Q. Discuss the etiopathogenesis, clinical features, complications and management of Coalescent mastoiditis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
coalescent mastoiditis etiopathogenesis pathology acute mastoiditis
search_medical_text
coalescent mastoiditis clinical features complications management treatment surgery
search_medical_image
coalescent mastoiditis CT scan diagram anatomy
GradeResponse
GradeResponse
GradeResponse
Now I have solid foundational material. Let me compose a comprehensive, examination-grade answer synthesizing retrieved content with my full knowledge base from the referenced textbooks.
COALESCENT MASTOIDITIS
A Comprehensive 50-Mark Answer
[As per RGUHS curriculum — Scott-Brown, Cummings, Stell & Maran, Dhingra, Hazarika, Zakir Hussain and recent advances]
TABLE OF CONTENTS
- Introduction & Definition
- Surgical Anatomy of the Mastoid
- Etiopathogenesis
- Pathological Stages
- Clinical Features
- Diagnosis & Investigations
- Complications
- Management
- Recent Advances
- Flowcharts & Summary Tables
1. INTRODUCTION & DEFINITION
Coalescent mastoiditis (also called Acute Surgical Mastoiditis, Acute Suppurative Mastoiditis with Bony Destruction, or Mastoid Empyema) is the stage of acute mastoiditis in which the bony septa between adjacent mastoid air cells are destroyed by the suppurative process, converting the mastoid into a single pus-filled cavity.
"Coalescent mastoiditis involves destruction of the bony septa of the mastoid air cells, representing progression beyond incipient mastoiditis." — Harrison's Principles of Internal Medicine, 21st Ed., p. 1061
It is a true surgical emergency in ENT — failure to treat leads to life-threatening intracranial and extracranial complications.
2. SURGICAL ANATOMY OF THE MASTOID
Understanding the anatomy is essential to appreciating the pathology and complications.
MASTOID ANATOMY (SCHEMATIC)
══════════════════════════════════════════════════════════
SQUAMOSAL SUTURE
|
┌──────────┴──────────────────────────┐
│ MASTOID PROCESS │
│ │
│ ┌─────────────────┐ │
│ │ MASTOID ANTRUM │ ← KEY SPACE │
│ │ (always present)│ │
│ └────────┬────────┘ │
│ │ Aditus ad Antrum │
│ ┌──────┴───────┐ │
│ │ EPITYMPANUM │ │
│ │ (Attic) │ │
│ └──────────────┘ │
│ │
│ Air cells: Periantral → Peripheral │
│ │
│ Boundaries: │
│ - Anterior: EAC, middle ear │
│ - Superior: Middle cranial fossa │
│ - Posterior/medial: Posterior │
│ cranial fossa, sigmoid sinus │
│ - Medial: Labyrinth │
│ - Lateral: Mastoid cortex │
└─────────────────────────────────────┘
Macewan's Triangle (Suprameatal Triangle):
- Lies posterosuperior to EAC
- Surface marking for mastoid antrum (1.5 cm deep in adults)
- Bounded by:
→ Suprameatal crest (above)
→ Posterosuperior wall of EAC (anteriorly)
→ Tangent from posterior wall EAC (posteriorly)
Key relationships (Dhingra, 7th Ed.):
- Sigmoid sinus: posterior to mastoid air cells
- Facial nerve: traverses the mastoid in its third (mastoid/vertical) segment
- Dural plates: cover the tegmen (roof) and posterior fossa wall
- Labyrinth (semicircular canals): medial boundary
3. ETIOPATHOGENESIS
3.1 Etiology
Causative Organisms
| Organism | Frequency | Notes |
|---|---|---|
| Streptococcus pneumoniae | Most common | All ages; post-antibiotic era |
| Streptococcus pyogenes (Group A) | Common | Virulent; risk of intracranial spread |
| Haemophilus influenzae | Common in children | Less since Hib vaccine |
| Staphylococcus aureus (MRSA) | Increasing | Post-surgical, neonates |
| Pseudomonas aeruginosa | Chronic/post-antibiotic | Gram-negative |
| Fusobacterium necrophorum | Rare | Lemierre's syndrome association |
| Anaerobes | Chronic suppurative disease | Bacteroides, Peptostreptococcus |
(Harrison's 21st Ed., p. 1061; Cummings Otolaryngology, 7th Ed.)
Predisposing Factors
- Inadequately treated AOM (most common precipitant)
- Antibiotic resistant organisms
- Immunosuppression (HIV, diabetes, malnutrition)
- Virulent organisms (Group A Streptococcus)
- Anatomical factors: sclerotic mastoid, poor pneumatization
- Chronic otitis media as background
- Young age (< 2 years) — immune immaturity
- Cleft palate, Down syndrome (Eustachian tube dysfunction)
3.2 Pathogenesis
PATHOGENESIS FLOWCHART
══════════════════════════════════════════════════════════════
UPPER RESPIRATORY TRACT INFECTION / AOM
│
▼
┌───────────────────────────────────┐
│ EUSTACHIAN TUBE DYSFUNCTION │
│ → Negative middle ear pressure │
│ → Fluid accumulation in ME │
└──────────────┬────────────────────┘
│
▼
┌───────────────────────────────────┐
│ ACUTE OTITIS MEDIA (AOM) │
│ Stage 1: Hyperemia │
│ Stage 2: Exudation │
│ Stage 3: Suppuration │
└──────────────┬────────────────────┘
│
Spread via Aditus ad Antrum
│
▼
┌───────────────────────────────────┐
│ INCIPIENT MASTOIDITIS │
│ • Mucosal congestion │
│ • Edema of air cell lining │
│ • Fluid in mastoid air cells │
│ • Bony septa INTACT │
│ • Reversible with antibiotics │
└──────────────┬────────────────────┘
│
Continued infection +
Inadequate drainage +
Virulent organism
│
▼
┌───────────────────────────────────┐
│ COALESCENT MASTOIDITIS ★ │
│ • Periostitis of bony septa │
│ • Osteitis → necrosis of septa │
│ • DESTRUCTION of bony walls │
│ • Cells merge → EMPYEMA CAVITY │
│ • Pus under pressure │
└──────────────┬────────────────────┘
│
┌──────────┴──────────┐
│ │
▼ ▼
Lateral spread Medial/Superior/
through cortex Posterior spread
│ │
▼ ▼
SUBPERIOSTEAL COMPLICATIONS
ABSCESS (see Section 7)
3.3 Mechanism of Bony Destruction (Detailed)
The key pathophysiological step distinguishing coalescent from incipient mastoiditis is osteitis with coalescence:
- Vascular engorgement of the mucoperiosteum lining air cells → edema
- Pus accumulation raises intracellular pressure
- Ischemia of bone due to pressure on small feeding vessels
- Osteoclastic resorption activated by inflammatory mediators (IL-1β, TNF-α, PGE₂)
- Enzymatic digestion of bony trabeculae by bacterial proteases and neutrophil elastase
- Necrosis of intervening septa → air cells merge
- Formation of a single empyema cavity with pus under tension
This process follows the "path of least resistance":
- Laterally → through mastoid cortex → subperiosteal abscess (most common)
- Superiorly → through tegmen mastoideum → extradural abscess
- Posteriorly → sigmoid sinus plate → sigmoid sinus thrombophlebitis
- Medially → into labyrinth → labyrinthitis
- Via Trautmann's triangle → posterior fossa extension
- Along facial nerve sheath or petrous apex → Gradenigo's syndrome (rarely)
(Scott-Brown's Otolaryngology, 8th Ed.; Stell & Maran, 5th Ed.)
4. PATHOLOGICAL STAGES
As described by Schwartze (1873) and refined by Proctor:
| Stage | Name | Pathology |
|---|---|---|
| I | Hyperemia | Mucosal hyperemia, mild edema |
| II | Exudation | Serous/seropurulent fluid in cells |
| III | Suppuration (Incipient) | Frank pus in cells, septa intact |
| IV | Coalescence ★ | Septa destroyed, empyema formed |
| V | Complication | Extension beyond mastoid |
5. CLINICAL FEATURES
5.1 History
- Prior episode of AOM in 2–4 weeks (most common presentation)
- "Masked mastoiditis": inadequate antibiotic treatment suppresses symptoms but does not eradicate infection
- Recurrence or worsening of ear symptoms after initial improvement
5.2 Symptoms
| Symptom | Description |
|---|---|
| Otalgia | Severe, deep-seated, throbbing pain; extends over mastoid |
| Otorrhoea | Profuse, creamy-yellow, pulsatile discharge; "lighthouse sign" (cream-colored pus spurting with each pulse) — Dhingra |
| Hearing loss | Conductive type; often pre-existing |
| Fever | High-grade, continuous; may be spiking |
| Headache | Frontal/temporal; worsens at night |
| Postauricular swelling | Tender, fluctuant; hallmark of subperiosteal abscess |
| Vertigo/tinnitus | Suggest labyrinthine involvement |
5.3 Signs
CLINICAL SIGNS — COALESCENT MASTOIDITIS
══════════════════════════════════════════════════════════
AURICLE DISPLACED FORWARD & DOWNWARD ★
↑
┌──────────────────────────────────────┐
│ POSTAURICULAR REGION │
│ │
│ • Obliteration of postauricular │
│ groove (earliest sign) │
│ • Erythema, edema of overlying skin│
│ • Tenderness on palpation │
│ • Fluctuation (if abscess formed) │
└──────────────────────────────────────┘
↓
OTOSCOPY FINDINGS:
• Sagging of posterosuperior meatal wall ★
(pathognomonic — due to periostitis of
posterior EAC wall from within)
• Congested, bulging TM or perforation
with profuse pulsatile discharge
• Granulations may be present
Sagging of posterosuperior meatal wall is the most important clinical sign — it indicates periostitis of the bony EAC from the mastoid side.
Mastoid Tenderness:
- Over Macewan's triangle (mastoid antrum)
- Over tip of mastoid process
5.4 Bezold's Abscess (Special Form)
Pus bursts through the medial surface of the mastoid tip → tracks under the sternocleidomastoid muscle → presents as a deep neck abscess in the posterior triangle. Described by Friedrich Bezold (1881).
BEZOLD'S ABSCESS PATHWAY:
Mastoid tip (medial cortex) →
Attachment of SCM/digastric →
Deep neck space (posterior triangle) →
Parapharyngeal / retropharyngeal space →
Mediastinum (rare, life-threatening)
5.5 Citelli's Abscess
Pus erodes through digastric ridge → tracks to posterior belly of digastric → deep to SCM → posterior belly of digastric fossa
5.6 Luc's Abscess (Zygomatic Mastoiditis)
Extension into zygomatic air cells → swelling anterior to ear, below zygomatic arch
6. INVESTIGATIONS
6.1 Laboratory
| Investigation | Finding |
|---|---|
| CBC | Leukocytosis (TLC >15,000/mm³), neutrophilia |
| ESR, CRP | Elevated |
| Blood culture | Positive in bacteremia |
| Ear swab C&S | Identifies causative organism, antibiotic sensitivity |
| LFT/RFT | Baseline before aminoglycosides |
6.2 Imaging
Plain X-Ray Mastoid (Schuller's View / Law's View)
- Loss of cellular pattern
- Haziness / clouding of air cells
- Loss of cell walls / septa (coalescence)
- Increased density of mastoid
- (Limited value in era of CT)
HRCT Temporal Bone (Gold Standard) ★
This is the investigation of choice.
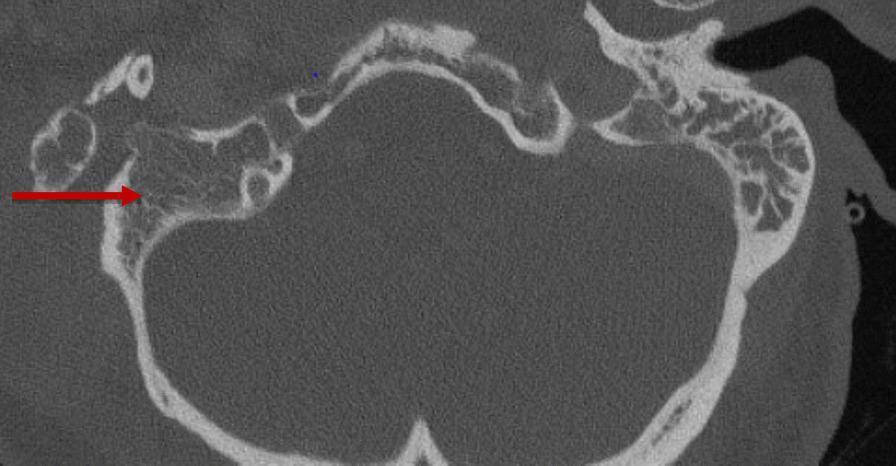
CT temporal bone (axial, non-contrast): Right-sided coalescent mastoiditis — complete opacification of mastoid air cells with destruction of bony septa (red arrow). The left side shows normal, well-pneumatized air cells. (Source: PMC Clinical VQA)
CT Findings:
- Opacification of mastoid air cells (soft tissue density replacing air)
- Destruction/erosion of bony septa ← HALLMARK of coalescent mastoiditis
- Subperiosteal abscess: soft tissue density outside mastoid cortex
- Sigmoid sinus plate erosion (risk of thrombosis)
- Tegmen erosion (risk of intracranial extension)
- Labyrinthine fistula (semicircular canal wall erosion)
MRI Brain with Gadolinium
- Indicated when intracranial complications are suspected
- Shows dural enhancement, epidural/subdural abscess, brain abscess, sigmoid sinus thrombosis
- Superior soft tissue resolution
Audiometry
- Pure tone audiogram: Conductive hearing loss (typically 30–50 dB)
- Tympanometry: Flat type B curve
7. COMPLICATIONS
COMPLICATION FLOWCHART
══════════════════════════════════════════════════════════════
COALESCENT MASTOIDITIS
│
┌────────────────┼────────────────┐
│ │ │
▼ ▼ ▼
EXTRACRANIAL INTRACRANIAL LABYRINTHINE
COMPLICATIONS COMPLICATIONS COMPLICATIONS
│ │ │
┌─────┤ ┌─────┤ ┌────┤
│ │ │ │ │ │
▼ ▼ ▼ ▼ ▼ ▼
Subperi- Bezold's Extra- Subdural Serous Suppurative
osteal abscess dural abscess labyr- labyrinth-
abscess abscess inthitis itis
│ │ │
▼ ▼ ▼
Mastoid Meningitis Sensorineural
fistula Brain abscess hearing loss
(temporal lobe Vertigo
Facial nerve or cerebellum) Nystagmus
palsy Sigmoid sinus
thrombophlebitis
Lateral sinus
thrombosis
Otitic hydrocephalus
(benign ICH)
7.1 Extracranial Complications
| Complication | Mechanism | Clinical Features |
|---|---|---|
| Subperiosteal abscess | Lateral cortex erosion | Postauricular swelling, fluctuance, auricle pushed forward |
| Bezold's abscess | Medial mastoid tip | Neck swelling, torticollis, dysphagia |
| Citelli's abscess | Digastric groove | Submandibular/lateral neck swelling |
| Luc's abscess | Zygomatic root | Preauricular swelling |
| Facial nerve palsy | Facial canal dehiscence, direct pressure | LMN facial palsy (House-Brackmann grading) |
7.2 Intracranial Complications (ICCs)
| Complication | Frequency | Clinical Pointer |
|---|---|---|
| Meningitis | Most common ICC | Neck stiffness, Kernig's, photophobia, CSF pleocytosis |
| Extradural abscess | 2nd most common | Headache, low-grade fever, dural "lollipop" on MRI |
| Brain abscess | Temporal lobe / cerebellar | Focal neurological deficit; contralateral hemiplegia / cerebellar ataxia |
| Subdural abscess | Less common | Rapid deterioration |
| Sigmoid sinus thrombophlebitis | Septic embolism risk | "Picket-fence" fever, Griesinger sign (postauricular edema due to thrombosis of emissary vein) |
| Otitic hydrocephalus | Venous hypertension | Papilledema, headache, normal CSF |
| Gradenigo's Syndrome | Petrous apicitis | Triad: otorrhoea + trigeminal pain (V) + ipsilateral lateral rectus palsy (VI) |
Gradenigo's Triad (Stell & Maran):
- Persistent otorrhoea
- Pain in distribution of trigeminal nerve (retro-orbital)
- Ipsilateral abducens (VI) nerve palsy → diplopia
7.3 Labyrinthine Complications
- Serous labyrinthitis: Toxin spread through round window; reversible SNHL
- Suppurative (circumscribed) labyrinthitis: Labyrinthine fistula formation; profound SNHL, severe vertigo
- Petrositis: Extension to petrous apex
8. MANAGEMENT
8.1 Management Algorithm
MANAGEMENT FLOWCHART — COALESCENT MASTOIDITIS
══════════════════════════════════════════════════════════════
DIAGNOSIS: Coalescent Mastoiditis
(Clinical + CT confirmation)
│
▼
HOSPITAL ADMISSION (All cases)
+ IV Access + Blood/Ear cultures
+ Baseline investigations
│
▼
┌───────────────────────────────────────┐
│ IV ANTIBIOTICS (High dose, immediate)│
│ + Analgesics + Antipyretics │
│ + Myringotomy (if TM intact) │
└──────────────────┬────────────────────┘
│
Response to 24-48 hrs
medical therapy?
│
┌─────────┴──────────┐
│ │
▼ ▼
YES: Improving NO: Not responding
(Rare in true OR Complications
coalescent) present
│ │
▼ ▼
Continue IV CORTICAL MASTOIDECTOMY
antibiotics (Simple Mastoidectomy)
+ close follow-up │
│
┌─────────┴──────────┐
│ │
▼ ▼
Subperiosteal Intracranial
abscess present? complication?
│ │
▼ ▼
INCISE & DRAIN MRI → Neurosurgery
+ Mastoidectomy referral + Modified
Radical/Radical
Mastoidectomy
8.2 Medical Management
Antibiotic Therapy (Cummings 7th Ed., Dhingra 7th Ed.)
Empirical IV antibiotics (before culture results):
| Scenario | Antibiotic of Choice |
|---|---|
| Community-acquired, no prior antibiotics | IV Amoxicillin-Clavulanate or IV Ceftriaxone 50–100 mg/kg/day |
| Suspected MRSA | Add IV Vancomycin 15 mg/kg 8-hourly |
| Gram-negative suspected | IV Piperacillin-Tazobactam or Cefepime |
| Intracranial extension | IV Ceftriaxone + Metronidazole + Vancomycin (triple therapy) |
| Post-culture, guided | Based on C&S sensitivity report |
Duration: IV antibiotics for 2–4 weeks; step-down to oral after clinical improvement.
Adjuncts:
- Analgesics (Paracetamol, NSAIDs)
- Antipyretics
- IV fluids (if toxic)
- Corticosteroids (IV Dexamethasone): reduces inflammation, especially with meningitis
- Anticoagulation: if sigmoid sinus thrombosis confirmed (controversial)
8.3 Surgical Management
A. Myringotomy ± Grommet Insertion
Indication: Intact TM with bulging
- Provides drainage of middle ear pus
- Relieves pressure
- Allows microbiological sampling
- Does NOT address mastoid disease — preliminary step
B. Cortical Mastoidectomy (Schwartze Operation) ★
The definitive surgery for coalescent mastoiditis.
Eponym: Schwartze and Eysell (1873)
CORTICAL MASTOIDECTOMY — STEPS
══════════════════════════════════════════════════════════
Position: Supine, head turned to opposite side
Anesthesia: General anesthesia
Incision: Postauricular (Wilde's incision)
2-3 mm behind postauricular sulcus
STEPS:
1. Postauricular incision → expose mastoid cortex
2. Identify landmarks:
- Macewan's (Suprameatal) triangle
- Spine of Henle
- Linea temporalis (superior)
- EAC (anterior)
3. Open mastoid cortex with cutting burr
Drill in Macewan's triangle area
4. Exenterate ALL air cells:
- Periantral cells
- Peripheral cells (tip, zygomatic, perilabyrinthine)
5. Identify and preserve:
- Tegmen plate (dural plate, superior)
- Sigmoid sinus plate (posterior)
- Posterior EAC wall (DO NOT BREACH)
- Facial nerve (horizontal portion, vertical segment)
- Short process of incus (landmark for lateral semicircular canal)
- Lateral semicircular canal (blue line)
6. Open antrum → communicate with ME via aditus
7. Achieve hemostasis
8. Wound closure with drain
RULE OF CORTICAL MASTOIDECTOMY:
"Remove all infected cells while preserving
the EAC posterior wall, ossicles, and
labyrinthine structures"
Boundaries of Dissection (Safe Triangles):
- Superiorly: Tegmen (do not breach → meningitis)
- Posteriorly: Sigmoid sinus (do not breach → massive hemorrhage)
- Anteriorly: Posterior EAC wall (preserve intact)
- Medially: Labyrinth / lateral semicircular canal (Donaldson's line)
- Inferiorly: Digastric ridge (facial nerve lies medial)
Key landmark: The short process of the incus is the most reliable landmark for the facial nerve in mastoid surgery (Cummings).
C. Modified Radical Mastoidectomy (Bondy's Operation)
- When attic/epitympanic disease present with intact ossicles
- Creates mastoid cavity open to EAC; preserves ossicular chain
D. Radical Mastoidectomy (Zaufal-Stacke)
- When ossicles and middle ear are extensively diseased
- Creates large open cavity
- Rarely needed in primary coalescent mastoiditis
E. Drainage of Subperiosteal Abscess
- Incision over most fluctuant point
- Drainage + culture
- Often combined with mastoidectomy in same sitting
F. Management of Bezold's Abscess
- Postauricular incision extended inferiorly along anterior SCM border
- Drainage of neck collection
- Mastoidectomy in same sitting
8.4 Management of Specific Complications
| Complication | Management |
|---|---|
| Facial nerve palsy | Mastoidectomy + facial nerve decompression; nerve repair if lacerated |
| Meningitis | High-dose IV antibiotics (Ceftriaxone + Vancomycin); consider Dexamethasone; Neurology consult |
| Extradural abscess | Mastoidectomy + drainage via bone removal over dura |
| Brain abscess | Neurosurgery: aspiration or excision; long-term antibiotics |
| Sigmoid sinus thrombosis | Mastoidectomy + unroofing of sigmoid; anticoagulation (controversial); ligation if septic embolism |
| Labyrinthine fistula | Mastoidectomy with preservation of matrix over fistula; fascia graft |
| Otitic hydrocephalus | Acetazolamide, repeated LP, optic nerve sheath decompression |
9. RECENT ADVANCES
9.1 Antibiotic Stewardship & Trends
- Rising incidence of MRSA-related mastoiditis (community-acquired MRSA, CA-MRSA) — now detected in up to 10–15% of cases in some series
- Extended-spectrum beta-lactamase (ESBL)-producing organisms increasing
- Routine culture and sensitivity mandatory before committing to long-term antibiotics
- Linezolid and daptomycin as alternatives in MRSA mastoiditis
9.2 Minimally Invasive Approaches
- Endoscopic-assisted mastoidectomy: Karl Storz 0° and 30° rigid endoscopes to inspect residual cells, especially around facial nerve and oval window niche
- Image-guided surgery (Navigation/IGS): CT-based intraoperative navigation for complex mastoiditis with significant anatomy distortion or previous surgery
- Reduces risk to facial nerve and sigmoid sinus
9.3 Diagnostic Advances
- Diffusion-weighted MRI (DWI): Superior for distinguishing brain abscess from tumor; identifying early cerebritis
- MR Venography: Non-invasive investigation for sigmoid sinus thrombosis (replaces invasive venography)
- PET-CT: Emerging role in differentiating active infection from post-surgical change
9.4 Microbiology Advances
- 16S rRNA gene sequencing and metagenomic next-generation sequencing (mNGS) — identifies organisms that do not grow on routine culture (anaerobes, fastidious organisms)
- Fusobacterium necrophorum increasingly recognized in adolescents; associated with Lemierre's syndrome
9.5 Immunological Insights
- Role of biofilm formation by S. aureus and P. aeruginosa in recurrent/refractory mastoiditis
- Biofilms resist conventional antibiotics; anti-biofilm agents (e.g., N-acetylcysteine, dispersin B) under investigation
9.6 Outcome Studies
- Recent systematic reviews (2019–2023) confirm that early cortical mastoidectomy is superior to prolonged IV antibiotics alone in true coalescent mastoiditis
- Intracranial complications have not decreased significantly despite antibiotic availability — suggesting need for higher clinical vigilance
- Grommets at time of mastoidectomy reduce need for revision surgery (Level III evidence)
10. FLOWCHARTS & SUMMARY TABLES
DIFFERENTIAL DIAGNOSIS TABLE
| Condition | Differentiating Feature |
|---|---|
| Acute mastoiditis (incipient) | No bony destruction on CT; responds to IV antibiotics |
| Postauricular lymphadenitis | Lymph node palpable; no EAC changes; no TM pathology |
| Ramsay Hunt syndrome | Herpetic vesicles in EAC; facial palsy; SNHL; viral serology |
| Furuncle of EAC | Localized, no mastoid tenderness, EAC swelling only |
| Postauricular sebaceous cyst | Chronic, non-tender, translucent skin change, no fever |
| Cholesteatoma with abscess | Long history COM; keratin debris; attic perforation |
SUMMARY TABLE: COMPLICATIONS OF COALESCENT MASTOIDITIS
┌──────────────────────────────────────────────────────┐
│ COMPLICATIONS — SUMMARY │
├─────────────────┬────────────────────────────────────┤
│ EXTRACRANIAL │ INTRACRANIAL │
├─────────────────┼────────────────────────────────────┤
│ Subperiosteal │ Meningitis (most common ICC) │
│ abscess │ │
│ Bezold's │ Extradural abscess │
│ abscess │ │
│ Citelli's │ Subdural empyema │
│ abscess │ │
│ Luc's abscess │ Brain abscess (temporal/cerebellar)│
│ Mastoid │ Sigmoid sinus thrombophlebitis │
│ fistula │ │
│ Facial palsy │ Otitic hydrocephalus │
│ (extracranial) │ Gradenigo's syndrome │
├─────────────────┼────────────────────────────────────┤
│ LABYRINTHINE │ │
├─────────────────┤ MANAGEMENT PRINCIPLE: │
│ Serous │ │
│ labyrinthitis │ Mastoidectomy + targeted │
│ Suppurative │ antibiotics + drainage of │
│ labyrinthitis │ any abscesses ± neurosurgery │
│ Petrositis │ │
└─────────────────┴────────────────────────────────────┘
ANTRUM LANDMARKS MNEMONICS
"She Likes Doing Fascinating Surgery"
- Sinus (sigmoid) → posterior
- Linea temporalis → superior
- Donaldson's line → lateral SCC
- Facial nerve → anterior/inferior
- Spine of Henle → anterior landmark of suprameatal triangle
REFERENCES
- Harrison's Principles of Internal Medicine, 21st Edition, p. 1061 — Pathogenesis of mastoiditis, causative organisms
- Cummings Otolaryngology: Head and Neck Surgery, 7th Edition — Management of acute mastoiditis, surgical technique
- Scott-Brown's Otolaryngology, 8th Edition — Etiopathogenesis, complications, surgical anatomy
- Dhingra's Diseases of Ear, Nose and Throat, 7th Edition — Clinical features, signs, Bezold's abscess, management
- Stell & Maran's Textbook of Head and Neck Surgery, 5th Edition — Gradenigo's syndrome, petrositis, intracranial complications
- Hazarika's Textbook of ENT and Head-Neck Surgery — RGUHS-oriented approach, cortical mastoidectomy technique
- Zakir Hussain's ENT Review — RGUHS examination-focused treatment algorithms
- PMC Clinical VQA Dataset — CT temporal bone image demonstrating coalescent mastoiditis with bony destruction
Examiner's Note (RGUHS): For a 50-mark RGUHS answer, the key points examiners expect are: (i) Definition clearly distinguishing incipient vs. coalescent mastoiditis, (ii) Pathogenesis with emphasis on osteitis and septa destruction, (iii) Sagging of posterosuperior meatal wall as the pathognomonic sign, (iv) HRCT as investigation of choice, (v) Cortical (Schwartze) mastoidectomy as definitive treatment with steps and landmarks, (vi) Complication chart including Bezold's abscess and intracranial complications, (vii) Gradenigo's triad, and (viii) Recent advances including MRSA, endoscopic mastoidectomy and navigation-guided surgery.
This is a shared conversation. Sign in to Orris to start your own chat.