Hypocalcemia
Reading File
Finding Sources
Searching PubMed
hypocalcemia management diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
hypocalcemia ECG QT prolongation Chvostek Trousseau sign
I now have comprehensive information. Let me compile the full response.
Hypocalcemia
Definition
Hypocalcemia is defined as a serum total calcium < 8.5 mg/dL or an ionized calcium < 2.0 mEq/L (< 1.0 mmol/L). Since ~50% of serum calcium is protein-bound (primarily to albumin), total calcium must be corrected for hypoalbuminemia:
Corrected Ca = measured Ca + 0.8 × (4.0 − serum albumin g/dL)
Ionized calcium is the physiologically active fraction and is not affected by albumin.
Pathophysiology
Calcium homeostasis involves three key players:
- PTH: stimulates bone resorption and renal calcium reabsorption; activates renal 1α-hydroxylase
- Vitamin D (1,25(OH)₂D / calcitriol): increases intestinal calcium absorption
- Calcitonin: opposes PTH
Disruption in any of these axes — deficient PTH production/secretion, PTH resistance, vitamin D deficiency/resistance, or excess calcium loss — can produce hypocalcemia.
Causes
Most Common
| Category | Examples |
|---|---|
| Hypoalbuminemia | Cirrhosis, nephrotic syndrome, malnutrition (most common cause — pseudo-hypocalcemia, ionized Ca is normal) |
| Hypoparathyroidism | Post-thyroidectomy/parathyroidectomy (1–2% of total thyroidectomies), autoimmune, DiGeorge syndrome, infiltrative (iron/copper deposition, granuloma) |
| Vitamin D deficiency | Malabsorption, liver disease, malnutrition, lack of sunlight, anticonvulsants (phenytoin) |
| Chronic renal failure | ↓ 1,25(OH)₂D synthesis, phosphate retention, skeletal resistance to PTH |
| Hypomagnesemia | Impairs PTH secretion and induces peripheral PTH resistance |
| Hyperphosphatemia | Complexes with calcium (tumor lysis syndrome, rhabdomyolysis, renal failure) |
Less Common / Situational
- Acute pancreatitis — calcium soaps precipitate in abdominal cavity; glucagon stimulates calcitonin
- Massive blood transfusion — citrate chelates calcium
- Sepsis / critical illness — usually via hypoalbuminemia
- Drugs: bisphosphonates, calcitonin, foscarnet, cinacalcet, phenytoin, heparin, glucagon, protamine
- Toxins: hydrofluoric acid, ethylene glycol (complex and chelate calcium)
- Respiratory alkalosis — shifts ionized Ca to bound form (↓ ionized without changing total Ca)
- Hungry bone syndrome — post-parathyroidectomy rapid bone remineralization
- Pseudohypoparathyroidism (PHP / Albright hereditary osteodystrophy) — end-organ PTH resistance due to Gsα protein defect; high PTH + low Ca + high phosphate
Clinical Features
Neuromuscular (dominant)
- Perioral and digital paresthesias
- Muscle cramping, carpopedal spasm
- Tetany → laryngospasm (life-threatening), bronchospasm
- Hyperreflexia, anxiety, confusion, psychosis, seizures (severe)
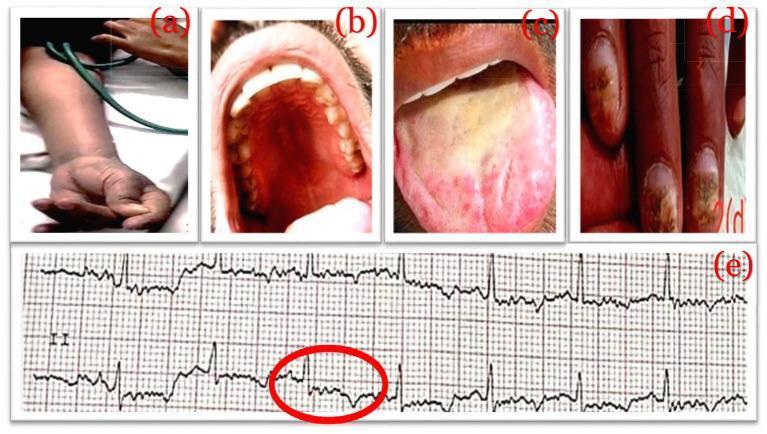
Classic Signs
- Chvostek sign: tap the facial nerve just anterior to the ear → ipsilateral facial muscle twitch. Sensitive but not specific (present in ~25% of normals)
- Trousseau sign: inflate BP cuff 20 mmHg above systolic for 3 minutes → carpal spasm ("main d'accoucheur" — wrist flexion, MCP flexion, IP extension, thumb adduction). More specific for hypocalcemia
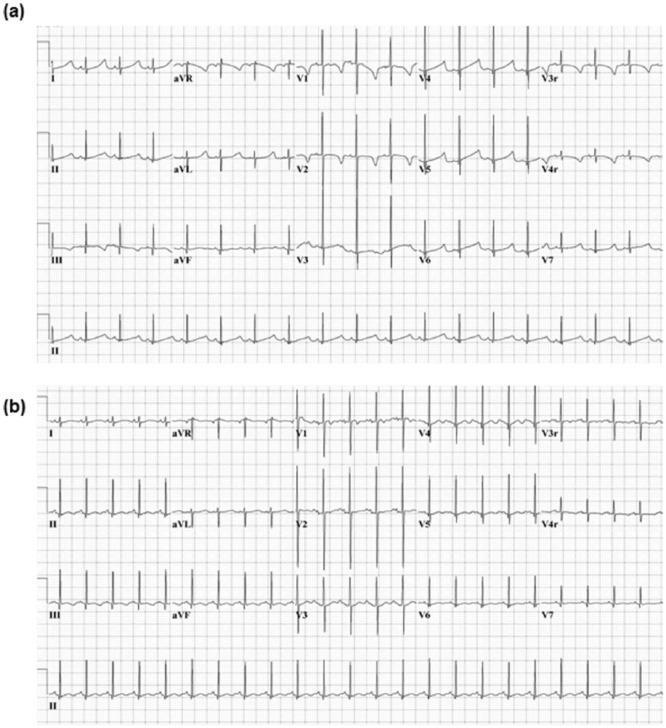
Cardiovascular
- QT prolongation (due to ST segment lengthening) — the most common ECG finding
- Can mimic acute MI (J-point elevation)
- Ventricular dysrhythmias, CHF, hypotension, cardiac collapse
- Patients with Ca < 8.95 mg/dL have a 2.3× higher risk of sudden cardiac death
Chronic Manifestations
- Cataracts, poor dentition, dry skin, coarse hair, pruritus
- Extrapyramidal symptoms (PHP), basal ganglia calcification
- Alopecia, candidiasis (seen in autoimmune hypoparathyroidism)
- Rickets (children) / osteomalacia (adults) if vitamin D-related
ECG in Hypocalcemia
Diagnostic Workup
| Test | Rationale |
|---|---|
| Serum total Ca | Initial screen |
| Ionized Ca | Most accurate; unaffected by albumin |
| Serum albumin | Corrected calcium calculation |
| PTH | Low/absent → hypoparathyroidism; elevated → vitamin D deficiency, renal failure, PHP |
| Phosphate | High + low Ca → hypoparathyroidism or renal failure; low + low Ca → vitamin D deficiency |
| Magnesium | Hypomagnesemia impairs PTH; must be corrected first |
| 25(OH)D, 1,25(OH)₂D | Assess vitamin D status |
| Creatinine/eGFR | Renal failure assessment |
| ECG / cardiac monitoring | QT interval; dysrhythmia surveillance |
Key laboratory pattern summary:
| Disorder | Ca | PTH | Phosphate | 25(OH)D | 1,25(OH)₂D |
|---|---|---|---|---|---|
| Hypoparathyroidism | ↓ | ↓/absent | ↑ | Normal | ↓ |
| Pseudohypoparathyroidism | ↓ | ↑↑ | ↑ | Normal | ↓ |
| Vitamin D deficiency | ↓ | ↑ (2° HPT) | ↓ | ↓ | ↓/N/↑ |
| Chronic renal failure | ↓ | ↑ (2° HPT) | ↑ | Variable | ↓ |
| Hypoalbuminemia | ↓ total (ionized normal) | Normal | Normal | Normal | Normal |
Management
Acute / Symptomatic (IV Calcium)
- Calcium gluconate 1–2 g IV (92 mg elemental Ca per 10 mL amp) over 10 minutes → preferred peripherally (less caustic)
- Calcium chloride 1 g IV (272 mg elemental Ca) → preferred in cardiac arrest; use central access (caustic to veins)
- 100–300 mg elemental calcium over 5–30 min → raises ionized Ca by 0.5–1.5 mEq/L
- Follow with calcium gluconate infusion (10–15 mg/kg over 4–6 hrs) to maintain effect
- Most patients requiring IV calcium require hospital admission for monitoring
Concurrent Corrections
- Correct hypomagnesemia first — hypocalcemia refractory to calcium replacement until Mg is repleted
- Manage hyperphosphatemia with phosphate binders
- Treat underlying alkalosis
Chronic / Asymptomatic
- Oral calcium (calcium carbonate 1–3 g/day in divided doses; best absorbed with food)
- Vitamin D supplementation: cholecalciferol (D₃) for deficiency; calcitriol (1,25(OH)₂D) for hypoparathyroidism and chronic renal failure (bypasses activation steps)
- Thiazide diuretics: increase renal calcium reabsorption — useful adjunct in hypoparathyroidism
- Recombinant PTH (teriparatide / PTH 1-84): for chronic hypoparathyroidism unresponsive to conventional therapy
- Target ionized/corrected Ca in low-normal range (8.0–8.5 mg/dL) to avoid hypercalciuria
Special Scenarios
| Situation | Key Point |
|---|---|
| Post-thyroidectomy | Occurs in 1–2% of total thyroidectomies; monitor Ca and PTH intraoperatively/postoperatively |
| Massive transfusion | Citrate chelation; monitor ionized Ca; supplement empirically in hepatic failure |
| HF exposure (hydrofluoric acid) | Profound hypocalcemia; requires topical/IV/intra-arterial calcium |
| Neonatal hypocalcemia | First 72 hours (early) vs. end of 1st week (late); late type linked to high-phosphate formula or maternal hyperparathyroidism |
| Pancreatitis | Degree of hypocalcemia correlates with severity (Ranson criteria) |
Sources: Rosen's Emergency Medicine, pp. 2524–2526 | Henry's Clinical Diagnosis & Management by Laboratory Methods, pp. 253–254 | Textbook of Family Medicine, 9e, p. 1601
Hypoalbuminemia and hypocalcemia symptoms
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
This is the crux of the question. I now have everything needed for a precise, clinically important answer.
Hypoalbuminemia + Hypocalcemia: Why There Are Usually No Symptoms
This is one of the most important clinical distinctions in calcium disorders.
The Key Concept: "Pseudohypocalcemia"
When low serum calcium is caused solely by hypoalbuminemia, the patient is typically asymptomatic — because the physiologically active fraction of calcium (ionized/free Ca²⁺) remains normal.
About 50% of total serum calcium is protein-bound, primarily to albumin. The other 50% is ionized (free) calcium — the form that actually drives neuromuscular excitability, cardiac conduction, and all calcium-dependent cellular processes. When albumin falls, total calcium drops proportionally, but ionized calcium is untouched.
This is called pseudohypocalcemia — a low total calcium lab value that does not represent true calcium deficiency.
Corrected Calcium Formula
To unmask whether the low total calcium reflects real hypocalcemia, you apply the correction:
Corrected Ca (mg/dL) = Measured Ca + 0.8 × (4.0 − serum albumin g/dL)
- If the corrected calcium is normal → the low total Ca is entirely explained by hypoalbuminemia → ionized Ca is normal → patient should have no hypocalcemia symptoms
- If the corrected calcium is still low → true hypocalcemia coexists → symptoms may be present
Example (from Roberts & Hedges' Clinical Procedures in Emergency Medicine):
A malnourished man has total Ca = 7.5 mg/dL, albumin = 2.0 g/dL.
Corrected Ca = 7.5 + 0.8 × (4.0 − 2.0) = 7.5 + 1.6 = 9.1 mg/dL → Normal
→ No true hypocalcemia, no symptoms expected.
Limitations of the Correction Formula
The albumin-correction formula is a simplification. Its reliability deteriorates in:
- Very high or very low albumin concentrations
- ICU patients with multiple organ failure (calcium distribution is altered by pH, free fatty acids, bilirubin, heparin, temperature)
- Hemodialysis patients (disease-specific equations perform better)
- Patients with abnormal proteins (e.g., myeloma — globulins also bind calcium)
In these situations, direct measurement of ionized calcium is the gold standard. Ionized Ca < 1.0 mmol/L (< 2.0 mEq/L) confirms true hypocalcemia regardless of albumin.
When Symptoms DO Appear in Hypoalbuminemic Patients
Symptoms of hypocalcemia (tetany, paresthesias, Chvostek/Trousseau signs, QT prolongation, seizures) occur when ionized calcium falls, not simply when total calcium falls. This happens when:
| Scenario | Mechanism |
|---|---|
| Alkalosis (respiratory or metabolic) | ↑ pH increases calcium binding to albumin → ↓ ionized Ca even with normal total Ca |
| Co-existing true hypocalcemia | Vitamin D deficiency, hypoparathyroidism, Mg deficiency alongside hypoalbuminemia |
| Massive citrate load (blood transfusions) | Citrate chelates ionized Ca directly |
| Hyperphosphatemia | Phosphate complexes with ionized Ca |
Alkalosis is particularly relevant in hypoalbuminemic patients because many underlying conditions (cirrhosis, sepsis, anxiety, pain) cause respiratory alkalosis, which can convert borderline pseudohypocalcemia into true symptomatic hypocalcemia by shifting ionized Ca into the bound fraction.
Summary Table
| Situation | Total Ca | Ionized Ca | Symptoms? |
|---|---|---|---|
| Pure hypoalbuminemia | ↓ | Normal | None (pseudohypocalcemia) |
| True hypocalcemia (normal albumin) | ↓ | ↓ | Yes |
| Hypoalbuminemia + alkalosis | ↓ | ↓ | Yes |
| Hypoalbuminemia + true hypoCa | ↓↓ | ↓ | Yes |
| Dehydration/hemoconcentration | ↑ (falsely) | Normal | None |
Bottom line: A low total calcium in a hypoalbuminemic patient almost always represents pseudohypocalcemia — the ionized fraction is normal and the patient is symptom-free. Always correct for albumin (or measure ionized Ca directly) before diagnosing or treating hypocalcemia.
Sources: Harrison's Principles of Internal Medicine, 22e | Tietz Textbook of Laboratory Medicine, 7e | Henry's Clinical Diagnosis & Management by Laboratory Methods | Bradley and Daroff's Neurology in Clinical Practice
Focal seizures
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.