Ech
Hey! How can I help you today?
Ecg
Asking for Preferences
Reading File
Finding Sources
Searching Images
12-lead ECG anatomy leads placement diagram
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
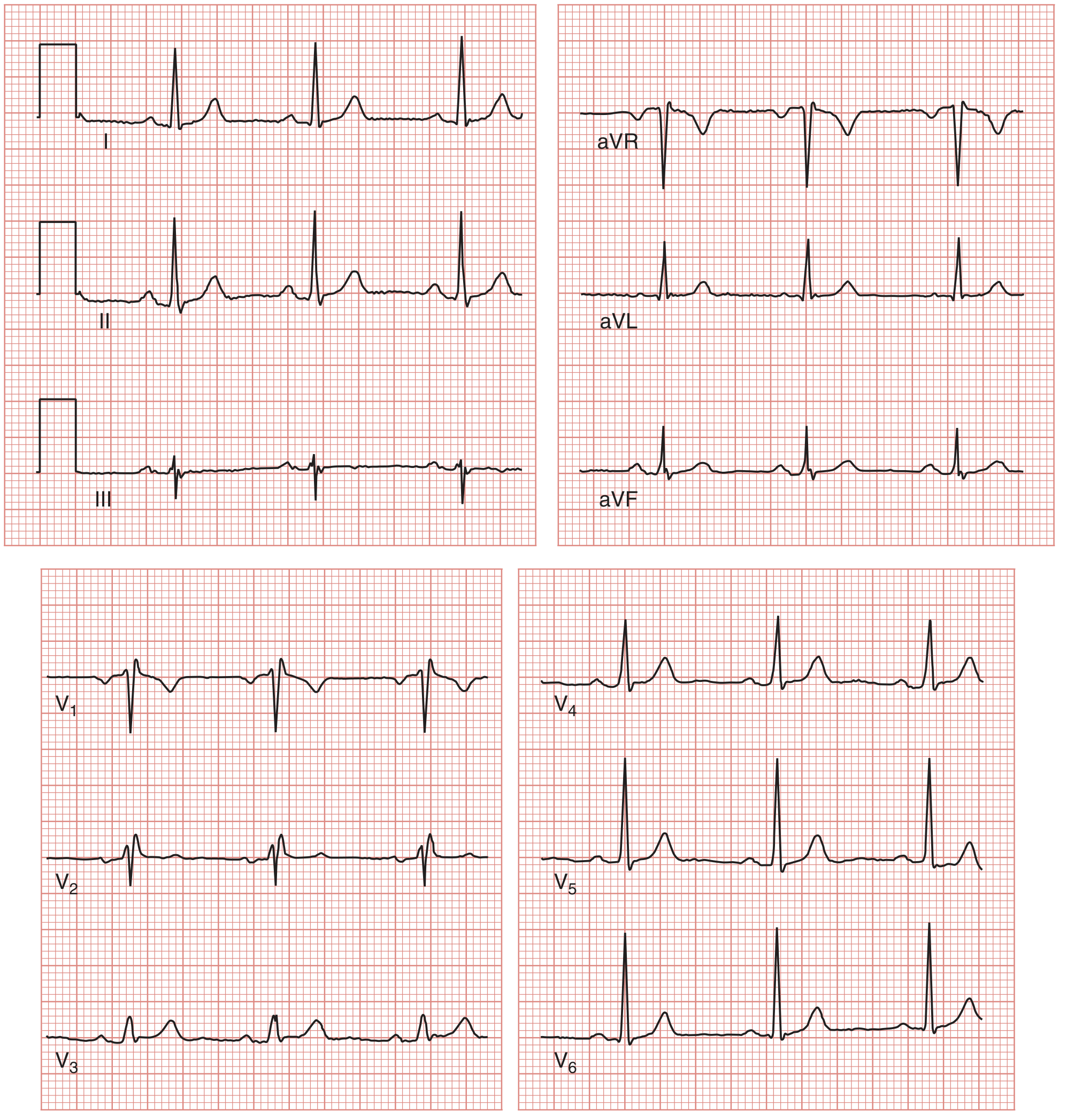
Here's a structured guide to reading a 12-lead ECG, using a systematic approach so you never miss anything.
How to Read a 12-lead ECG
Step 0 — Understand the Paper & Leads
ECG paper:
- Small box = 1 mm = 0.04 s (horizontal) / 0.1 mV (vertical)
- Large box = 5 mm = 0.2 s
- 5 large boxes = 1 second
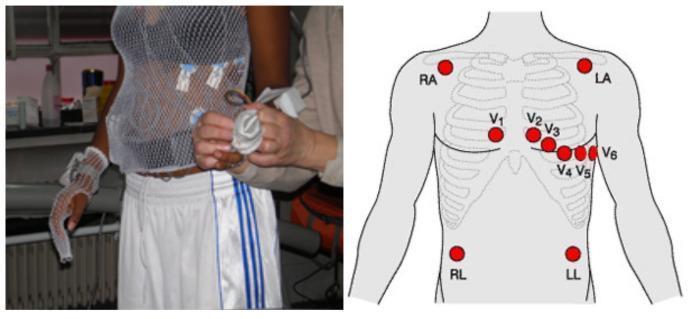
The 12 leads view the heart from different angles:
Electrode placement:
| Group | Leads | View |
|---|---|---|
| Limb (frontal plane) | I, II, III | Left/right/inferior |
| Augmented limb | aVR, aVL, aVF | Right arm, left arm, left foot |
| Precordial (horizontal plane) | V1–V6 | Right → left ventricle |
Precordial placement:
- V1 & V2: 4th intercostal space, right/left of sternum
- V4: 5th intercostal space, midclavicular line
- V3: between V2 & V4
- V5 & V6: anterior/mid-axillary line (same level as V4)
Step 1 — Rate
Quick method (large boxes between R-R interval):
| Large boxes | Rate (bpm) |
|---|---|
| 1 | 300 |
| 2 | 150 |
| 3 | 100 |
| 4 | 75 |
| 5 | 60 |
| 6 | 50 |
Formula: Rate = 300 ÷ (number of large boxes)
Normal = 60–100 bpm
Step 2 — Rhythm
Ask three questions:
- Where is the pacemaker? (Should be SA node → normal sinus rhythm)
- Is it regular? (Are R-R intervals equal?)
- Normal sequence? P wave → QRS → T in every beat?
Normal sinus rhythm: upright P in II, each P followed by QRS, rate 60–100.
Step 3 — Waves, Intervals & Segments
| Component | What it represents | Normal duration |
|---|---|---|
| P wave | Atrial depolarization | < 0.12 s, upright in II |
| PR interval | AV node conduction (P onset → QRS onset) | 0.12–0.20 s (3–5 small boxes) |
| QRS complex | Ventricular depolarization | < 0.12 s (< 3 small boxes) |
| ST segment | Plateau of ventricular action potential | Isoelectric (flat) |
| T wave | Ventricular repolarization | Upright in most leads |
| QT interval | QRS onset → T wave end | Rate-dependent; roughly < 0.44 s |
Step 4 — Axis
Normal QRS axis: −30° to +90° (frontal plane).
Quick check:
- Both leads I and aVF positive → normal axis
- Lead I positive, aVF negative → left axis deviation (LAD)
- Lead I negative, aVF positive → right axis deviation (RAD)
Causes of LAD: left ventricular hypertrophy, left bundle branch block, inferior MI.
Causes of RAD: right ventricular hypertrophy, pulmonary embolism, lateral MI.
Causes of RAD: right ventricular hypertrophy, pulmonary embolism, lateral MI.
Step 5 — Hypertrophy
Left ventricular hypertrophy (LVH): S in V1 + R in V5 or V6 ≥ 35 mm (Sokolow-Lyon)
Right ventricular hypertrophy (RVH): Dominant R in V1, right axis deviation
Step 6 — ST & T Wave Changes
| Finding | Suggests |
|---|---|
| ST elevation | STEMI, pericarditis, Brugada |
| ST depression | NSTEMI, ischemia, digoxin effect |
| T wave inversion | Ischemia, LVH, PE (V1–V4) |
| Peaked T waves | Hyperkalemia, hyperacute STEMI |
Step 7 — Bundle Branch Blocks
- RBBB: QRS ≥ 0.12 s + RSR' ("rabbit ears") in V1, wide S in I & V6
- LBBB: QRS ≥ 0.12 s + broad notched R in I, V5, V6; no septal Q waves
Summary Mnemonic: RRIAWST
Rate → Rhythm → Intervals → Axis → Waves (hypertrophy) → ST changes → Twave/Bundle branch blocks
Source: Medical Physiology (Boron & Boulpaep), Box 21-2 & Figure 21-11
Want me to go deeper on any step — like ST changes in MI, arrhythmia recognition, or axis calculation?
This is a shared conversation. Sign in to Orris to start your own chat.