Anemia case discusssion in community medicnie
"anemia" AND "community" AND "India"
Anaemia Mukt Bharat programme targets interventions 2025
Anemia - Case Discussion in Community Medicine
CASE VIGNETTE
- Breathlessness on walking short distances (3 months)
- Easy fatigability and weakness
- Pallor of palms and conjunctivae
- No fever, no bleeding episodes, no jaundice
PART 1: DIAGNOSIS
WHO Diagnostic Cut-offs for Anaemia
| Population Group | Hb Cut-off (g/dL) | MCHC |
|---|---|---|
| Adult males | < 13 | < 34% |
| Adult females (non-pregnant) | < 12 | < 34% |
| Pregnant women | < 11 | < 34% |
| Children 6 months - 6 years | < 11 | < 34% |
| Children 6 - 14 years | < 12 | < 34% |
- Hb 10-11 g/dL = Early (mild) anaemia
- Hb < 10 g/dL = Marked (moderate-severe) anaemia
Working Diagnosis
PART 2: DEFINITION
"A condition in which the haemoglobin content of blood is lower than normal as a result of a deficiency of one or more essential nutrients, regardless of the cause of such deficiency."
PART 3: THE EPIDEMIOLOGICAL PROBLEM
Global Burden
- Affects nearly two-thirds of pregnant and one-half of non-pregnant women in developing countries
- Even in developed countries, 4-12% of reproductive-age women are anaemic
India - A National Emergency
- Iron deficiency anaemia is the most widespread micronutrient deficiency in India, cutting across all age groups, castes, and religions
- 72.7% of urban children under 3 years are anaemic; 81.2% of rural children are anaemic
- Prevalence increased from 74.2% (1998-99) to 79.2% (2005-06) for children
- 19% of maternal deaths in India are due to anaemia
- Adolescent girls: 72.6% prevalence (DLHS 2002-04); severe anaemia 21.1%
- Bihar had the highest prevalence (87.6%); Punjab the lowest
High-Risk Groups
- Pregnant and lactating women
- Women of reproductive age (15-49 years)
- Children 6-35 months
- Adolescent girls (10-19 years)
- Low socio-economic strata
PART 4: CAUSES / ETIOLOGY
Primary Cause in Community Settings
| Cause | Mechanism |
|---|---|
| Poor dietary intake | Diets predominantly cereal-based; low in haem iron |
| Poor bioavailability | < 5% of dietary iron absorbed from plant sources |
| Increased demand | Pregnancy, lactation, rapid childhood growth, adolescence |
| Menstrual blood loss | Women lose significant iron each cycle |
| Malaria | Hemolysis and sequestration of RBCs |
| Hookworm infestation | Chronic intestinal blood loss |
| Close-interval pregnancies | Cumulative depletion of iron stores |
| Folate deficiency | Megaloblastic anaemia (especially pregnant women, poor families) |
Key point: Poor bioavailability of iron from the habitual Indian diet (cereal-based, high in phytates) is considered a major reason for widespread iron deficiency even when total intake appears adequate.
PART 5: EVALUATION OF IRON STATUS
| Parameter | Normal | Deficiency Indicator |
|---|---|---|
| Haemoglobin | As per age/sex (Table above) | Below cut-off = anaemia |
| Serum iron | 0.80-1.80 mg/L | < 0.50 mg/L = probable IDA |
| Serum ferritin | > 12 mcg/L | < 10 mcg/L = absent stores |
| Serum transferrin saturation | ~30% | < 16% = deficiency |
| MCHC | 34% | < 34% = hypochromic RBCs |
PART 6: DETRIMENTAL EFFECTS (Consequences)
(a) Pregnancy
- Increased risk of maternal and fetal mortality and morbidity
- 19% of maternal deaths in India attributable to anaemia
- Abortions, premature births, postpartum haemorrhage, low birth weight
(b) Infection
- Anaemia can be caused/aggravated by malaria and intestinal parasites
- Iron deficiency impairs cellular immunity and immune function
- Increased susceptibility to infections
(c) Work Capacity & Productivity
- Even mild anaemia causes significant impairment of maximal work capacity
- More severe anaemia = greater reduction in productivity
- Major economic impact on the country
PART 7: MANAGEMENT (Community Level)
Eligibility Criteria for IFA Supplementation
- Hb 10-12 g/dL: Daily IFA supplementation
- Hb < 10 g/dL: Refer to nearest PHC for further management
National Nutritional Anaemia Prophylaxis Programme (NNAPP)
IFA Dosage Schedule
| Beneficiary | Elemental Iron | Folic Acid | Duration |
|---|---|---|---|
| Pregnant/Lactating women | 100 mg/day (300 mg ferrous sulphate) | 0.5 mg/day | Until Hb normal + 2-3 months |
| Children 6-60 months | 20 mg/day (liquid formulation) | 0.1 mg/day | 100 days |
| School children | Age-appropriate tablet | - | Periodically |
- Haemoglobin should be re-checked every 3-4 months
- If Hb < 10 g/dL (severe): refer for blood transfusion or high-dose parenteral iron
PART 8: NATIONAL PROGRAMMES
1. National Nutritional Anaemia Prophylaxis Programme (NNAPP) - 4th Five Year Plan
2. National Iron Plus Initiative (NIPI)
3. Weekly Iron and Folic Acid Supplementation (WIFS)
4. Anaemia Mukt Bharat (AMB) Programme - 2018 (6×6×6 Strategy)
- Pre-school children (6-59 months)
- Children 5-9 years
- Adolescent boys and girls (10-19 years)
- Pregnant women
- Lactating women
- Women of reproductive age (15-49 years)
- Prophylactic IFA supplementation (age-specific)
- Periodic deworming (bi-annual)
- Intensified year-round behaviour change and communication (BCC)
- Testing of anaemia with point-of-care devices
- Mandatory provision of IFA in programmes (ICDS, mid-day meal, NHM)
- Addressing non-nutritional causes (malaria, haemoglobinopathies, fluorosis)
- Ministry-level convergence, dashboards, real-time monitoring, AMB index
PART 9: PREVENTION STRATEGIES
1. Iron and Folic Acid Supplementation
2. Iron Fortification
- Addition of ferric orthophosphate or ferrous sulphate with sodium bisulphate to salt (double-fortified salt)
- When consumed for 12-18 months, significantly reduces anaemia prevalence
- Accepted by Government of India as a public health approach; commercial production since 1985
- Advantage: salt is universally consumed - benefits all segments; no special delivery system needed
3. Other Strategies (Long-term)
- Dietary diversification and nutrition education
- Control of intestinal parasites (deworming)
- Malaria control
- Behaviour change communication
PART 10: OTHER TYPES OF ANAEMIA IN COMMUNITY MEDICINE
Sickle Cell Anaemia
- Autosomal recessive disorder; point mutation in DNA causes abnormal Hb S
- Heterozygous = clinically healthy (sickle cell trait)
- Homozygous = chronic haemolytic anaemia; death often before puberty
- Prevalent in sub-Saharan Africa and certain regions of India
- Rate of sickling influenced by concentration of HbS in RBC
- Associated with malaria-endemic areas (malaria provides heterozygote advantage)
- Management: supportive; prenatal diagnosis available by DNA analysis; genetic counselling
Thalassaemia
- Hereditary disorder with reduced synthesis of globin chain (alpha or beta)
- Produces hypochromic microcytic anaemia due to defective haemoglobinization
- Community approach: carrier screening, genetic counselling, prenatal diagnosis
Megaloblastic / Folic Acid Deficiency Anaemia
- Folate deficiency anaemia occurs in pregnant women from low-income groups
- Sub-clinical folate deficiency reported in ~30% of pregnant women in rural North India
- Microcytic anaemia (from iron deficiency) can mask concurrent megaloblastic anaemia
PART 11: SUMMARY TABLE FOR EXAM - CASE APPROACH
| Step | Action |
|---|---|
| 1. Detect | Pallor (conjunctiva, palms, nail beds), breathlessness, fatigue |
| 2. Diagnose | Hb estimation; classify severity by WHO cut-offs |
| 3. Investigate | Peripheral smear, serum ferritin, MCV/MCH, serum iron, TIBC |
| 4. Treat | IFA tablets (Hb 10-12); refer to PHC (Hb < 10) |
| 5. Prevent | IFA prophylaxis, dietary advice, deworming, iron-fortified foods |
| 6. Notify/Report | Link to AMB programme, NHM tracking, HMIS data |
| 7. Community-level | ASHA-led screening, AWC-based delivery, school deworming, VHND |
RECENT EVIDENCE
- Park's Textbook of Preventive and Social Medicine (Park's PSM), pp. 719-720, 738-740
- Government of India - Anaemia Mukt Bharat (PIB)
- AMB Index Study, Global Health: Science and Practice, 2018-2023
Make a visual poster on the 6×6×6 Anaemia Mukt Bharat strategy
A professional medical education poster titled "Anaemia Mukt Bharat - 6×6×6 Strategy" with a clean, vibrant design on a white background with red and orange accent colors representing India's health mission. Layout: Three main columns side by side, each with a bold header: COLUMN 1 - "6 TARGET GROUPS (Life Cycle Approach)" with a lifecycle/human silhouette icon, listing: 1. Pre-school children (6–59 months) 2. Children (5–9 years) 3. Adolescent Girls & Boys (10–19 years) 4. Pregnant Women 5. Lactating Women 6. Women of Reproductive Age (15–49 years) COLUMN 2 - "6 KEY INTERVENTIONS" with a medical cross icon, listing: 1. Prophylactic IFA Supplementation 2. Periodic Deworming (bi-annual) 3. Behaviour Change Communication (BCC) 4. Point-of-Care Testing (HemoCue) 5. Mandatory IFA in Programmes (ICDS, NHM) 6. Addressing Non-Nutritional Causes (malaria, haemoglobinopathies) COLUMN 3 - "6 INSTITUTIONAL MECHANISMS" with a government/gear icon, listing: 1. Ministry-level convergence 2. Real-time monitoring & dashboard 3. District-level planning 4. AMB Index tracking 5. Convergence with POSHAN Abhiyaan 6. Community mobilization via ASHA/AWC Below the three columns, a bold red banner: "TARGET: Reduce Anaemia by 3% per year | T3 Approach: TEST · TREAT · TALK" At the top: India map outline with a red drop of blood, the text "Anaemia Mukt Bharat" in large bold red font, "Launched 2018 under POSHAN Abhiyaan" in smaller text, and a tagline "A Life Cycle Approach to Eliminate Anaemia" Footer: WHO Hb cut-offs table mini-graphic and the text "National Iron Plus Initiative (NIPI) | WIFS | NNAPP" Overall style: clean infographic poster, medical/public health educational style, bold icons for each point, color-coded columns (red, orange, maroon), easy to read at a glance.
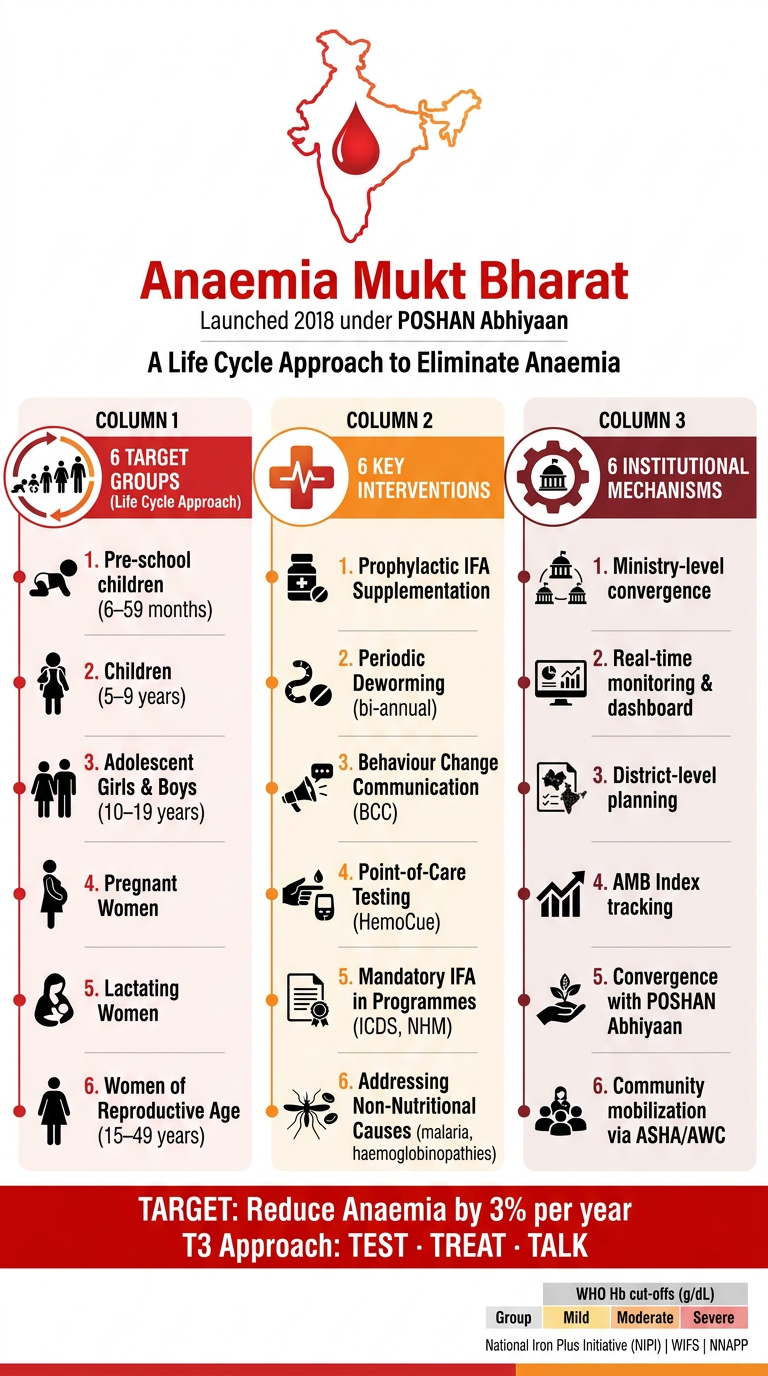
- Column 1 - The 6 target population groups following a life cycle approach (from pre-school children to women of reproductive age)
- Column 2 - The 6 key programmatic interventions (IFA supplementation, deworming, BCC, point-of-care testing, mandatory IFA delivery, and addressing non-nutritional causes)
- Column 3 - The 6 institutional mechanisms (ministry convergence, real-time dashboards, AMB Index, POSHAN Abhiyaan linkage, and community mobilization via ASHA/AWC)
- Bottom banner - The core target (3% annual reduction in anaemia) and the T3 Approach: Test · Treat · Talk
Search for latest Anaemia Mukt Bharat Index performance across Indian states
Anaemia Mukt Bharat Index 2024 2025 state rankings performance India
"Anemia Mukt Bharat" AND "index" AND "states"
https://theprint.in/india/madhya-pradesh-top-in-country-in-a…
PMID: 41371944
Anaemia Mukt Bharat scorecard 2025-26 full state rankings all states list
Anaemia Mukt Bharat (AMB) Index - Latest State Performance
What is the AMB Index?
- Children aged 6-59 months
- Children aged 5-9 years
- Adolescents aged 10-19 years
- Pregnant women
- Lactating mothers
AMB Scorecard 2025-26 - Annual Rankings (Published May 2025)
| Rank | State | AMB Index Score | Key Highlights |
|---|---|---|---|
| 1 | Madhya Pradesh | 92.1 | Overtook AP from last year; all 52 districts reported fully for 12 months |
| 2 (Joint) | Andhra Pradesh | 90.6 | Ranked 1st last year |
| 2 (Joint) | Telangana | 90.6 | Consistent top performer |
| 3 | Tamil Nadu | 89.9 | - |
- Children 6-59 months: 80.4%
- Children 5-9 years: 95%
- Adolescents: 95%
- Pregnant women: 95%
- Lactating mothers: 95%
- Uttar Pradesh: 74 of 75 districts in incomplete/non-reporting category
- Rajasthan: Dropped from 19th to 23rd position
AMB Scorecard Q1 2025-26 (April-June 2025) - Quarterly Rankings
| Rank | State | AMB Index Score |
|---|---|---|
| 1 | Andhra Pradesh | 88.0 |
| 2 | Haryana | 85.2 |
| 3 | Telangana | 82.5 |
| - | UP | 49.0 |
| - | Bihar | 47.6 |
| National Average | All India | 56.6 |
- Climbed from 3rd to 2nd place
- Children 6 months - 5 years coverage: 90.5% (vs. 87.2% previous year)
- More than double the national average of 38.7% for this group
National Trend: IFA Coverage 2018-2023 (Peer-Reviewed Data)
| Year | National IFA Coverage (AMB Index) |
|---|---|
| 2018-19 | 35.5% |
| 2022-23 | 57.6% |
| Increase | +22.1 percentage points |
Summary: Top vs. Bottom Performers at a Glance
| Category | States |
|---|---|
| Consistent top performers | Madhya Pradesh, Andhra Pradesh, Telangana, Tamil Nadu, Haryana |
| Improving states | Haryana (climbed from 3rd to 2nd in Q1 2025-26) |
| Slipping states | Rajasthan (dropped from 19th to 23rd, 2025-26) |
| Chronic laggards | Uttar Pradesh (~49 pts), Bihar (~47.6 pts) |
| National average | ~56.6 (Q1 2025-26) |