explain me liver anatomy
Reading File
Finding Sources
Searching the Web
liver anatomy overview lobes segments vasculature
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a thorough overview of liver anatomy, drawn from Bailey & Love's Surgery, Schwartz's Principles of Surgery, Gray's Anatomy for Students, Guyton & Hall Medical Physiology, and Medical Physiology (Boron & Boulpaep).
Liver Anatomy
1. General Features
The liver is the largest organ in the body, weighing approximately 1,500 g (~2% of total body weight) in the average adult. It sits in the right upper quadrant (right hypochondrium) of the abdominal cavity, tucked beneath the right hemidiaphragm and protected by the rib cage. Its shape is that of a wedge or prism, with the base to the right and the apex pointing left. It is reddish-brown in color and enclosed in a tough fibrous capsule called Glisson's capsule.
2. Surfaces
- Diaphragmatic (anterior/superior) surface - smooth and convex, molds to the undersurface of the diaphragm
- Visceral (posterior/inferior) surface - irregular, bears impressions from adjacent organs (stomach, duodenum, right kidney, right adrenal, hepatic flexure of the colon)
- The bare area on the posterior surface is a region not covered by peritoneum, where the liver is in direct contact with the diaphragm
3. Ligaments and Peritoneal Attachments
The liver is held in position by peritoneal reflections forming several ligaments:
| Ligament | Description |
|---|---|
| Falciform ligament | Connects liver to the anterior abdominal wall; separates the left lateral segment from the left medial segment along the umbilical fissure. Its lower free edge contains the ligamentum teres (obliterated umbilical vein) |
| Ligamentum teres (round ligament) | Remnant of the obliterated umbilical vein; enters the liver at the umbilical fissure |
| Ligamentum venosum (Arantius' ligament) | Remnant of the ductus venosus; lies deep between the caudate lobe and the left lateral segment |
| Left triangular ligament | Fixes the left lobe to the diaphragm; dividing it mobilizes the liver from the diaphragm |
| Right triangular ligament | Fixes the right lobe to the right hemidiaphragm |
| Coronary ligaments | Extend from the triangular ligaments anteriorly; the right coronary ligament also anchors the liver to the right retroperitoneum (right kidney region) |
| Lesser omentum (hepatoduodenal + gastrohepatic ligaments) | Connects the liver to the stomach and duodenum; the right free edge of the hepatoduodenal ligament contains the portal triad (bile duct, hepatic artery, portal vein) |
The foramen of Winslow (epiploic foramen) lies posterior to the hepatoduodenal ligament and connects the lesser sac. Clamping this ligament (the Pringle maneuver) controls all vascular inflow to the liver.
4. Lobes - Morphological vs. Functional Division
Morphological (classical) lobes
The external surface shows four lobes separated by visible fissures:
- Right lobe - largest, makes up 60-70% of liver mass
- Left lobe - smaller, separated from the right by the falciform ligament (on the anterior surface) and the ligamentum venosum (on the posterior surface)
- Caudate lobe (lobe of Spigelius) - on the posterior surface, between the IVC on the right and the ligamentum venosum on the left, anterior to the porta hepatis
- Quadrate lobe - on the inferior surface, between the gallbladder fossa on the right and the ligamentum teres on the left
Functional (surgical) division - Cantlie's line
The true functional division is a plane called Cantlie's line - an imaginary line from the gallbladder fossa to the inferior vena cava (IVC). This divides the liver into the right and left hemilivers of roughly equal functional mass. The middle hepatic vein runs in this plane. Importantly, the falciform ligament does NOT separate the functional right and left lobes.
5. Segmental Anatomy - Couinaud's Classification
The most surgically important classification was developed by French surgeon Claude Couinaud in the 1950s based on portal vein and hepatic vein branching. The liver is divided into 8 functionally independent segments, each with its own portal supply, hepatic arterial supply, bile drainage, and hepatic venous outflow. Segments are numbered I through VIII clockwise:
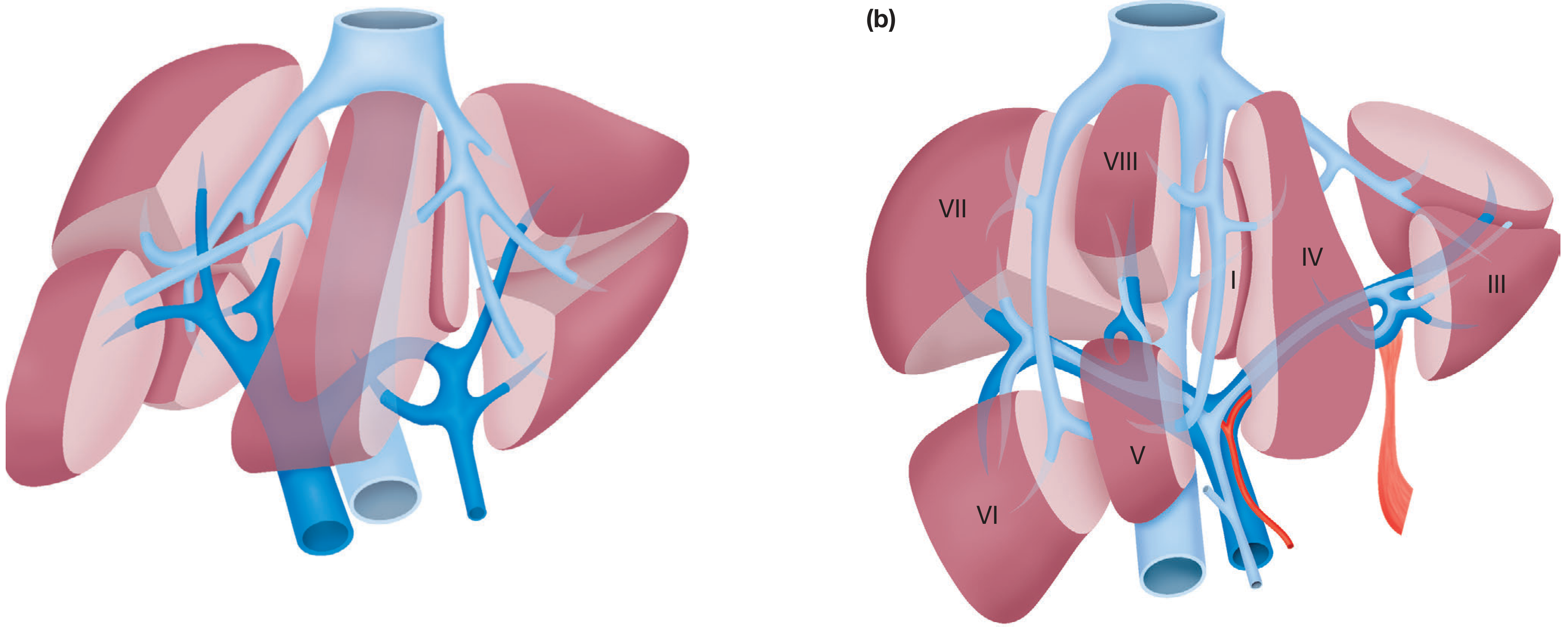
Couinaud's segments - functional division of the liver (Bailey & Love's Surgery)
| Segment | Location |
|---|---|
| I | Caudate lobe (posterior, drains independently into IVC) |
| II | Left lobe - left lateral, superior |
| III | Left lobe - left lateral, inferior |
| IV (IVa/IVb) | Left lobe - left medial segment; IVa is cephalad, IVb is caudad (adjacent to gallbladder) |
| V | Right lobe - right anterior, inferior |
| VI | Right lobe - right posterior, inferior |
| VII | Right lobe - right posterior, superior |
| VIII | Right lobe - right anterior, superior |
- Left lobe = segments II + III (left lateral) + IV (left medial)
- Right lobe = segments V + VI + VII + VIII
- Right hepatectomy removes segments V, VI, VII, VIII; leaving I, II, III, IV
- Each segment can be resected independently without disrupting blood supply or bile drainage to the remaining segments
6. Blood Supply
The liver has a dual blood supply, receiving approximately 1,350 mL/min total (27% of resting cardiac output):
Portal Vein (~80% of hepatic blood flow)
- Formed behind the neck of the pancreas by the union of the superior mesenteric vein and the splenic vein
- Carries nutrient-rich, partially deoxygenated blood from the gastrointestinal tract and spleen
- Portal pressure is normally ~9 mmHg (rises in cirrhosis, causing portal hypertension)
- Divides into right and left portal vein branches at the porta hepatis
Hepatic Artery (~20% of hepatic blood flow)
- The common hepatic artery arises from the coeliac trunk, then gives off the gastroduodenal artery before continuing as the proper hepatic artery
- The proper hepatic artery divides into right and left hepatic arteries
- Significant anatomical variations are common:
- A replaced right hepatic artery (from the superior mesenteric artery) occurs in ~20% of individuals
- A replaced left hepatic artery (from the left gastric artery) is also common
- Surgeons must identify and preserve these variants during cholecystectomy or hepatic resection
Hepatic Veins (venous outflow)
- Three main hepatic veins: right, middle, and left
- They drain directly into the inferior vena cava (IVC) just below the diaphragm
- The caudate lobe (segment I) drains independently via small venous tributaries directly into the IVC - this is clinically relevant in Budd-Chiari syndrome, where it can be spared from congestion
7. Porta Hepatis
The porta hepatis ("gate of the liver") is the transverse fissure on the inferior surface of the liver where structures enter and exit. It contains (enclosed in the hepatoduodenal ligament):
- Common hepatic duct - anteriorly and to the right
- Proper hepatic artery - anteriorly and to the left
- Portal vein - posteriorly
This arrangement is an important surgical landmark (remember it as: duct - artery - vein, from right to left and front to back).
8. Biliary Drainage
- Bile is produced in bile canaliculi between adjacent hepatocytes and flows toward the portal triad (opposite direction to blood flow)
- Canaliculi drain into bile ductules (canals of Hering), then into interlobular bile ducts at the portal triads
- These drain into the right and left hepatic ducts, which merge at the hepatic duct confluence to form the common hepatic duct
- The common hepatic duct joins the cystic duct (from the gallbladder) to form the common bile duct
- Biliary anatomy has considerable variation: in 30-40% of individuals, there is a non-standard hepatic duct confluence (trifurcation, aberrant ducts draining into the left hepatic duct, etc.) - these variants are a major source of bile duct injury during cholecystectomy
9. Lymphatic Drainage
- The liver produces approximately 50% of total body lymph
- Lymph drains to hepatic lymph nodes in the porta hepatis, then to coeliac lymph nodes, and ultimately to the cisterna chyli and thoracic duct
- Deep lymphatics follow the hepatic veins to superior diaphragmatic nodes
10. Innervation
- Parasympathetic: left vagus nerve (anterior hepatic branch) and right vagus (posterior hepatic branch)
- Sympathetic: greater thoracic splanchnic nerves via the coeliac ganglia
- Notably, the denervated liver after transplantation functions normally, indicating these nerves are not essential for metabolic function
- The right phrenic nerve provides sensory supply to the liver capsule, explaining why hepatic disease can cause referred pain to the right shoulder/scapula
11. Microanatomy - The Hepatic Lobule
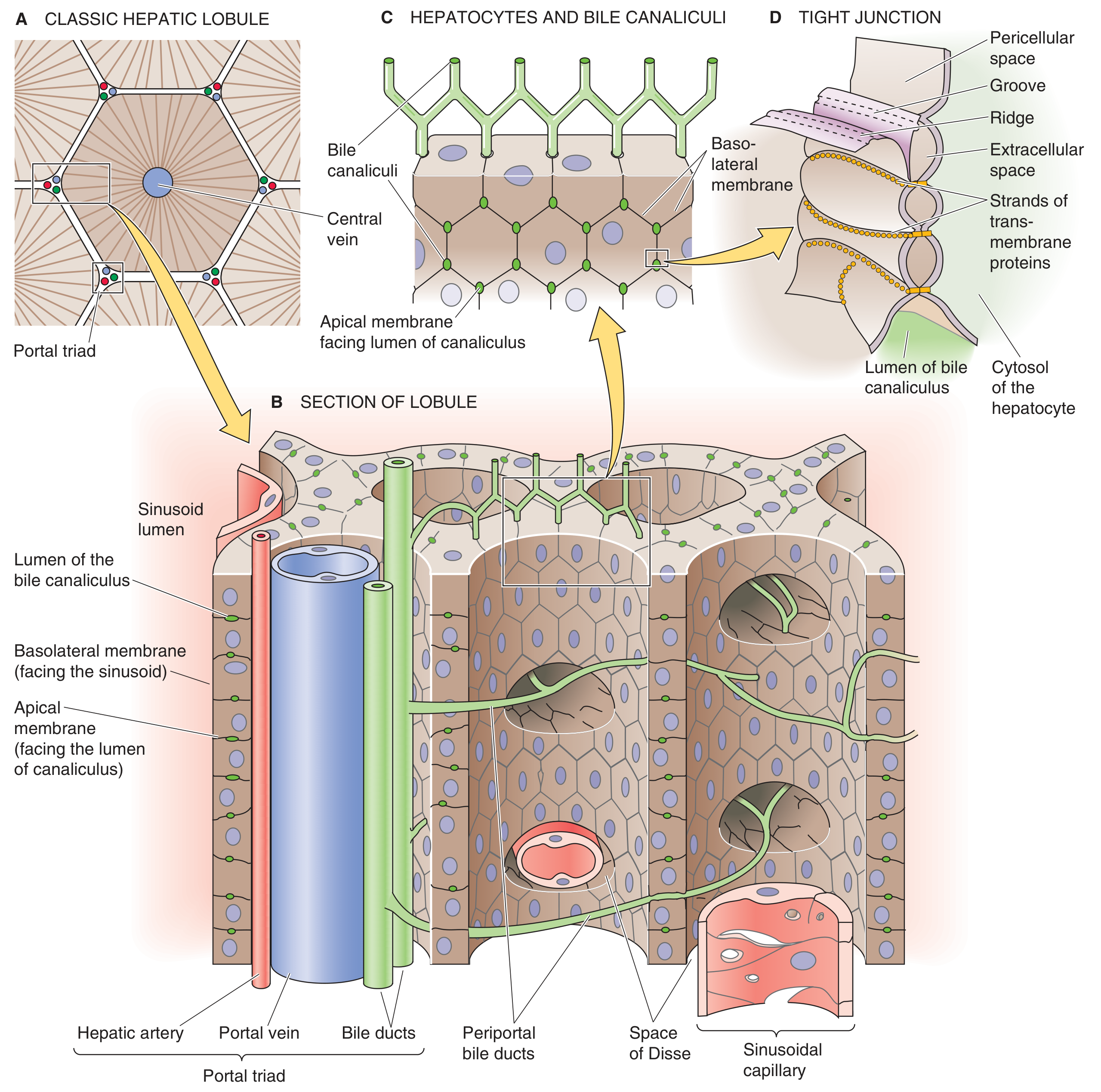
Hepatocytes, sinusoids, and intrahepatic bile system - from Medical Physiology (Boron & Boulpaep)
The functional unit of the liver is the hepatic lobule (50,000-100,000 per liver). Each lobule is a cylindrical structure organized around a central vein, with hepatic plates radiating outward like spokes:
- Portal triad - at the periphery of each lobule; contains a branch of the hepatic artery, portal vein, and bile duct
- Sinusoids - specialized capillaries between hepatocyte plates; blood flows from the portal triad inward toward the central vein; lined by fenestrated endothelium and Kupffer cells (resident macrophages)
- Space of Disse - the perisinusoidal space between the endothelium and hepatocyte basolateral membrane; allows free exchange of solutes and proteins; connects to lymphatics
- Bile canaliculi - tiny (~1 μm diameter) channels formed by the apical membranes of adjacent hepatocytes; bile flows in the opposite direction to blood (centrifugally, toward the portal triads)
- Hepatocytes account for ~80% of liver volume; they are polarized cells with a basolateral membrane facing the sinusoid (for uptake/secretion into blood) and an apical membrane forming the canaliculus (for bile secretion)
- Kupffer cells line the sinusoids and phagocytose bacteria, debris, and foreign matter from portal blood
Functional zones (acinar model):
- Zone 1 (periportal) - receives blood richest in oxygen and nutrients; most resistant to ischemia; most susceptible to toxins absorbed from the gut
- Zone 2 (midzonal)
- Zone 3 (centrilobular/perivenular) - receives blood lowest in oxygen; most susceptible to ischemic necrosis and alcohol-related damage
Summary Table
| Feature | Detail |
|---|---|
| Weight | ~1,500 g |
| Location | Right upper quadrant, beneath right hemidiaphragm |
| Capsule | Glisson's capsule |
| Lobes (morphological) | Right, Left, Caudate, Quadrate |
| Functional division | Cantlie's line (gallbladder fossa to IVC) |
| Couinaud segments | 8 (I = caudate; II-III = left lateral; IV = left medial; V-VIII = right) |
| Arterial supply | Proper hepatic artery (from coeliac trunk) |
| Venous inflow | Portal vein (80%) + hepatic artery (20%) |
| Venous drainage | Right, middle, left hepatic veins → IVC |
| Bile flow direction | Centrifugal (opposite to blood flow) |
| Functional unit | Hepatic lobule (50,000-100,000 per liver) |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., Schwartz's Principles of Surgery 11th Ed., Gray's Anatomy for Students, Guyton and Hall Textbook of Medical Physiology, Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.