Difference and ECG differences of sinus tachycardia, sinus brandycardia, sinus arrhythmia, sick sinus arrhythmia, atrial fibrillation, atrial flutter with image explanation.
Reading File
search_medical_text
sinus tachycardia sinus bradycardia sinus arrhythmia ECG features diagnosis criteria
search_medical_text
sick sinus syndrome atrial fibrillation atrial flutter ECG features diagnosis
search_medical_image
sinus tachycardia sinus bradycardia ECG rhythm strip
search_medical_image
atrial fibrillation atrial flutter ECG rhythm strip
GradeResponse
GradeResponse
GradeResponse
GradeResponse
search_medical_text
atrial fibrillation ECG irregularly irregular absent P waves fibrillatory baseline clinical features
search_medical_text
atrial flutter sawtooth F waves AV block 2:1 4:1 ECG clinical features
search_medical_image
sick sinus syndrome sinus arrhythmia ECG bradycardia pauses
Here is a comprehensive comparison of all six rhythm disorders, synthesized from Harrison's Principles of Internal Medicine (21st Ed.) and core electrophysiology knowledge.
Sinus & Atrial Rhythm Disorders: ECG Comparison Guide
Quick Reference Table
| Feature | Sinus Tachycardia | Sinus Bradycardia | Sinus Arrhythmia | Sick Sinus Syndrome | Atrial Fibrillation | Atrial Flutter |
|---|---|---|---|---|---|---|
| Rate | >100 bpm | <60 bpm | 60–100 bpm (variable) | Variable (often <50 bpm) | 350–600 atrial; 60–180 ventricular | 250–350 atrial; ~150 ventricular |
| Rhythm | Regular | Regular | Irregularly regular | Irregular, with pauses | Irregularly irregular | Regular (or patterned) |
| P waves | Normal sinus | Normal sinus | Normal sinus | Absent/abnormal during pauses | Absent; fibrillatory baseline | Sawtooth F-waves |
| P:QRS ratio | 1:1 | 1:1 | 1:1 | Variable | No consistent P waves | 2:1, 3:1, or 4:1 |
| PR interval | Normal | Normal | Normal | Variable | Unmeasurable | Normal per conducted beat |
| QRS | Narrow (unless aberrant) | Narrow | Narrow | Narrow (unless bundle branch disease) | Narrow (unless aberrant) | Narrow (unless aberrant) |
1. Sinus Tachycardia
What it is
Accelerated firing of the sinoatrial (SA) node, almost always a physiologic response to an underlying cause (fever, pain, anemia, hypovolemia, anxiety, hyperthyroidism, drugs). Intrinsic (inappropriate) sinus tachycardia is rare.
ECG Features
- Rate: >100 bpm (usually 100–180 bpm)
- P waves: Normal sinus morphology — positive in leads I, II, aVF; biphasic in V₁; frontal axis 0°–90° (Harrison's, p. 6998)
- P:QRS: 1:1, every P followed by a QRS
- PR interval: Normal (0.12–0.20 s), may shorten slightly at very fast rates
- QRS: Narrow, normal morphology
- Rhythm: Regular
- Key finding: Gradual onset and offset ("warm up / cool down") — distinguishes it from paroxysmal SVT
Clinical Pearl
Treat the cause, not the rate. Beta-blockers are indicated only in inappropriate sinus tachycardia or when rate control is hemodynamically essential.
2. Sinus Bradycardia
What it is
Slowed SA node automaticity. Can be normal (athletes, vagal tone during sleep) or pathologic (hypothyroidism, inferior MI, increased ICP, beta-blockers, calcium channel blockers, hypothermia).
ECG Features
- Rate: <60 bpm
- P waves: Normal sinus morphology (positive I, II, aVF)
- P:QRS: 1:1
- PR interval: Normal
- QRS: Narrow
- Rhythm: Regular
- Key finding: Everything looks like a normal sinus rhythm — just slower
Clinical Pearl
Asymptomatic sinus bradycardia in a young, fit athlete requires no treatment. Symptomatic bradycardia with hypotension → atropine IV, then transcutaneous pacing if refractory.
3. Sinus Arrhythmia
What it is
A normal variant caused by cyclical variation in vagal tone with respiration. During inspiration, vagal tone decreases → heart rate increases. During expiration, vagal tone increases → heart rate decreases. Most prominent in children and young adults.
ECG Features
- Rate: Normal (60–100 bpm), but varies by >10% with respiration (or >0.12 s PP interval variation)
- P waves: Normal sinus morphology — identical shape in each lead
- P:QRS: 1:1
- PR interval: Normal and constant
- QRS: Narrow
- Rhythm: Irregularly regular — cycles with breathing
- Key finding: The PP interval waxes and wanes with the respiratory cycle; the P-wave morphology is always the same (unlike ectopic atrial beats)
Clinical Pearl
Non-respiratory sinus arrhythmia (PP variation not linked to breathing) can indicate SA node disease and warrants further evaluation.
4. Sick Sinus Syndrome (Sinus Node Dysfunction / SND)
What it is
Intrinsic disease of the SA node causing failure of impulse generation or conduction. Can manifest as persistent bradycardia, sinus pauses/arrest, sinoatrial exit block, or tachy-brady syndrome (alternating tachycardia and bradycardia). Common in the elderly; associated with fibrosis, ischemia, infiltrative disease (Harrison's, p. 6949).
ECG Features (multiple patterns)
- Persistent sinus bradycardia (<40–50 bpm, not explained by medications or vagal tone)
- Sinus pauses/arrest: PP intervals suddenly double or triple (or are not multiples of the basic PP) — a pause with no P wave
- Sinoatrial exit block:
- Type I (Wenckebach): Progressive PP shortening before a dropped P wave
- Type II: Pause is an exact multiple of the basic PP interval
- Tachy-Brady pattern: Bursts of atrial fibrillation or flutter alternating with profound bradycardia or sinus pauses after termination of the tachycardia
- Chronotropic incompetence: Heart rate fails to increase appropriately with exercise
- Key finding: Symptoms (syncope, presyncope, fatigue) + documented bradycardia or pauses on Holter/telemetry
Clinical Pearl
Diagnosis requires symptom-rhythm correlation — a resting ECG alone is often insufficient. Many patients need permanent pacemaker implantation (Harrison's, p. 6949).
5. Atrial Fibrillation (AF)
What it is
Chaotic, disorganized electrical activity throughout both atria from multiple re-entrant wavelets. The atria quiver at 350–600 impulses/min; the AV node acts as a gatekeeper, conducting impulses irregularly to the ventricles. Most common sustained arrhythmia worldwide. Risk factors: hypertension, heart failure, valvular disease, age, sleep apnea, thyrotoxicosis.
ECG Features
- Rate: Atrial 350–600 bpm (unmeasurable); ventricular 60–180 bpm depending on AV nodal conduction
- P waves: Absent — replaced by an irregular, chaotic fibrillatory baseline (f-waves), best seen in V₁ and lead II
- Rhythm: Irregularly irregular R-R intervals — the hallmark finding
- PR interval: Unmeasurable (no discrete P waves)
- QRS: Narrow (unless pre-existing bundle branch block or rate-related aberrancy → Ashman phenomenon)
- Baseline: Undulating, fibrillatory — no isoelectric line between QRS complexes
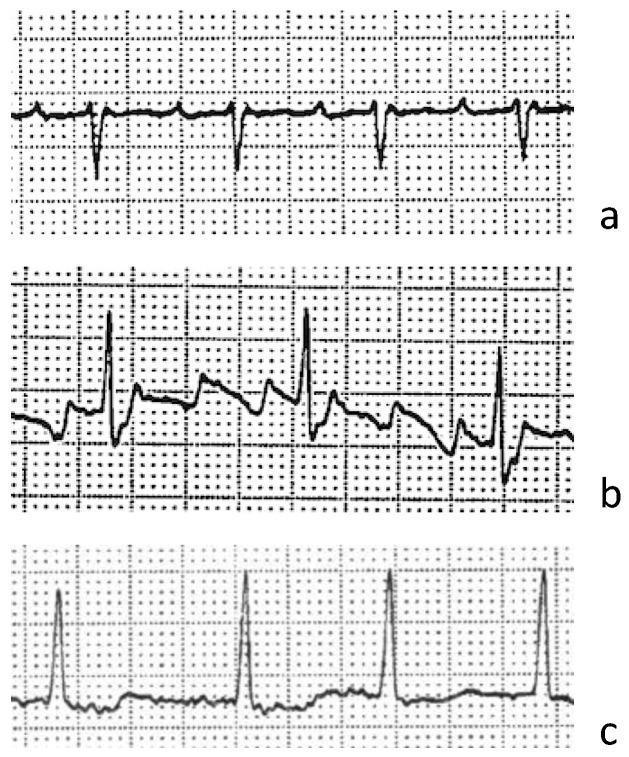
ECG Image
Clinical Pearl
The 3 management pillars: Rate control (beta-blockers, CCBs, digoxin) + Rhythm control (cardioversion, antiarrhythmics) + Anticoagulation (CHA₂DS₂-VASc score to guide stroke prevention with warfarin or DOAC).
6. Atrial Flutter
What it is
A macro-reentrant circuit, typically circulating around the tricuspid annulus in the right atrium (typical/counterclockwise flutter). The atria beat at 250–350 bpm. The AV node usually conducts with a 2:1 block → ventricular rate ~150 bpm (classic presentation). Less commonly 3:1 or 4:1 block.
ECG Features
- Atrial rate: 250–350 bpm (classically ~300 bpm)
- Ventricular rate: Depends on AV conduction ratio:
- 2:1 block → ~150 bpm
- 4:1 block → ~75 bpm
- Flutter waves (F-waves): Classic sawtooth pattern — negative, continuous, undulating waves in leads II, III, aVF with no isoelectric baseline between them; positive in V₁
- P waves: Replaced by F-waves; no true P waves
- Rhythm: Regularly regular (or regularly patterned if AV ratio varies)
- QRS: Narrow (unless aberrant conduction)
- Key diagnostic trick: At 2:1 flutter, the ventricular rate is ~150 bpm — always suspect flutter when the rate is exactly 150. Carotid sinus massage or adenosine transiently slows AV conduction and unmasks the sawtooth F-waves.
Clinical Pearl
Atrial flutter is highly amenable to catheter ablation of the cavotricuspid isthmus (CTI), with >95% success rates. Anticoagulation strategy mirrors AF (same thromboembolic risk).
Summary: Key ECG Differentiators at a Glance
| Clue on ECG | Think of... |
|---|---|
| Normal P waves, rate >100, gradual onset | Sinus Tachycardia |
| Normal P waves, rate <60, regular | Sinus Bradycardia |
| Normal P waves, rate varies with breathing | Sinus Arrhythmia |
| Pauses, brady-tachy alternation, no clear P waves during pauses | Sick Sinus Syndrome |
| No P waves, chaotic baseline, irregularly irregular QRS | Atrial Fibrillation |
| Sawtooth F-waves at ~300/min, regular ventricular rate ~150 | Atrial Flutter |
Sources: Harrison's Principles of Internal Medicine, 21st Edition (pp. 6998, 6949); ECG images from PMC Clinical VQA dataset (Orris Medical Image Database).
This is a shared conversation. Sign in to Orris to start your own chat.