Rheumatic fever complete long answer for pathology MBBS exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Robbins Pathologic Basis of Disease. Let me now compile the complete long answer for the MBBS pathology exam.
Rheumatic Fever - Complete Long Answer (Pathology MBBS)
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
Definition
Rheumatic fever (RF) is an acute, immunologically mediated, multisystem inflammatory disease that classically occurs 2-3 weeks after group A beta-hemolytic streptococcal (GABHS) pharyngitis. It may progress to chronic rheumatic heart disease (RHD), which is among the most important causes of acquired heart disease in developing countries.
Etiology and Epidemiology
- Causative organism: Group A beta-hemolytic Streptococcus pyogenes (specifically rheumatogenic strains)
- Inciting site: Pharyngeal infection (not skin infection)
- Age group: Most commonly affects children between 5 and 15 years; first attacks can occur in middle to later life
- Incidence: Only 0.3% to 3% of individuals who experience streptococcal pharyngitis develop RF, indicating genetic susceptibility
- Geographic distribution: Remains a major public health problem in low-resource countries and in crowded, economically depressed urban areas; declined markedly in developed nations due to improved sanitation and antibiotic use
Pathogenesis (Molecular Mimicry)
The pathogenesis of RF is based on cross-reactive immune responses (molecular mimicry):
- Initial infection: Group A streptococcus infects the pharynx and expresses M proteins (virulence factors on the bacterial surface)
- Immune sensitization: The host generates antibodies and CD4+ T cells directed against streptococcal M proteins
- Cross-reactivity: These antibodies and T cells cross-react with host cardiac antigens - pericardial, myocardial, or valvular proteins - because of structural similarity between streptococcal M protein epitopes and cardiac self-antigens
- Tissue damage mechanism:
- Antibody binding to cardiac antigens activates complement
- Fc-receptor-bearing cells (neutrophils and macrophages) are recruited
- CD4+ T cell cytokine production leads to macrophage activation (within Aschoff bodies)
- Combined antibody-mediated and T cell-mediated reactions cause tissue injury
- Key proof of immune basis: Streptococci are completely absent from the cardiac lesions
- Delay: The 2-3 week latent period between infection and symptoms corresponds to the time needed to mount an adequate immune response
- Genetic susceptibility: An intrinsic genetic factor predisposes a small subset of infected individuals to develop the cross-reactive immune response
Morphology (Pathological Changes)
1. Acute Rheumatic Fever - Pancarditis
During acute RF, focal inflammatory lesions are found in all three layers of the heart:
A. Aschoff Bodies (PATHOGNOMONIC)
The hallmark of rheumatic carditis. These are:
- Focal granulomatous lesions found in the myocardium (interstitium)
- Composition: Foci of T lymphocytes, occasional plasma cells, and activated macrophages
- Central zone: Area of fibrinoid necrosis (collagen surrounded by activated macrophages)
- Characteristic cells - Anitschkow cells (Anitschkow myocytes / Caterpillar cells):
- Plump activated macrophages with abundant cytoplasm
- Central round-to-ovoid nuclei, occasionally binucleate
- Chromatin condenses into a central, slender, wavy ribbon = "caterpillar cells" or "owl-eye" nuclei
- Giant cells (Aschoff giant cells) may be present
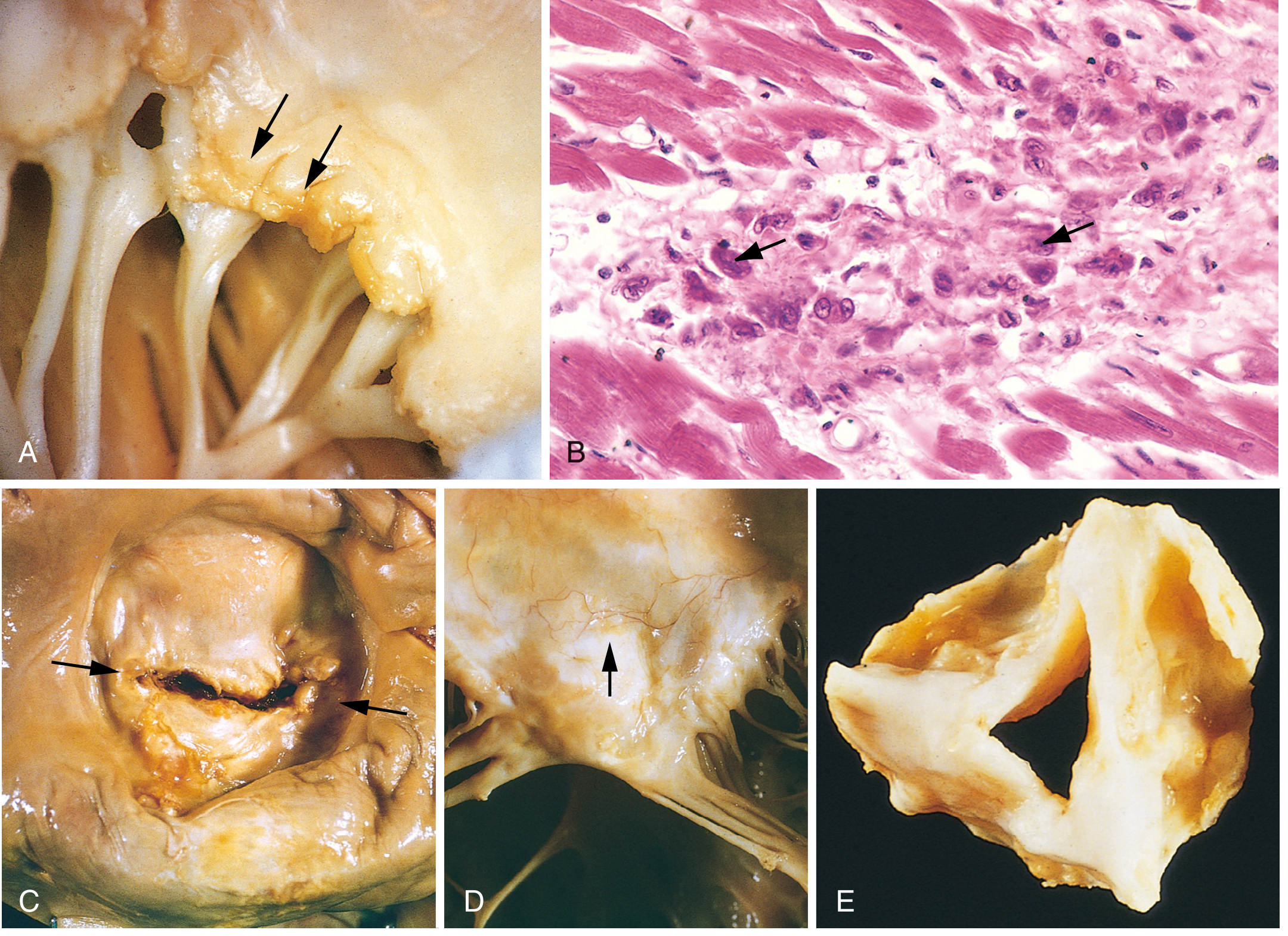
Fig. 12.22 (B) from Robbins Pathologic Basis of Disease shows the microscopic appearance of an Aschoff body with characteristic Anitschkow cells (arrows).
B. Pericarditis
- Fibrinous or serofibrinous pericarditis - produces a "bread-and-butter" appearance on gross examination
- Usually resolves without significant sequelae
C. Myocarditis
- Diffuse inflammation with Aschoff bodies throughout the myocardial interstitium
- Can cause cardiac dilation leading to functional mitral valve insufficiency or heart failure
- Accounts for the 1-2% mortality in fulminant RF
D. Endocarditis (Valvulitis) - Most Clinically Significant
- Inflammation of the endocardium and left-sided valves
- Fibrinoid necrosis within the valve cusps or tendinous cords
- Verrucae: Small (1-2 mm), firm, warty vegetations overlying the necrotic foci
- Located along the lines of valve closure
- Single row arrangement
- These are sterile, unlike infective endocarditis vegetations
- MacCallum plaques: Irregular thickenings on the posterior wall of the left atrium, caused by subendocardial lesions (exacerbated by regurgitant jet injury)
2. Chronic Rheumatic Heart Disease (RHD)
Caused by repeated episodes of RF leading to cumulative valve damage and progressive fibrosis:
Mitral Valve (Most Commonly Affected)
- Affected in virtually 100% of cases of chronic RHD
- Isolated mitral involvement: ~two-thirds of cases
- Mitral + aortic involvement: ~25% of cases
Cardinal anatomic changes of the mitral valve:
- Leaflet thickening - due to fibrosis and neovascularization
- Commissural fusion - fusion of adjacent leaflet edges
- Shortening of leaflets - overall reduction in valve area
- Thickening and fusion of the chordae tendineae - cords become short, thick, and matted
- "Fish-mouth" or "button-hole" stenosis - the classic appearance of severe mitral stenosis due to calcification and fibrous bridging across commissures
- RHD is virtually the only cause of mitral stenosis
Consequences of Mitral Stenosis:
- Progressive left atrial dilation
- Mural thrombi in left atrium (risk of systemic embolism)
- Pulmonary hypertension - from chronic pulmonary venous congestion
- Pulmonary vascular and parenchymal changes
- Right ventricular hypertrophy (cor pulmonale)
- Left ventricle is largely unaffected in pure mitral stenosis
Aortic Valve
- Involved in ~25% of RHD cases (usually with mitral)
- Thickening and fusion of cusps, leading to aortic stenosis or regurgitation
Microscopy in Chronic RHD:
- Organization of acute inflammation
- Postinflammatory neovascularization
- Transmural fibrosis obliterating normal leaflet architecture
- Aschoff bodies are rarely seen in surgical/autopsy specimens from chronic RHD (due to the long intervals between acute episodes and chronic deformity)
Clinical Features
Major Jones Criteria (Revised)
| Feature | Details |
|---|---|
| Carditis | Pancarditis: pericardial friction rubs, tachycardia, arrhythmias, new murmur |
| Migratory polyarthritis | Large joints, one after another; painful, swollen, then spontaneously subsides; no residual disability |
| Sydenham chorea | Neurological disorder with involuntary rapid movements ("St. Vitus dance") |
| Subcutaneous nodules | Firm, painless, on extensor surfaces of extremities |
| Erythema marginatum | Irregular, circinate skin rash with central clearing |
Minor Jones Criteria
- Fever
- Arthralgia
- Elevated acute-phase reactants (ESR, CRP, leukocytosis)
- Prolonged PR interval on ECG
- Evidence of preceding streptococcal infection (elevated ASO titer, positive throat culture)
Diagnosis (Revised Jones Criteria, 2015)
- Evidence of preceding GABHS infection, PLUS
- 2 major manifestations, OR
- 1 major + 2 minor manifestations
Laboratory Findings
| Test | Finding |
|---|---|
| ASO titer (Antistreptolysin O) | Most useful; rises 4-6 weeks after infection; positive in most patients |
| Anti-DNase B | Remains elevated longer than ASO |
| Throat culture | Often negative by the time RF manifests |
| ESR, CRP | Elevated (acute phase reactants) |
| ECG | Prolonged PR interval (1st degree AV block) |
| Echocardiography | Valvular abnormalities, evidence of carditis |
Comparison: Vegetative Endocarditis Forms (MBBS Exam Favourite)
| Feature | Rheumatic Fever | Infective Endocarditis | NBTE |
|---|---|---|---|
| Location of vegetations | Along line of closure | On cusps/irregular | Along line of closure |
| Size | Small (1-2 mm) | Large, bulky, friable | Small, flat |
| Organisms present | None (sterile) | Yes | None |
| Valve destruction | Minimal acutely | Extensive | Minimal |
| Character | Firm, warty | Friable, destructive | Flat, non-destructive |
Prognosis and Complications
- Recurrence: After initial RF, there is increased vulnerability to reactivation with each subsequent streptococcal pharyngitis; damage is cumulative with each episode
- Chronic RHD: Manifests years to decades after the initial attack
- Complications of chronic RHD:
- Cardiac murmurs (mitral stenosis = most common valve lesion)
- Atrial fibrillation (especially with mitral stenosis)
- Thromboembolic complications (stroke)
- Infective endocarditis (superimposed on damaged valves)
- Heart failure
- Mortality: ~1-2% die from fulminant RF cardiac involvement in the acute phase
Prevention
| Type | Measure |
|---|---|
| Primary prevention | Prompt antibiotic treatment of GABHS pharyngitis (penicillin for 10 days) |
| Secondary prevention | Long-term penicillin prophylaxis to prevent recurrent streptococcal infections and further valve damage |
Summary for Quick Recall
RF = GABHS pharyngitis → molecular mimicry → cross-reactive immunity
→ M protein antibodies attack cardiac antigens
→ PANCARDITIS:
Pericarditis (bread-and-butter)
Myocarditis (Aschoff bodies - Anitschkow/caterpillar cells)
Endocarditis (small verrucae on line of closure, MacCallum plaques)
→ Repeated attacks → Chronic RHD
Mitral stenosis ("fish-mouth") → LA dilation → AF → embolism
Aschoff bodies = T cells + plasma cells + Anitschkow macrophages
Key exam points to remember:
- Aschoff body is pathognomonic of rheumatic carditis
- Anitschkow cells (caterpillar cells) are activated macrophages, not cardiomyocytes
- RHD is virtually the only cause of mitral stenosis
- Vegetations of RF are small, sterile, on the line of closure (unlike large, friable, destructive vegetations of infective endocarditis)
- Pathogenesis = molecular mimicry (cross-reactivity between M protein and cardiac antigens)
- Streptococci are absent from RF lesions (proving immune basis)
- MacCallum plaques = left atrial wall subendocardial lesions
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), pp. 525-527
Inflammatory bowel disease complete long answer for pathology MBBS exam
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.