Emypmea
Wnpywma thoracis
"empyema thoracis"[MeSH Terms] AND management
Empyema Thoracis
Definition
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- S. Das - A Manual on Clinical Surgery
Stages / Pathogenesis
| Stage | Features | Pleural Fluid |
|---|---|---|
| 1. Exudative | Rapid sterile fluid outpouring; increased permeability | Low WBC, low LDH, normal glucose and pH |
| 2. Fibropurulent | Bacteria invade; leukocytes, fibrin, and loculations form | Low pH and glucose; high LDH |
| 3. Organizational | Pleural surfaces thicken into a "pleural peel" | Thick pus and cellular debris |
- Murray & Nadel's Textbook of Respiratory Medicine
Etiology & Risk Factors
- Contiguous spread from intrapulmonary infection (most common) - parapneumonic
- Hematogenous or lymphatic dissemination
- Direct transdiaphragmatic spread from subdiaphragmatic or liver abscess (more common on the right)
- Esophageal perforation, chest trauma, post-surgical complications, lung transplant complications
- Rupture of a peripheral lung abscess into the pleural space
- Community-acquired: Streptococcus milleri group, Streptococcus pneumoniae, anaerobes (reflecting oropharyngeal flora)
- Hospital-acquired: Staphylococcus aureus (including MRSA), Gram-negative organisms (E. coli, Klebsiella, Pseudomonas)
Clinical Presentation
- Difficult to distinguish from pneumonia: fever, cough, dyspnea, malaise, pleuritic chest pain (often prolonged)
- Many patients with pneumonia develop a parapneumonic effusion without a change in symptoms
| Type | Criteria |
|---|---|
| Uncomplicated | Glucose >40 mg/dL, pH >7.2, negative Gram stain/culture, no loculations |
| Complicated | Glucose <40 mg/dL OR pH <7.2 OR loculated on ultrasound |
| Frank empyema | Gross pus on aspiration |
Diagnosis
- Chest X-ray: confirms pleural effusion; may show loculation or shift
- Ultrasound: best bedside tool - identifies loculations, guides safe aspiration
- CT chest: better delineates loculations, pleural thickening, underlying lung pathology
- Thoracocentesis: diagnostic and therapeutic - send for pH, glucose, LDH, protein, Gram stain, culture (aerobic + anaerobic)
Types
Treatment
- Adequate pus drainage with a closed tube (not early open drainage)
- Obliteration of the pleural space
- Proper nutritional support
- Antibiotics
| Stage | Management |
|---|---|
| Exudative | Antibiotics alone usually sufficient |
| Fibropurulent | Chest tube drainage (intercostal tube thoracostomy); intrapleural fibrinolytics (streptokinase/tPA + DNase) if loculated |
| Organizational | Surgical: VATS decortication (preferred) or open thoracotomy; thoracoplasty for refractory cases |
Complications
- Bronchopleural fistula
- Empyema necessitatis - pus burrows through the chest wall to the subcutaneous tissue
- Fibrothorax - dense fibrous adhesions obliterating the pleural space, restricting pulmonary expansion
- Septicaemia, metastatic abscess formation
Prognosis / Epidemiology
- Murray & Nadel's Textbook of Respiratory Medicine
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- S. Das - A Manual on Clinical Surgery, 13th Edition
- Tintinalli's Emergency Medicine
Diagram
Medical diagram of Empyema Thoracis showing: 1. A cross-section of the thoracic cavity with labeled anatomy (lung, pleural space, visceral pleura, parietal pleura, chest wall, diaphragm) 2. Three stages shown in separate panels: - Stage 1 Exudative: sterile fluid accumulation in pleural space, clear fluid - Stage 2 Fibropurulent: bacteria invading, fibrin deposits, loculations forming, yellow-green pus - Stage 3 Organizational: thick pleural peel forming around lung, trapped lung 3. Routes of infection shown with arrows: parapneumonic (from lung), hematogenous, transdiaphragmatic (from subdiaphragmatic abscess), esophageal perforation 4. A small inset showing Empyema Necessitatis - pus burrowing through chest wall 5. Clean, professional medical illustration style with clear labels, color-coded stages, white background
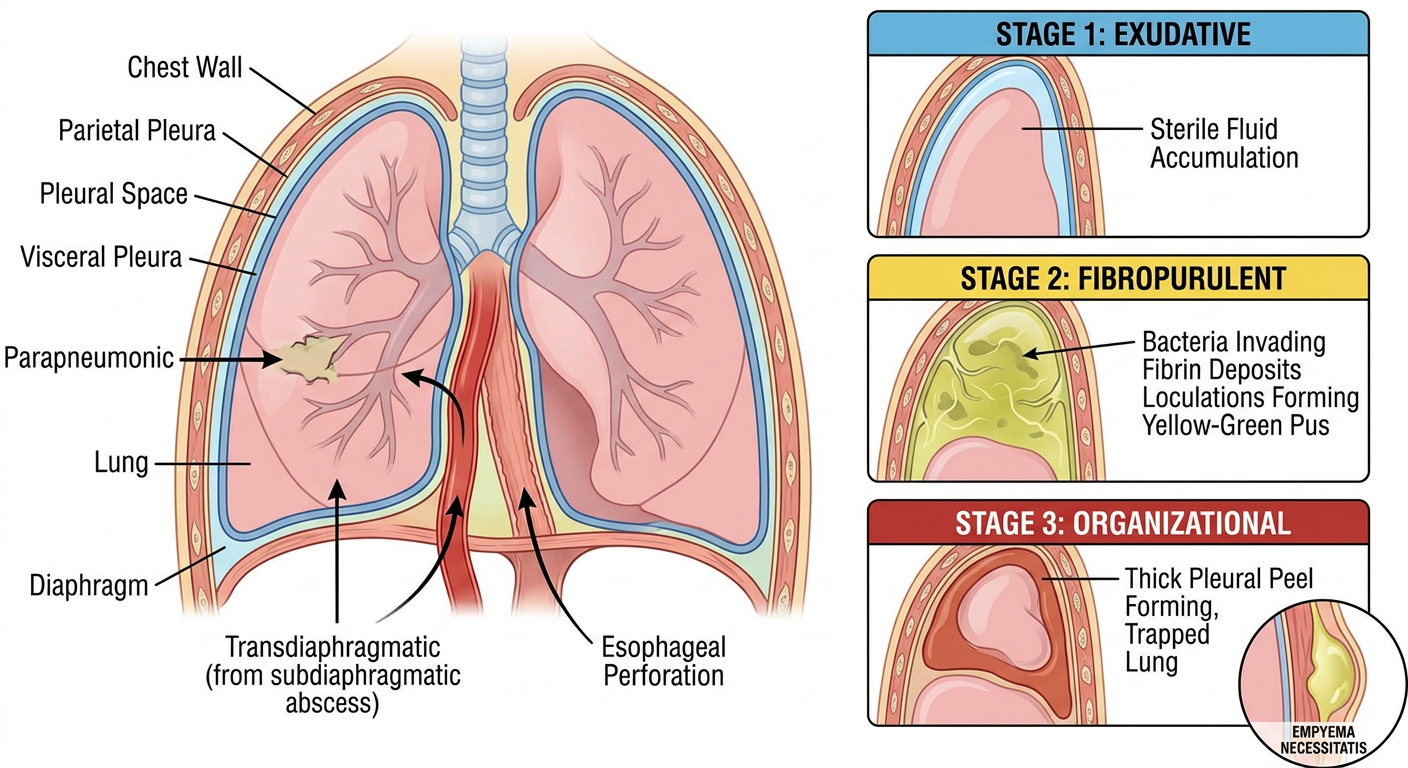
- Thoracic cross-section with key anatomical structures (lung, visceral/parietal pleura, chest wall, diaphragm)
- Three stages of empyema development - exudative (sterile fluid), fibropurulent (pus + loculations + fibrin), and organizational (pleural peel trapping the lung)
- Routes of infection - parapneumonic (from lung), hematogenous, transdiaphragmatic (from subdiaphragmatic abscess), and esophageal perforation
- Empyema necessitatis inset - showing pus burrowing through the chest wall into subcutaneous tissue