Spirometry
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to give a thorough answer on spirometry. Let me compile the full response.
Spirometry
Spirometry is the fundamental pulmonary function test (PFT) that measures the volume and flow of air during breathing maneuvers. It is performed using a pneumotachometer (measures flow, integrates to derive volume) or a volume-based spirometer.
Lung Volumes and Capacities
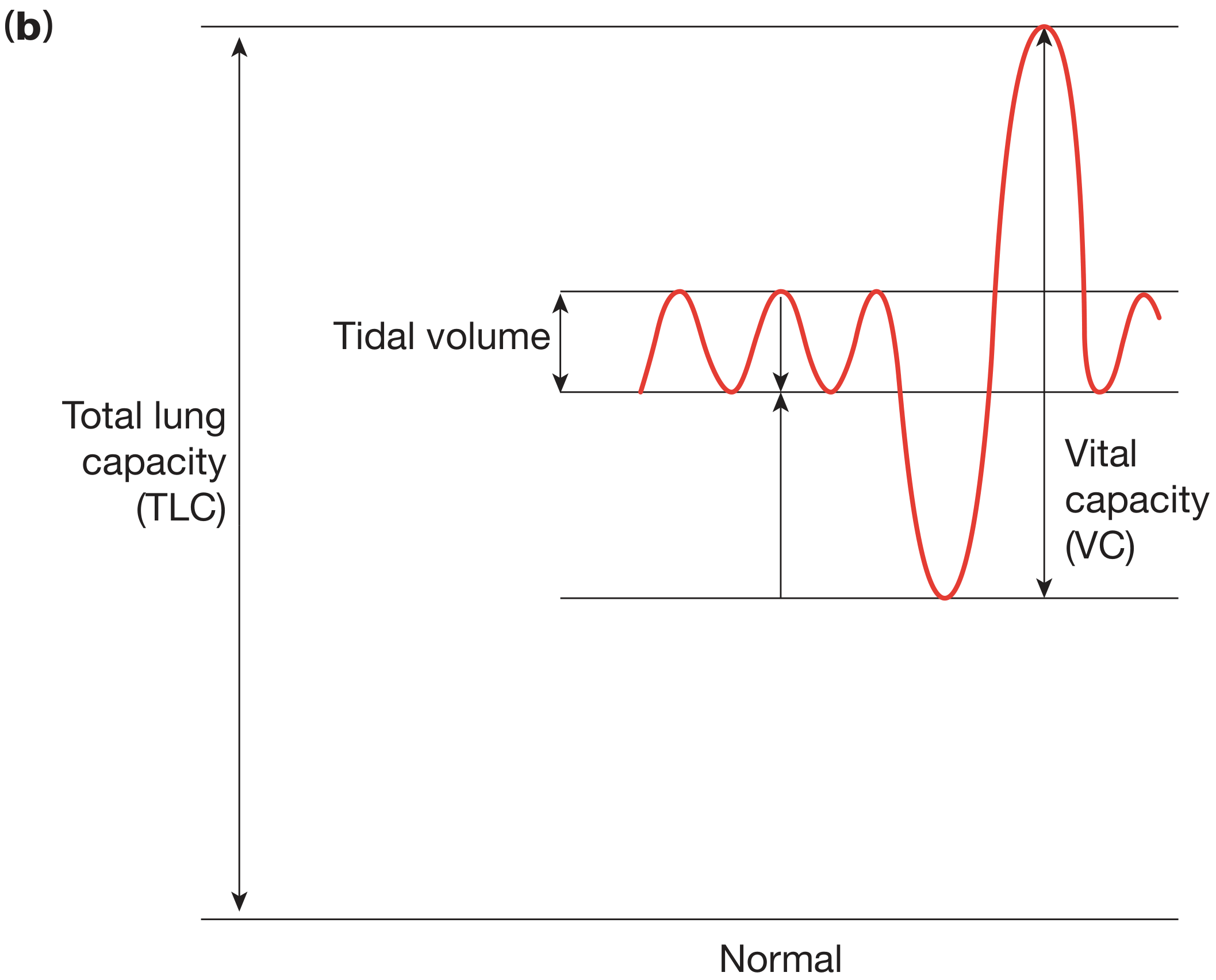
| Term | Definition |
|---|---|
| Tidal Volume (VT) | Volume inhaled/exhaled per normal breath |
| Inspiratory Reserve Volume (IRV) | Max extra volume inhaled from end-inspiration |
| Expiratory Reserve Volume (ERV) | Max extra volume exhaled from end-expiration |
| Residual Volume (RV) | Air remaining after maximal exhalation (not measurable by spirometry alone) |
| Vital Capacity (VC) | Max volume exhaled after maximal inspiration |
| Total Lung Capacity (TLC) | All gas in lungs at maximal inspiration (requires body plethysmography or gas dilution) |
| Functional Residual Capacity (FRC) | Volume at resting end-expiration |
| Inspiratory Capacity (IC) | Max volume inspired from resting expiratory level |
- Murray & Nadel's Textbook of Respiratory Medicine, Figure 31.2
Key Spirometric Parameters
The FVC Maneuver
The subject inhales maximally to TLC, then exhales as rapidly and forcefully as possible. This generates the volume-time curve (FVC curve) and the flow-volume loop.
| Parameter | Description | Normal |
|---|---|---|
| FVC (Forced Vital Capacity) | Total volume exhaled forcefully | Predicted by age, sex, height, ethnicity |
| FEV1 | Volume exhaled in the first 1 second | >80% predicted |
| FEV1/FVC ratio | Key obstructive index | ≥0.70 (GOLD) or above lower limit of normal (LLN) |
| FEV6 | Volume exhaled in 6 sec; approximates FVC | Valid substitute, easier for severe obstruction |
| FEF25-75% | Mean flow between 25-75% of FVC; reflects small airways | 60-140% predicted (high variability) |
| PEF | Peak expiratory flow | Effort-dependent; used in asthma monitoring |
The first 25-30% of the maximal expiratory maneuver is effort-dependent; the remainder is effort-independent and reflects intrinsic airway properties.
- Murray & Nadel's Textbook of Respiratory Medicine
Technique and Acceptability Criteria
- Patient inhales to TLC, seals lips around mouthpiece
- Forceful, maximal, continuous exhalation to end of breath
- A well-trained technician must communicate clearly - patient cooperation is critical
- Minimum 3 acceptable maneuvers required; two best FVC and FEV1 values should be within 150 mL
- Nose clip must be fitted to prevent air leak (air leak falsely lowers measurements)
- Incomplete exhalation gives falsely low FVC; poor initial effort gives falsely low FEV1
Common technical errors include:
-
Air leak from poorly fitting nose clip or mouthpiece - causes wandering baseline
-
Incomplete expiration - falsely low FVC, spuriously elevated FEF25-75%
-
Poor initial expiratory effort - falsely low FEV1 and FEF25-75%
-
Pfenninger and Fowler's Procedures for Primary Care
Pre-test Preparation
- Stop LABAs at least 12 hours before testing
- Stop short-acting bronchodilators at least 6 hours before testing
- Postbronchodilator spirometry values should be used for diagnosis (especially if obstruction is suspected)
Interpretation: The 3-Step Approach
Step 1: Inspect the flow-volume curve visually
Look for quality of effort and patterns (concavity in obstruction, reduced volumes in restriction, plateau in upper airway obstruction).
Step 2: Assess the FEV1/FVC ratio
- Low FEV1/FVC (<0.70 or <LLN) → suggests obstruction
- Normal FEV1/FVC with low FVC → suggests restriction (confirm with TLC)
Step 3: Use the full algorithm
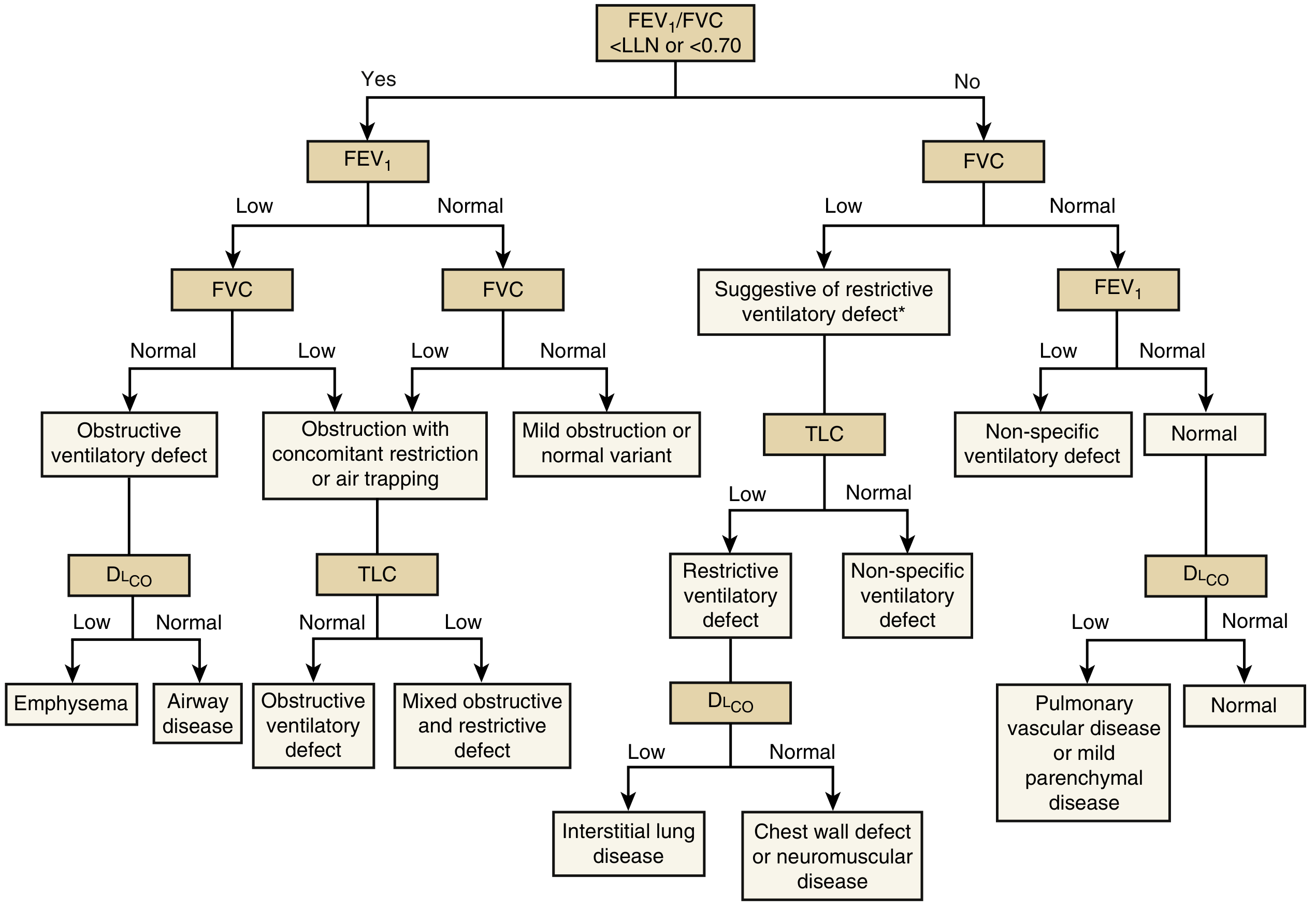
- Murray & Nadel's Textbook of Respiratory Medicine, Figure 32.1
Patterns of Ventilatory Defect
Obstructive Pattern
- FEV1/FVC < 0.70 (GOLD) or < LLN (ATS/ERS)
- FEV1 reduced
- FVC may be normal or reduced (if air trapping or concurrent restriction)
- Flow-volume loop shows concave (scooped) expiratory curve; prolonged expiratory time
- Causes: Asthma, COPD, bronchiectasis, bronchiolitis
- In COPD, typical pattern is irreversible; in asthma, reversible (see below)
GOLD COPD Severity Staging (by FEV1 % predicted, post-bronchodilator):
| GOLD Stage | FEV1 % Predicted |
|---|---|
| GOLD 1 (Mild) | ≥80% |
| GOLD 2 (Moderate) | 50-79% |
| GOLD 3 (Severe) | 30-49% |
| GOLD 4 (Very Severe) | <30% |
Note: Current GOLD guidelines also incorporate symptoms (mMRC/CAT) and exacerbation history for comprehensive staging.
Restrictive Pattern
- FEV1/FVC normal (both FEV1 and FVC reduced proportionally)
- FVC <80% predicted with normal ratio - suggestive; confirmed by low TLC on body plethysmography
- FEV1/FVC may actually be >70% (e.g., 90% in fibrosing alveolitis)
- Causes: Pulmonary fibrosis, pleural disease, chest wall deformity, neuromuscular disease, obesity
Example values (Bailey & Love):
- Normal: FEV1 3.1 L, FVC 3.8 L, FEV1/FVC 82%
- Obstructive (asthma): FEV1 1.4 L, FVC 3.5 L, FEV1/FVC 40% → post-bronchodilator: FEV1 2.5 L, FVC 3.5 L, FEV1/FVC 71%
- Restrictive (fibrosing alveolitis): FEV1 1.8 L, FVC 2.0 L, FEV1/FVC 90%
Mixed Pattern
- Low FEV1/FVC + low TLC
- Both obstruction and restriction co-exist
Non-Specific Pattern
- Normal FEV1/FVC with low FEV1 or low FVC, but TLC is normal
- Does not fit classical obstructive or restrictive criteria
Bronchodilator Reversibility Testing
After baseline spirometry, administer a short-acting bronchodilator (typically salbutamol 400 mcg) and repeat after 15-20 minutes.
Positive bronchodilator response (ATS/ERS criteria):
- Increase in FEV1 of >12% AND >200 mL from baseline
- Also: increase in FVC of >20% and >200 mL
This indicates reversible airflow obstruction and is suggestive (not diagnostic) of asthma. In asthma, the FEV1/FVC is typically <70%; in severe asthma with significant air trapping, the FVC may fall and paradoxically increase the FEV1/FVC ratio.
- Murray & Nadel's Textbook of Respiratory Medicine
Spirometry in Specific Diseases
Asthma (FEV1-based severity, NAEP 2007)
| FEV1 % Predicted | Severity |
|---|---|
| ≥80% | Mild (if symptomatic) |
| 60-79% | Moderate |
| ≤60% | Severe |
COPD
- Diagnosis requires postbronchodilator FEV1/FVC < 0.70
- Flow-volume loop: concave expiratory limb, reduced flow at all volumes
- Volume-time curve: prolonged expiratory time
Additional Related Tests
| Test | What it Measures | Clinical Use |
|---|---|---|
| DLCO (diffusing capacity for CO) | Gas transfer across alveolar-capillary membrane | Low in emphysema, ILD; normal/high in asthma |
| TLC (total lung capacity) | All lung gas at maximal inflation (body plethysmography) | Confirms restriction (low TLC) or hyperinflation (high TLC) |
| RV/TLC ratio | Air trapping index | Elevated in obstruction |
| MVV | Maximal voluntary ventilation | Can be estimated as FEV1 × 35-40; estimates exercise ventilatory reserve |
Indications for Spirometry
- Diagnosis of obstructive or restrictive lung disease (asthma, COPD, ILD, NMD)
- Monitoring disease progression or treatment response
- Occupational surveillance - workers in hazardous environments
- Preoperative assessment - particularly before lung resection surgery
- Disability evaluation
Note: Spirometry alone cannot establish a specific disease diagnosis - it characterizes the pattern and severity of ventilatory defect. Most diseases cause a predictable type of defect, and the test is sufficiently reproducible to follow disease course over time.
- Murray & Nadel's Textbook of Respiratory Medicine; Bailey & Love's Short Practice of Surgery; Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.