Define Transformation zone, describe it's evaluation, what are the recent guidelines for screening of cervical cancer
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"cervical cancer screening" guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Searching the Web
USPSTF ASCCP ACS cervical cancer screening guidelines 2024 2025 HPV primary
Reading File
Finding Sources
Loading Image
Reading Web Page
https://www.asccp.org/wp-content/uploads/2026/01/Practice-Ad…
I now have all the information needed for a comprehensive, well-cited answer. Let me compile it.
Transformation Zone of the Cervix
Definition and Anatomy
The transformation zone (TZ) is the area of the cervix located between two distinct epithelial boundaries:
- The original squamocolumnar junction (SCJ) - the location where columnar epithelium originally met squamous epithelium at birth/menarche
- The new (current) SCJ - where the current active interface between columnar and squamous epithelium lies
Within this zone, columnar epithelium that has been exposed to the acidic vaginal environment undergoes squamous metaplasia - a physiological replacement of columnar cells by maturing squamous cells. This process produces features visible at colposcopy: gland openings, nabothian cysts, and islands of metaplastic epithelium. The TZ is the most common site of cervical carcinoma, as metaplastic cells in active transformation are most vulnerable to HPV-mediated oncogenic change.
- Color Atlas of Human Anatomy, Vol. 2 - Internal Organs, p. 458
- Schwartz's Principles of Surgery, 11th Ed., p. 1818
How the TZ Changes with Age
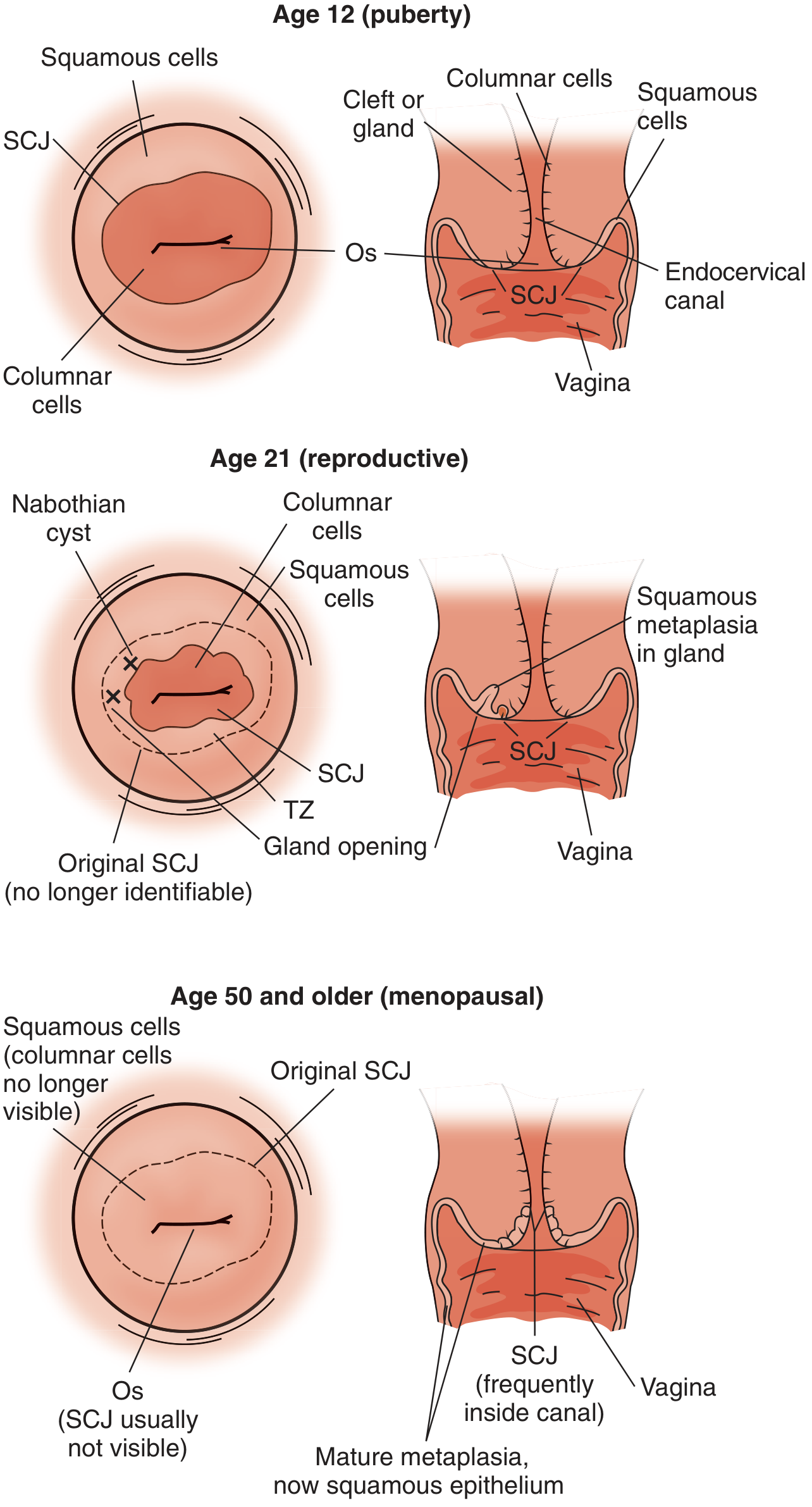
As shown above:
-
Puberty/young women: Large ectropion; the SCJ is on the ectocervix and easily visible; the TZ is wide and fully exposed
-
Reproductive age: As metaplasia matures, the new SCJ migrates toward the os; the TZ contains nabothian cysts, gland openings, and islands of squamous metaplasia
-
Menopause/older women: Estrogen withdrawal causes the SCJ and TZ to recede into the endocervical canal, often making them invisible on colposcopy
-
Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., Fig. 151-1
Types of Transformation Zone
The IFCPC (International Federation for Colposcopy and Cervical Pathology) classifies the TZ into three types based on the visibility of the SCJ:
| Type | Description | Colposcopy Adequacy |
|---|---|---|
| Type 1 | Entirely ectocervical; SCJ fully visible; may be small or large | Adequate |
| Type 2 | Has an endocervical component; SCJ still fully visible after exposing the canal | Adequate |
| Type 3 | SCJ not visible; partially or fully within the endocervical canal | Inadequate - may require ECC or LEEP conization |
Evaluation of the Transformation Zone
Colposcopy
Colposcopy is the primary method for TZ evaluation and is indicated after abnormal cytology, a positive HPV test, or any suspicious cervical lesion.
Procedure:
- The cervix is visualized under 2x-15x magnification
- Cervical mucus is removed
- 3%-5% acetic acid is applied - dehydrates cells, causing dysplastic cells with dense nuclei to appear acetowhite (acetic acid whitening)
- A green filter enhances vascular patterns, making atypical vessels appear darker against the epithelium
Colposcopic findings that warrant biopsy:
- Acetowhitening (especially dense white)
- Punctation (stippled red dots from looped capillaries seen end-on)
- Mosaicism (tiles of acetowhite epithelium divided by vessel grid)
- Atypical vessels (irregular caliber, branching)
Lugol's iodine (Schiller's test): Normal mature squamous epithelium is rich in glycogen and stains dark mahogany brown. High-grade CIN lesions have poorly differentiated cells with low glycogen and remain Lugol's non-staining (yellow) - marking areas for biopsy.
Adequacy of colposcopy: For colposcopy to be deemed adequate, the entire SCJ must be visible. If it is obscured within the canal (Type 3 TZ), an endocervical curettage (ECC) or LEEP conization may be required.
- Schwartz's Principles of Surgery, 11th Ed., p. 1818-1819
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., Chapter 137
Pap Smear (Cervical Cytology)
The Pap smear samples cells from the TZ - both the ectocervical component and the endocervical canal. Proper sampling of the entire TZ is essential: the presence of endocervical/metaplastic cells confirms TZ sampling has occurred.
LEEP (Loop Electrosurgical Excision Procedure)
LEEP completely removes the TZ with a wire loop and is both diagnostic and therapeutic. It is preferred over ablative methods (e.g., cryotherapy) when:
-
High-grade lesion (CIN 2-3) involves 3+ quadrants
-
Atypical vessels are prominent
-
Lesion not covered by cryoprobe
-
Recurrent CIN after previous therapy
-
Colposcopy is unsatisfactory (Type 3 TZ - LEEP conization)
-
Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., Chapter 149
Recent Cervical Cancer Screening Guidelines (2024-2025)
USPSTF 2018 (Current Formal Recommendation; Draft 2024 Update Pending)
| Age Group | Recommendation |
|---|---|
| < 21 years | No screening regardless of sexual history |
| 21-29 years | Cytology (Pap) alone every 3 years |
| 30-65 years | Cytology every 3 years OR hrHPV testing alone every 5 years OR co-testing every 5 years |
| > 65 years | Discontinue if adequate prior negative screening (3 negative Paps or 2 negative co-tests in last 10 years) |
| Post-hysterectomy (benign) | Discontinue vaginal vault Pap smears |
The 2024 USPSTF draft update (under public comment) endorses primary HPV testing as the preferred option for women 30-65, and ACS/ASCCP support this direction.
American Cancer Society (ACS) 2020 Guidelines (Updated December 2025)
The ACS 2025 update introduced important changes for average-risk individuals ages 25-65:
- Start age: 25 years (instead of 21), regardless of sexual debut
- Preferred modality: Primary high-risk HPV (hrHPV) testing alone every 5 years - clinician-collected cervical specimen preferred
- Acceptable alternatives:
- Co-testing (HPV + cytology) every 5 years
- Cytology alone every 3 years (if HPV testing unavailable)
- Self-collected vaginal HPV testing is now an acceptable alternative when clinician-collected samples are difficult to obtain; however, positive self-collected tests still require a clinician-collected cervical cytology for triage before colposcopy
- Exit screening: After age 65, screening can be discontinued if there is documented adequate prior screening and the individual is not immunocompromised
ASCCP 2025 Enduring Guidelines - Self-Collection (Published 2025)
- Three FDA-approved tests exist for primary HPV screening on self-collected specimens (as of May 2024/2025)
- Self-collected samples are slightly less sensitive than clinician-collected specimens
- Positive self-collected HPV results still require standard clinical follow-up (speculum exam, colposcopy, histology)
- PMID 39982254 - Wentzensen et al. 2025, J Low Genit Tract Dis
- PMID 39791481 - Massad et al. 2025 on extended HPV genotyping management
Special Populations (Increased Risk - Screen More Frequently)
- HIV-positive: Every 6 months in the first year after diagnosis, then annually
- Immunosuppressed (organ transplant, prolonged steroid use)
- DES daughters (in utero diethylstilbestrol exposure) - require colposcopy
- History of CIN 2 or greater: Annual screening for 20 years after treatment, even if this extends beyond age 65
Summary: TZ at a Glance
| Feature | Detail |
|---|---|
| Location | Between original and new SCJ |
| Process | Active squamous metaplasia |
| Significance | Most common site of cervical cancer |
| Visualization | Colposcopy with acetic acid / Lugol's |
| Vulnerability | Metaplastic cells susceptible to HPV |
| Age effect | Migrates into canal with age/menopause |
The transformation zone is the target of all cervical cancer screening strategies because it is where virtually all cervical squamous cell carcinomas and adenocarcinomas arise. Adequate colposcopic evaluation requires full visualization of the TZ and SCJ; failure to achieve this mandates endocervical sampling or excisional procedures.
- Berek & Novak's Gynecology, p. 846-848
- Schwartz's Principles of Surgery, 11th Ed.
- ACS 2025 Updated Cervical Cancer Screening Guidelines (ASCCP Practice Advisory, December 2025)
- USPSTF Cervical Cancer Screening Recommendation
This is a shared conversation. Sign in to Orris to start your own chat.