Atropine drug
Reading File
Finding Sources
Searching the Web
atropine drug pharmacology uses mechanism of action
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data. Here is the full detailed answer on Atropine:
Atropine
Class: Anticholinergic (Antimuscarinic) agent | Source: Atropa belladonna (deadly nightshade)
WHO Essential Medicine: Yes
Chemical Structure & Physical Properties
Atropine is a tertiary amine - an ester of an aromatic acid (tropic acid) combined with an organic base (tropine). It is a racemic mixture of equal parts d- and l-hyoscyamine; only the levorotatory (l-) form is pharmacologically active. The ester linkage is essential for effective binding to acetylcholine receptors.
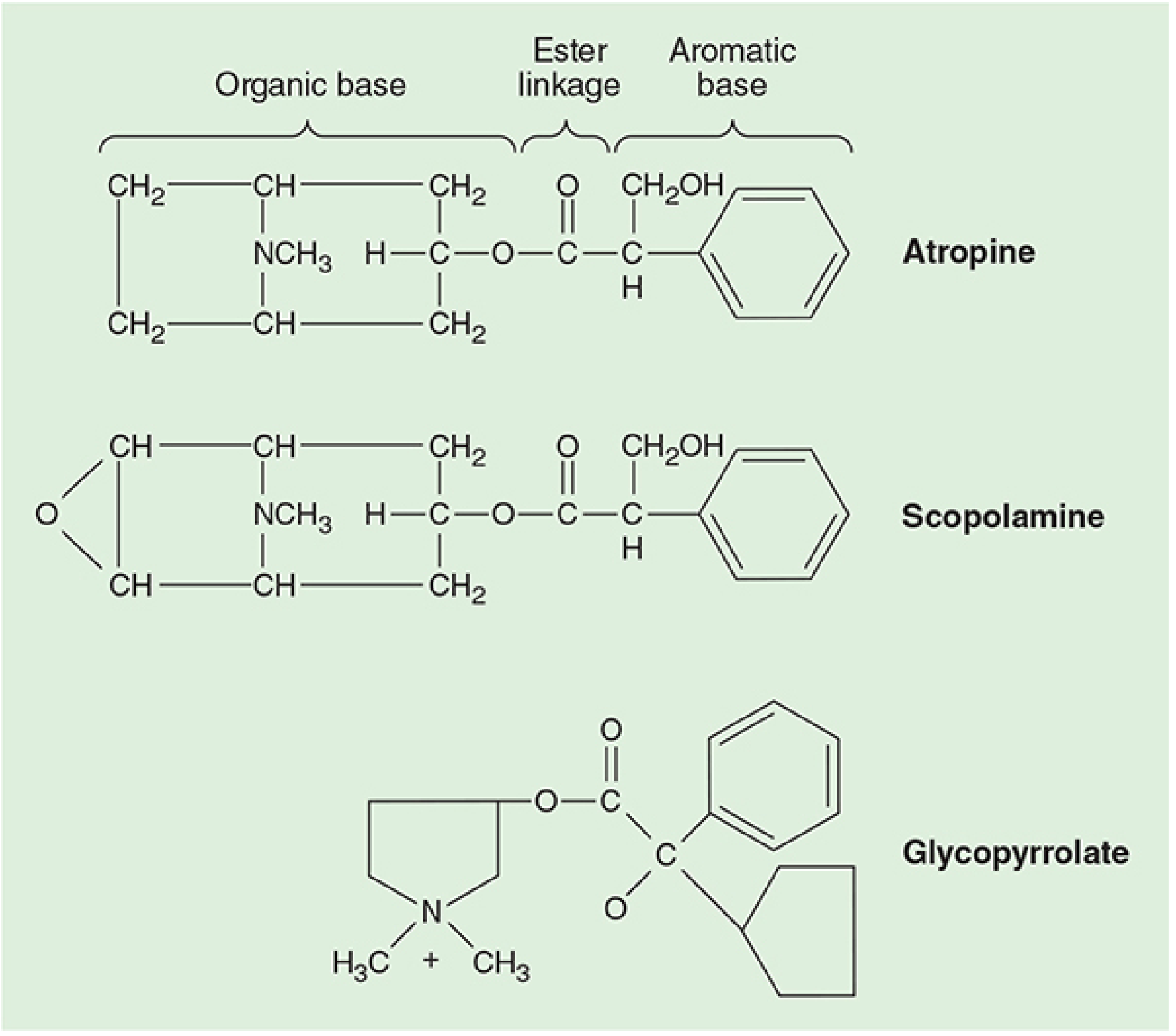
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 431
Because it is a tertiary amine, atropine can cross the blood-brain barrier (unlike glycopyrrolate, a quaternary ammonium compound, which cannot).
Mechanism of Action
Atropine is a competitive, reversible antagonist of muscarinic acetylcholine receptors. It blocks the binding of acetylcholine (ACh) to muscarinic receptors, thereby preventing receptor activation and inhibiting the cellular effects mediated through second messengers. It does NOT block nicotinic receptors at standard clinical doses.
Muscarinic receptor subtypes blocked:
| Subtype | Location | Effect of Blockade |
|---|---|---|
| M1 | Autonomic ganglia, gastric parietal cells, CNS | Decreased gastric acid, CNS effects |
| M2 | Cardiac (SA node, AV node) | Tachycardia, shortened PR interval |
| M3 | Smooth muscle, glands | Bronchodilation, reduced secretions, mydriasis |
The degree of clinical response depends on the baseline vagal tone of the patient.
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 430-431
Pharmacological Effects by System
Cardiovascular
- Blocks M2 receptors at the SA node → tachycardia (most potent anticholinergic for this)
- Promotes conduction through the AV node → shortens PR interval
- Reverses vagally-mediated bradycardia (baroreceptor reflex, oculocardiac reflex, peritoneal traction)
- Paradoxical bradycardia may occur with small IV doses (<0.4 mg) - mechanism unclear
- Large doses can cause atrial arrhythmias and nodal rhythms
- Dilates cutaneous vessels at large doses (atropine flush)
- Caution: Patients with CAD may not tolerate increased myocardial O2 demand from tachycardia
Respiratory
- Inhibits secretions from nose to bronchi (antisialagogue, antitussive)
- Relaxes bronchial smooth muscle → bronchodilation, reduces airway resistance, increases anatomical dead space
- Effects more pronounced in COPD and asthma
- Derivative ipratropium bromide (quaternary ammonium - no systemic absorption) is used in metered-dose inhalers for bronchospasm
Central Nervous System
- Minimal CNS effects at usual doses despite crossing the BBB
- At toxic doses: excitatory reactions, restlessness, hallucinations
- Associated with mild postoperative memory deficits
- Reversed by physostigmine (cholinesterase inhibitor that crosses the BBB)
Gastrointestinal
- Markedly reduces salivation
- Reduces gastric secretions (at larger doses)
- Decreases intestinal motility and peristalsis → prolonged gastric emptying
- Reduces lower esophageal sphincter pressure
- Does NOT prevent aspiration pneumonia
Ophthalmic
- Mydriasis (pupillary dilation) - especially with topical use
- Cycloplegia (loss of accommodation to near vision)
- Atropine eye drops last 7-14 days (much longer than tropicamide)
- Risk of precipitating acute angle-closure glaucoma
Genitourinary
- Smooth muscle relaxation → decreased ureter and bladder tone
- May cause urinary retention, especially in men with prostatic hypertrophy
Thermoregulation
- Inhibits sweat glands → atropine fever (hyperthermia)
Indications & Clinical Uses
| Indication | Route | Notes |
|---|---|---|
| Symptomatic bradycardia | IV | Drug of choice; 0.5-1 mg IV q5 min, max 3 mg |
| Organophosphate/nerve agent poisoning | IV/IM/IO | Reverses muscarinic toxidrome; large doses needed; does NOT reverse nicotinic muscle weakness |
| Preoperative antisialagogue | IV/IM | 0.4-0.6 mg; prevents secretions during airway procedures |
| Reversal of vagal bradycardia | IV | Oculocardiac reflex, peritoneal traction |
| Ophthalmic - mydriasis/cycloplegia | Topical | Uveitis, refraction exams, amblyopia treatment |
| Preintubation (children) | IV/IM | 0.02 mg/kg; evidence for routine use is limited |
| Bronchospasm | Nebulized | 0.025-0.05 mg/kg in 2.5 mL NS |
Dosing (Adults and Pediatrics)
Bradycardia / CPR:
- Adult: 0.5-1 mg IV q5 min; max total 3 mg
- Child: 0.02 mg/kg IV/IO/IM q5 min x 2-3 doses; max single dose 0.5 mg (child), 1 mg (adolescent)
- ET tube (child): 0.04-0.06 mg/kg, diluted in 1-2 mL NS
Preintubation:
- Neonate: 0.01-0.02 mg/kg IV/IM
- Child: 0.02 mg/kg IV/IM; max 0.5 mg
- Adult: 0.5 mg IV/IM
Organophosphate poisoning (AtroPen IM autoinjector):
- <6 mo (<7 kg): 0.25 mg
- 6 mo-4 yr (7-18 kg): 0.5 mg
- 4-10 yr (18-41 kg): 1 mg
-
10 yr and adult (>41 kg): 2 mg
- Mild symptoms: 1 dose; Severe symptoms: up to 3 doses in rapid succession
Harriet Lane Handbook, 23rd ed., p. 1026-1027
Available Formulations
| Form | Concentration |
|---|---|
| Injection (vials) | 0.4, 1 mg/mL |
| Injection (prefilled syringe) | 0.25 mg/5 mL, 0.5 mg/5 mL, 1 mg/10 mL |
| AtroPen autoinjector | 0.25, 0.5, 1, 2 mg (yellow, blue, dark red, green) |
| Ophthalmic solution | 1% (Isopto Atropine) |
| Ophthalmic ointment | 1% |
Side Effects (Anticholinergic Toxidrome)
Mnemonic: "Dry as a bone, blind as a bat, red as a beet, hot as a hare, mad as a hatter"
- Dry mouth, dry skin (anhidrosis)
- Blurred vision, mydriasis
- Flushing (atropine flush/fever)
- Hyperthermia
- Tachycardia
- CNS: dizziness, restlessness, hallucinations, delirium
- Constipation, urinary retention
Contraindications
- Glaucoma (narrow-angle) - may precipitate acute attack
- Obstructive uropathy / prostatic hypertrophy - risk of urinary retention
- Tachycardia / thyrotoxicosis (except in life-threatening muscarinic poisoning)
- Patients with CAD (tachycardia increases O2 demand)
- Heart transplant patients - atropine is ineffective for sinus bradycardia due to absence of vagal reinnervation
Comparison with Other Anticholinergics
| Effect | Atropine | Scopolamine | Glycopyrrolate |
|---|---|---|---|
| Tachycardia | +++ | + | ++ |
| Bronchodilation | ++ | + | ++ |
| Sedation | + | +++ | 0 |
| Antisialagogue | ++ | +++ | +++ |
| Crosses BBB | Yes | Yes | No |
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 431
Key Clinical Pearls
- Organophosphate poisoning: Atropine reverses muscarinic effects (SLUDGE: Salivation, Lacrimation, Urination, Defecation, GI upset, Emesis) but NOT the nicotinic-mediated muscle weakness. Add pralidoxime (2-PAM) to reactivate acetylcholinesterase.
- Heart transplant: Atropine does NOT work because the transplanted heart lacks vagal innervation - use epinephrine or pacing instead.
- Small IV doses (<0.4 mg): Can cause paradoxical bradycardia - always use adequate doses.
- Neonatal bradycardia: Routine use is no longer recommended. The old "minimum 0.1 mg" rule no longer applies and can overdose smaller patients.
- Physostigmine reverses central anticholinergic toxicity (physostigmine crosses the BBB; neostigmine does not).
Indications, contraindications, and mechanism of action of Atropine
Based on the comprehensive research I just completed on atropine, I can answer this directly from the sources already in context.
Atropine - Indications, Contraindications & Mechanism of Action
Mechanism of Action
Atropine is a competitive, reversible antagonist of muscarinic acetylcholine (ACh) receptors. It is structurally an ester of an aromatic acid combined with an organic base - the ester linkage is essential for receptor binding.
By occupying muscarinic receptors, atropine blocks ACh from binding, preventing receptor activation and inhibiting all downstream second-messenger effects. It acts on the parasympathetic nervous system as an antimuscarinic, effectively removing the "brake" that vagal tone exerts on target organs.
It does NOT block nicotinic receptors at clinical doses - this is why it cannot reverse the muscle weakness in organophosphate poisoning (nicotinic effect), only the secretory/cardiovascular muscarinic effects.
Muscarinic Receptor Subtypes Blocked
| Subtype | Location | Effect of Blockade |
|---|---|---|
| M1 | CNS, gastric parietal cells, autonomic ganglia | Reduced gastric acid; CNS stimulation at toxic doses |
| M2 | SA node, AV node (cardiac) | Tachycardia, shortened PR interval, reversal of heart block |
| M3 | Smooth muscle, exocrine glands, bronchi | Bronchodilation, dry mouth, reduced secretions, mydriasis |
The clinical response depends on baseline vagal tone - patients with high vagal tone show more pronounced responses.
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 430-431
Indications
1. Symptomatic Bradycardia
The most common emergency use. Atropine blocks M2 receptors at the SA and AV nodes, removing vagal inhibition and increasing heart rate. It is the most efficacious anticholinergic for bradyarrhythmia.
- Reverses: vagal reflex bradycardia (oculocardiac reflex, peritoneal traction, baroreceptor reflex), sinus bradycardia, AV nodal block
2. Organophosphate / Nerve Agent Poisoning
Organophosphates inhibit acetylcholinesterase → massive ACh accumulation → overwhelming muscarinic stimulation (SLUDGE syndrome: Salivation, Lacrimation, Urination, Defecation, GI upset, Emesis + bronchorrhea, bradycardia). Atropine reverses all muscarinic features.
- Large, repeated doses required until bronchial secretions terminate
- Combined with pralidoxime (2-PAM) to reactivate acetylcholinesterase
3. Preoperative Antisialagogue
Reduces salivary and respiratory secretions before intubation, bronchoscopy, or upper airway surgery. Prevents secretion-related complications during anesthesia.
4. Reversal of Neuromuscular Blockade (as pretreatment)
Given before neostigmine/pyridostigmine to prevent the bradycardia and excessive secretions caused by cholinesterase inhibitors.
5. Ophthalmic Uses
- Mydriasis (pupillary dilation) for fundal examination
- Cycloplegia (paralysis of accommodation) for refraction in children
- Uveitis - reduces pain by relaxing ciliary muscle and iris sphincter
- Longer duration (7-14 days) than tropicamide, so preferred for therapeutic rather than diagnostic use
6. Bronchospasm (via nebulizer)
Relaxes bronchial smooth muscle; used in acute bronchospasm, especially COPD. Ipratropium (a derivative) is the more commonly used inhaled form due to limited systemic absorption.
7. Preintubation in Children
Historically given to blunt vagal responses during laryngoscopy. Routine use is now not strongly supported by evidence.
8. Anticholinergic Antidote
Reverses toxicity from cholinomimetic drugs (pilocarpine, bethanechol, physostigmine overdose).
Contraindications
| Contraindication | Reason |
|---|---|
| Narrow-angle (acute angle-closure) glaucoma | Mydriasis causes forward displacement of the iris, blocking the canal of Schlemm and raising intraocular pressure acutely |
| Obstructive uropathy / Prostatic hypertrophy / Bladder-neck obstruction | Smooth muscle relaxation worsens urinary outflow obstruction → urinary retention |
| Tachycardia | Atropine increases heart rate further |
| Thyrotoxicosis | Already has elevated heart rate; tachycardia dangerous |
| Myasthenia gravis | Reduces already impaired cholinergic transmission |
| Coronary artery disease | Tachycardia increases myocardial O2 demand and decreases O2 supply - risk of ischemia |
| Heart transplant (for bradycardia) | Transplanted hearts lack vagal reinnervation - atropine is ineffective and should be avoided; use epinephrine or pacing |
| Paralytic ileus / GI obstruction | Reduces peristalsis, worsens obstruction |
Note: Glaucoma, uropathy, tachycardia, and thyrotoxicosis are relative contraindications - they are overridden in life-threatening muscarinic poisoning where benefit outweighs risk.
Harriet Lane Handbook, 23rd ed., p. 1027 | Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 434
Quick Summary Table
| Domain | Key Point |
|---|---|
| Class | Competitive, reversible muscarinic receptor antagonist |
| Prototype | Yes - the prototypical antimuscarinic |
| Receptors blocked | M1, M2, M3 (all muscarinic subtypes) |
| Does NOT block | Nicotinic receptors (NMJ, ganglia) |
| BBB penetration | Yes (tertiary amine) |
| Antidote for atropine toxicity | Physostigmine (crosses BBB) |
| Top indication | Symptomatic bradycardia + organophosphate poisoning |
| Key CI | Narrow-angle glaucoma, prostatic hypertrophy, tachycardia |
| Paradox | Small doses (<0.4 mg IV) can cause bradycardia |
This is a shared conversation. Sign in to Orris to start your own chat.