≥ 160 or DBP ≥ 110 → immediate hospitalization |
Targets balance maternal safety (preventing stroke, end-organ damage) with fetal perfusion (avoiding uteroplacental insufficiency from over-aggressive lowering). (Harrison's, p. 13634; Management of Elevated BP Guidelines, p. 60)
Antihypertensive Drug Management
First-Line Agents (Safe in Pregnancy)
| Drug | Class | Notes |
|---|---|---|
| Labetalol | α/β-blocker | Most commonly used; IV form for acute management |
| Nifedipine (extended-release) | Dihydropyridine CCB | Oral; preferred for outpatient chronic management |
| Methyldopa | Central α2-agonist | Long safety record; less preferred due to side effects |
(Harrison's, p. 13634; Management of Elevated BP Guidelines, p. 60)
Contraindicated in Pregnancy
| Drug Class | Reason |
|---|---|
| ACE inhibitors (e.g., enalapril, lisinopril) | Fetotoxic — renal dysgenesis, oligohydramnios, skull hypoplasia |
| Angiotensin Receptor Blockers (ARBs) | Same mechanism as ACEi; equally teratogenic |
| Direct renin inhibitors (e.g., aliskiren) | Insufficient safety data; avoid |
| Mineralocorticoid receptor antagonists (e.g., spironolactone) | Anti-androgenic effects on fetus |
Management Guidelines Summary
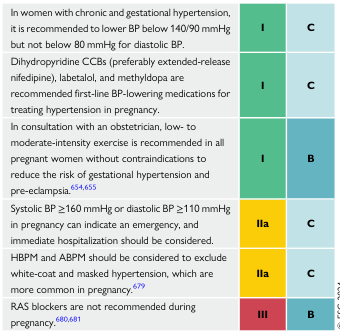
(Management of Elevated Blood Pressure and Hypertension Guidelines, p. 60)
Monitoring During Pregnancy
- Frequent antenatal visits — every 2–4 weeks (more frequent if poorly controlled)
- BP monitoring: Home BP monitoring (HBPM) and/or ambulatory BP monitoring (ABPM) to exclude white-coat and masked hypertension (more common in pregnancy)
- Urine protein at each visit — early detection of superimposed preeclampsia
- Fetal surveillance: Serial growth ultrasounds (every 4 weeks from 28 weeks), umbilical artery Doppler, non-stress tests
- Labs: Renal function, LFTs, CBC, uric acid
Delivery Planning
| Scenario | Timing |
|---|---|
| Well-controlled chronic HTN, no complications | 38–39 weeks |
| Poorly controlled or with superimposed preeclampsia | Earlier delivery; individualized |
| Severe features (SBP ≥160 or DBP ≥110, organ damage) | Expedite delivery after stabilization |
Postpartum Considerations
- BP often rises 3–6 days postpartum — close monitoring required
- Resume or initiate antihypertensives as needed; most are compatible with breastfeeding (labetalol, nifedipine, methyldopa)
- ACE inhibitors (e.g., enalapril, captopril) are acceptable postpartum and in breastfeeding
- Evaluate for secondary causes postpartum if not done previously
- Long-term: chronic hypertension persists — ongoing cardiovascular risk management
This is a shared conversation. Sign in to Orris to start your own chat.