Hypertension cause kidney damge how to what is science behind it in logical
Reading File
search_medical_text
hypertension kidney damage pathophysiology mechanisms
search_medical_text
hypertensive nephrosclerosis glomerular damage renin angiotensin system
search_medical_image
hypertension kidney nephrosclerosis glomerular pathology diagram
GradeResponse
GradeResponse
GradeResponse
Here is a logical, step-by-step breakdown of the science behind how hypertension damages the kidneys.
How Hypertension Damages the Kidneys — The Science
Step 1: The Kidney's Normal Pressure Management
The kidney filters blood through tiny, delicate capillary tufts called glomeruli. Each glomerulus is fed by an afferent arteriole (incoming) and drained by an efferent arteriole (outgoing). The pressure inside the glomerulus is tightly regulated — normally around 45–60 mmHg — so that filtration happens efficiently without physically destroying the capillary walls.
To protect glomeruli from high systemic blood pressure, the afferent arteriole automatically constricts. This is called autoregulation.
Step 2: Autoregulation Fails Under Sustained High Pressure
When blood pressure is chronically elevated, this protective autoregulatory mechanism becomes overwhelmed and eventually breaks down. High pressure is transmitted directly into the glomerular capillaries — a state called glomerular hypertension.
This is the central insult. The capillary walls face mechanical stress they were never designed to withstand.
Step 3: Mechanical Injury to Blood Vessel Walls
The sustained high pressure causes structural damage to the small arteries and arterioles feeding the kidney:
| Vessel | What Happens |
|---|---|
| Afferent arterioles | Wall thickens; hyaline material (plasma proteins) is deposited — called hyaline arteriolosclerosis |
| Interlobular & arcuate arteries | Fibrous tissue replaces smooth muscle — fibromuscular hyperplasia |
| Efferent arterioles | Less affected but contribute to downstream ischemia |
According to Harrison's Principles of Internal Medicine (p. 7647): "Atherosclerotic, hypertension-related vascular lesions in the kidney primarily affect preglomerular arterioles, resulting in ischemic changes in the glomeruli and postglomerular structures."
Step 4: Glomerular Injury — Two Parallel Pathways
Pathway A — Ischemic injury (from narrowed arterioles):
- Narrowed arterioles reduce blood flow to glomeruli
- Glomeruli become starved of oxygen → ischemic glomerulosclerosis
- Affected glomeruli scar over and stop functioning
Pathway B — Hyperfiltration injury (direct pressure damage):
- Where autoregulation fails, high pressure stretches the glomerular capillaries
- This activates mesangial cells and podocytes (the glomerular filter cells)
- They produce TGF-β (Transforming Growth Factor-Beta) and other fibrotic signals
- The glomerular basement membrane thickens and eventually collapses — focal segmental glomerulosclerosis (FSGS)
Step 5: The Renin-Angiotensin-Aldosterone System (RAAS) Makes It Worse
Ischemic kidney tissue responds by releasing renin from the afferent arteriole wall. Renin triggers the RAAS cascade:
Renin → Angiotensin I → Angiotensin II (via ACE) → Aldosterone
Per Harrison's (p. 8432), Angiotensin II:
- Constricts the efferent arteriole, raising filtration fraction and glomerular pressure further
- Stimulates aldosterone, causing salt and water retention — raising blood pressure even more
- Directly damages tubular cells and promotes fibrosis via TGF-β
This creates a vicious cycle: hypertension → kidney ischemia → RAAS activation → more hypertension → more kidney damage.
Step 6: Tubular and Interstitial Damage
As glomeruli scar, the downstream tubules they feed also die. This is called tubular atrophy. Surrounding tissue fills with collagen — interstitial fibrosis. The kidney gradually shrinks and loses functioning nephrons.
Step 7: The Endgame — Hypertensive Nephrosclerosis
The final histological (microscopic) picture is called hypertensive nephrosclerosis:
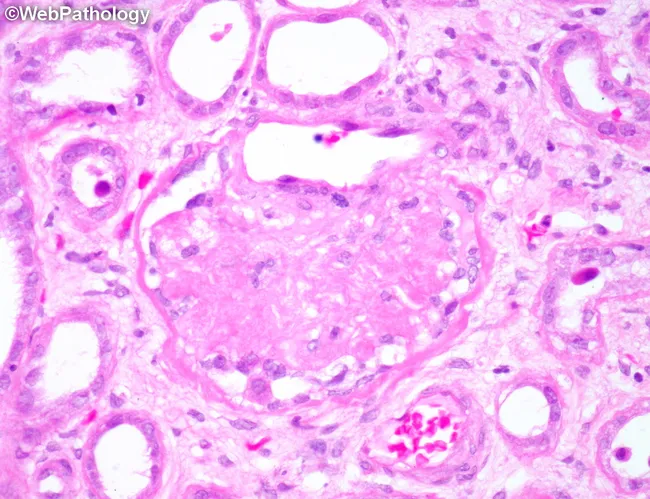
Renal biopsy (H&E stain): A globally sclerotic glomerulus with obliterated capillary lumina, hyaline arteriolosclerosis of arterioles, tubular atrophy, and mild interstitial fibrosis — the hallmark of benign hypertensive nephrosclerosis. (Source: WebPathology)
The Full Logical Chain — Summary
Chronic High BP
↓
Afferent arteriole autoregulation overwhelmed
↓
High pressure enters glomerulus (glomerular hypertension)
↓
┌─────────────────────────────────────────┐
↓ ↓
Arteriole wall thickening Mechanical stretch of
(hyaline arteriolosclerosis) glomerular capillaries
↓ ↓
Reduced blood flow Podocyte/mesangial activation
(ischemia) → TGF-β → fibrosis (FSGS)
↓
Kidney releases Renin → RAAS activated
↓
Angiotensin II → efferent constriction + aldosterone
↓
More sodium/water retention → BP rises further
↓
Tubular atrophy + Interstitial fibrosis
↓
Loss of nephrons → ↓GFR → Chronic Kidney Disease (CKD)
Key Takeaway
The damage is not from one single event. It is a mechanical + hormonal + fibrotic cascade: high pressure physically injures vessels and glomeruli, the kidney's own hormonal response (RAAS) amplifies both the blood pressure and the injury, and the scarring that follows is largely irreversible. This is why blood pressure control — especially with ACE inhibitors or ARBs (which block Angiotensin II) — is the primary strategy to slow hypertensive kidney disease.
More logical answer in easy words
search_medical_text
hypertension chronic kidney disease progression glomerular pressure
search_medical_image
glomerulus filtration hypertension damage illustration
GradeResponse
GradeResponse
How High Blood Pressure Slowly Destroys Your Kidneys — In Simple Words
First, Understand What the Kidney Actually Does
Think of your kidney as a water treatment plant. Every minute, about 1.2 litres of blood flows through it. Inside the kidney are about 1 million tiny filters called glomeruli (say: glo-MER-you-lie). Each one is basically a tiny ball of fragile capillaries (hair-thin blood vessels) that squeeze out waste from your blood, like a coffee filter.
For this filter to work safely, the pressure inside it must stay low and steady — around 45–60 mmHg.
Now, What Happens When Blood Pressure is High?
Imagine your garden hose. If you crank the tap to full power and block the end — the hose stretches, weakens, and eventually bursts. The same thing happens inside your kidney.
The Story — Step by Step
🔴 Step 1: High Pressure Hits the Pipes (Blood Vessels)
Your blood travels to the kidney through small arteries. When blood pressure is persistently high, these vessels experience constant force against their walls — like water always hammering a pipe.
Over time:
- The vessel walls thicken and stiffen to resist the pressure
- A protein called hyaline gets deposited inside the walls, making them hard
- The opening (lumen) of the vessel narrows
Result: Less blood gets through. The kidney tissue starts getting less oxygen — it becomes ischemic (starved).
🔴 Step 2: The Tiny Filters Get Hammered
Normally, the small artery entering each filter (afferent arteriole) squeezes itself to reduce pressure before blood enters the glomerulus. This is the kidney's self-protection system (autoregulation).
But with chronic high blood pressure, this protection breaks down. High pressure enters the glomerulus directly.

The fragile capillaries inside the glomerulus are now being stretched and battered with every heartbeat. Think of blowing too much air into a balloon — eventually the balloon distorts and tears.
Result: The glomerular filter gets damaged. It starts leaking things it shouldn't — like proteins (normally too big to pass through). Protein in urine (proteinuria) is one of the first warning signs.
🔴 Step 3: The Kidney Panics and Makes Things Worse
When the kidney senses reduced blood flow (from narrowed vessels), it thinks the body's blood pressure has dropped — even though it actually hasn't. So it activates its emergency pressure system called the RAAS (Renin-Angiotensin-Aldosterone System):
| Step | What Happens | Effect |
|---|---|---|
| Kidney releases Renin | Signals the body to raise BP | BP goes higher |
| Renin makes Angiotensin II | Squeezes blood vessels tighter | Even more pressure on kidney |
| Angiotensin II triggers Aldosterone | Kidneys retain more salt and water | More fluid = more BP |
This is the vicious cycle:
High BP → Damages kidney vessels
→ Kidney thinks BP is low
→ Releases hormones to RAISE BP
→ BP goes even higher
→ More kidney damage
→ Repeat...
Per Harrison's Principles of Internal Medicine (p. 8514): elevated blood pressure increases protein leakage across glomerular capillaries, and the more protein in urine, the faster kidney function declines.
🔴 Step 4: Filters Scar Over and Die
The damaged glomeruli cannot repair themselves. They scar over — this is called glomerulosclerosis (sclerosis = hardening/scarring). A scarred filter is a dead filter. It no longer cleans blood.
The tubules connected to dead filters also shrink and die (tubular atrophy). The surrounding tissue fills with scar tissue (interstitial fibrosis). The kidney literally shrinks in size.
This is what a kidney biopsy looks like under a microscope after years of high blood pressure — the glomerulus is completely scarred, the vessels are thickened with hyaline, and the tubules have shrunk. (Source: WebPathology)
🔴 Step 5: The Remaining Filters Burn Out
Here is where it gets really cruel. When some filters die, the surviving ones work harder to compensate. They increase their own filtration pressure to handle the extra load.
But this "overworking" causes hyperfiltration injury — the remaining filters wear out faster. It is like having 10 workers, losing 3, and making the remaining 7 do the job of 10 — they exhaust faster.
Result: A downward spiral where kidney function keeps declining even if blood pressure is later controlled.
The Full Story in One Picture
CHRONIC HIGH BLOOD PRESSURE
↓
Small kidney vessels thicken & narrow
↓
Two things happen simultaneously:
┌──────────────────┐ ┌──────────────────────┐
│ Less blood flow │ │ High pressure enters │
│ → Filters starve │ │ filters directly │
│ → Ischemia │ │ → Filters stretch/tear │
└──────────────────┘ └──────────────────────┘
↓ ↓
Kidney panics → releases RAAS hormones
↓
Blood pressure rises FURTHER
↓
More damage → Filters scar over (Nephrosclerosis)
↓
Fewer working filters → Remaining ones overwork
↓
Protein leaks into urine → GFR (filtration) falls
↓
CHRONIC KIDNEY DISEASE (CKD) → Kidney Failure
Why It Feels Like Nothing — Until It's Too Late
The kidneys have enormous reserve capacity. You can lose up to 50% of kidney function and feel completely normal. Symptoms only appear when function drops below 25–30%. This is why hypertension silently destroys kidneys for years before anything is noticed — earning both conditions the nickname "silent killers."
The Simple Fix Logic
Since Angiotensin II is the molecule doing the most damage (squeezing vessels, raising pressure, causing fibrosis), doctors use:
- ACE Inhibitors (e.g., Ramipril) — block Angiotensin II production
- ARBs (e.g., Losartan) — block Angiotensin II from binding
These not only lower blood pressure but directly protect the kidney filters — which is why they are the preferred drugs in hypertensive kidney disease.
This is a shared conversation. Sign in to Orris to start your own chat.