Meningitis tried
Reading File
search_medical_text
meningitis etiology diagnosis clinical features management
search_medical_image
meningitis imaging CSF findings brain CT MRI
GradeResponse
GradeResponse
Meningitis
Meningitis is inflammation of the meninges (the membranes surrounding the brain and spinal cord), most commonly caused by infection. It is a medical emergency.
Etiology
The causative agent varies by age and immune status (Harrison's, p. 14669):
| Category | Common Pathogens |
|---|---|
| Neonates | Group B Streptococcus, E. coli, Listeria monocytogenes |
| Children/Adults | Streptococcus pneumoniae, Neisseria meningitidis, H. influenzae |
| Elderly/Immunocompromised | L. monocytogenes, gram-negatives |
| Viral (Aseptic) | Enteroviruses, HSV-2, mumps, HIV |
| Fungal | Cryptococcus neoformans (esp. HIV patients), Candida |
| Tuberculous | Mycobacterium tuberculosis |
Pathophysiology
Organisms reach the meninges via hematogenous spread or direct extension. Once in the subarachnoid space, bacterial components trigger a robust inflammatory cascade, leading to:
- Increased intracranial pressure (ICP)
- Cerebral edema
- Impaired CSF resorption → hydrocephalus
- Vasculitis and cortical injury
Clinical Features
The classic triad (present together in only ~44% of cases):
- Fever
- Nuchal rigidity (neck stiffness)
- Altered mental status / headache
Additional signs:
- Kernig's sign: resistance to knee extension with hip flexed
- Brudzinski's sign: involuntary hip/knee flexion on neck flexion
- Photophobia, phonophobia
- Petechial/purpuric rash — classic for meningococcal disease (medical emergency)
- Seizures, focal neurological deficits (in complicated cases)
Diagnosis
Step 1 — CT Head Before LP?
Obtain CT first if any of:
- Papilledema
- Focal neurological deficits
- Severely altered consciousness / new-onset seizures
- Immunocompromised state
Do NOT delay antibiotics waiting for CT or LP!
Step 2 — Lumbar Puncture (CSF Analysis)
| Parameter | Bacterial | Viral | Tuberculous | Fungal |
|---|---|---|---|---|
| Appearance | Turbid/cloudy | Clear | Clear/xanthochromic | Clear/cloudy |
| WBC | >1000 (PMNs) | <500 (lymphs) | 100–500 (lymphs) | <500 (lymphs) |
| Protein | ↑↑ (>100 mg/dL) | Mildly ↑ | ↑↑ | ↑ |
| Glucose | ↓↓ (<40 mg/dL) | Normal | ↓ | ↓ |
| Opening pressure | ↑↑ | Normal/↑ | ↑ | ↑↑ |
| Gram stain/Culture | Positive ~70–80% | Negative | Negative (ZN stain) | India ink/CrAg |
Additional tests:
- Blood cultures (×2 before antibiotics if possible)
- Serum glucose (for CSF:serum ratio)
- CBC, CMP, CRP, procalcitonin
- PCR panels (HSV, enterovirus) on CSF
- Cryptococcal antigen (CrAg) in immunocompromised
Imaging
MRI with gadolinium is the imaging modality of choice when complications are suspected:
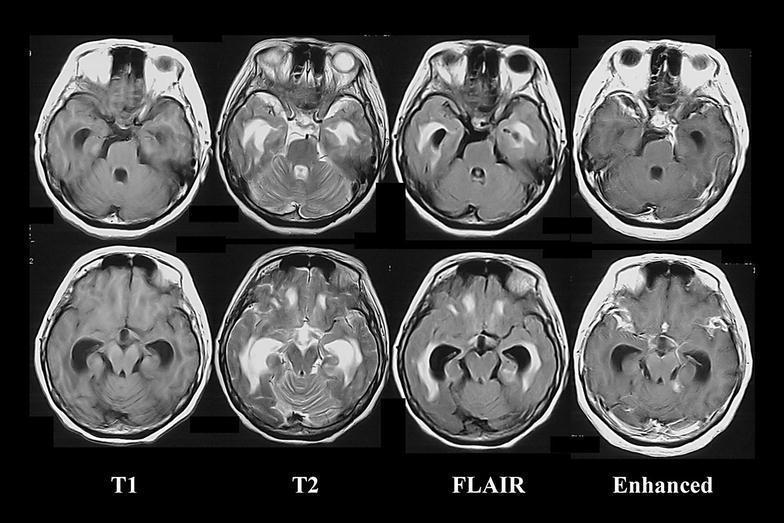
Multi-parametric MRI showing basal meningitis with communicating hydrocephalus, periventricular white matter changes on T2/FLAIR, and diffuse leptomeningeal enhancement on gadolinium sequences — characteristic of tuberculous or cryptococcal meningitis.
Management
Empiric Antibiotic Therapy (start immediately)
| Patient Group | Empiric Regimen |
|---|---|
| Adults 18–50 | Ceftriaxone 2g IV q12h + Vancomycin |
| >50 yrs / immunocompromised | + Ampicillin (covers Listeria) |
| Neonates | Ampicillin + Cefotaxime (or Gentamicin) |
| Penicillin allergy | Chloramphenicol or Meropenem |
Adjust based on culture/sensitivity results.
Adjunctive Dexamethasone
- Dexamethasone 0.15 mg/kg IV q6h × 4 days — start with or before first antibiotic dose
- Proven benefit in pneumococcal meningitis (reduces mortality, neurological sequelae)
- Benefit in other bacterial meningitis is less clear
Antiviral (if HSV suspected)
- Acyclovir 10 mg/kg IV q8h — start empirically if encephalitis is possible
Antifungal (Cryptococcal)
- Induction: Liposomal amphotericin B + Flucytosine × 2 weeks
- Consolidation: Fluconazole × 8 weeks
Supportive Care
- Strict neuro monitoring (GCS, pupils)
- ICP management (head of bed 30°, osmotherapy if needed)
- Seizure prophylaxis/treatment
- Fever control, fluid balance
- Isolation precautions for meningococcal disease (droplet)
Complications
| Complication | Notes |
|---|---|
| Hydrocephalus | May require EVD placement |
| SIADH / hyponatremia | Common, monitor Na⁺ closely |
| Subdural empyema | Neurosurgical emergency |
| Cerebral venous sinus thrombosis | MRV to diagnose |
| Hearing loss | Especially post-pneumococcal; audiological follow-up |
| Cognitive impairment, seizures | Long-term sequelae |
| Waterhouse-Friderichsen syndrome | Adrenal hemorrhage in meningococcemia |
| Death | Bacterial meningitis mortality ~20–30% without treatment |
Prophylaxis
- Meningococcal contacts: Rifampin 600 mg PO q12h × 2 days, or Ciprofloxacin single dose, or Ceftriaxone IM single dose
- Vaccination: MenACWY, MenB vaccines; PCV13/PPSV23 for pneumococcal; Hib vaccine
Prognosis
Bacterial meningitis carries significant morbidity/mortality. Prognosis worsens with:
- Delayed treatment
- Extremes of age
- Impaired consciousness at presentation
- Pneumococcal etiology
- Gram-negative organisms (Harrison's, p. 14669)
Viral meningitis is generally self-limiting with good outcomes. Tuberculous and fungal meningitis require prolonged therapy and carry higher morbidity.
This is a shared conversation. Sign in to Orris to start your own chat.