lets study brain tumor
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
glioblastoma MRI brain tumor pathology histology
Searching PubMed
"brain tumor" classification management
That's your complete USMLE-level brain tumor guide. Here's what's covered:
10 sections covering the full picture:
- Epidemiology — what's most common and when
- WHO 2021 Classification — the molecular-based system you must know
- Hereditary syndromes — NF1/2, TSC, VHL, Li-Fraumeni, etc.
- Clinical presentation — by general features and location
- Individual tumor profiles — GBM, oligodendroglioma, meningioma, schwannoma, medulloblastoma, craniopharyngioma, PCNSL, and brain mets
- Diagnosis — imaging patterns, MRI features, CSF
- Management — acute (dexamethasone, seizure control) + definitive (surgery/RT/chemo)
- USMLE mnemonics — one-liner pattern recognition table
- Peds vs. adult location rule
- 2024–2025 updates — WHO 2021, TTFields, new RT guidelines
Let me know if you want to go deeper on any specific tumor type, do practice questions, or cover a related topic (e.g., spinal cord tumors, pituitary adenomas, or paraneoplastic syndromes).
lets study neurocysticeercosis from nelson pediatrics mainly lets make it crisp conscise yet conceptual for mbbs level
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
neurocysticercosis MRI CT brain cyst scolex calcification
Excellent — rich content loaded. Now synthesizing the crisp, conceptual MBBS-level guide.
🪱 Neurocysticercosis (NCC) — Crisp MBBS Study Notes
Note: Nelson's Textbook of Pediatrics is not in the library, but the content below is compiled from equivalent authoritative pediatric-infectious-disease sources (Red Book principles, Bradley & Daroff, Grainger & Allison diagnostic radiology, Tintinalli, IDSA 2018 guidelines) — all directly relevant to MBBS/pediatric level.
1. THE CONCEPT IN ONE LINE
NCC = CNS infection by larval stage (cysticercus) of the pork tapeworm Taenia solium → most common parasitic cause of epilepsy worldwide.
2. LIFECYCLE — THE KEY TO UNDERSTANDING EVERYTHING
PORK TAPEWORM (Taenia solium)
↓
TWO ways to get infected:
① TAENIASIS (intestinal worm):
Eat undercooked PORK with larvae (cysticerci)
→ Adult worm lives in human gut → eggs passed in feces
→ Person is a DEFINITIVE HOST
② CYSTICERCOSIS / NCC:
Ingest T. solium EGGS (feco-oral route / contaminated food/water)
→ Eggs hatch → oncospheres → penetrate gut wall
→ Hematogenous spread to BRAIN, muscle, eye, skin
→ Form CYSTICERCI (larvae with scolex)
→ Person is an INTERMEDIATE HOST
Key concept: You get NCC from eggs (not from eating pork). You can get it from a tapeworm carrier in your household even if you're vegetarian!
3. EPIDEMIOLOGY
| Feature | Detail |
|---|---|
| Distribution | Latin America, India, Sub-Saharan Africa, SE Asia |
| Most common cause of | Secondary (provoked) epilepsy in developing world |
| Estimated global burden | ~1 million epilepsy cases due to NCC |
| Risk factor | Poor sanitation, open defecation, eating with tapeworm carriers |
| In children | Same mechanism; may present with encephalitic form (diffuse cysts + edema) |
4. PATHOLOGY — 4 STAGES OF THE CYST
This is the most important concept. Symptoms depend on which stage the cyst is in.
| Stage | What's Happening | Imaging | Symptoms |
|---|---|---|---|
| 1. Vesicular | Viable larva, host tolerates it | Thin-walled cyst, CSF-like fluid, scolex dot ("hole with dot") — NO edema, NO enhancement | Often asymptomatic |
| 2. Colloidal Vesicular | Larva begins dying → immune reaction | Ring-enhancing cyst + perilesional edema | Seizures, headache, ↑ ICP |
| 3. Granular Nodular | Larva dead, cyst collapses | Thick enhancing wall, more edema | Seizures, focal deficits |
| 4. Calcified Nodular | End-stage scar | Calcified nodule on CT, no enhancement | May trigger seizures even years later |
USMLE/MBBS pearl: Most seizures occur at stages 2 & 3 — when the dying larva triggers the inflammatory cascade. 80–90% of single lesions resolve in 3–6 months.
5. FORMS OF NCC
| Form | Location | Notes |
|---|---|---|
| Parenchymal (most common) | Brain parenchyma | Seizures, headache |
| Intraventricular | 4th ventricle most common | Obstructive hydrocephalus |
| Subarachnoid / Racemose | Basal cisterns | Meningitis-like, chronic hydrocephalus, worst prognosis |
| Cysticercotic Encephalitis | Diffuse | Multiple cysts + massive cerebral edema; seen in children & young women; AVOID antiparasitics acutely |
| Spinal | Spinal cord | Radiculopathy, myelopathy |
| Ocular | Vitreous, subretinal | Visual loss — surgical emergency |
6. CLINICAL FEATURES
Seizures — #1 presentation (50–70%); typically new-onset focal seizures in someone from endemic area
- Usually simple partial (focal) with secondary generalization
- Occur as cyst degenerates (stages 2–3)
Headache — raised ICP (especially intraventricular/subarachnoid form)
Hydrocephalus — cyst obstructs CSF flow at 4th ventricle or aqueduct
Focal neurological deficits — hemiplegia, visual changes depending on location
Chronic meningitis — basal/subarachnoid form
Encephalitic form (children) — diffuse cysts → massive edema → RICP, coma; corticosteroids are critical, antiparasitics contraindicated acutely
7. DIAGNOSIS
Imaging (cornerstone)
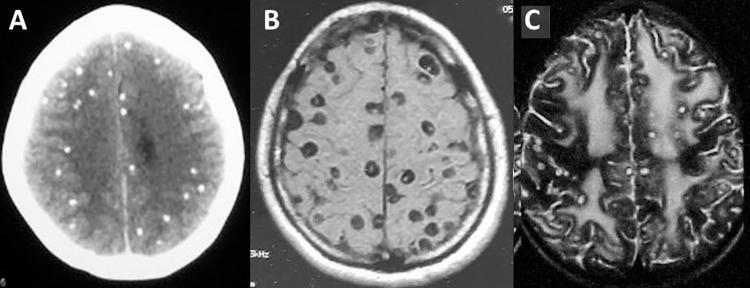
CT scan (non-contrast):
- Calcified lesions (end-stage) — hyperdense dots
- Cystic hypodense lesions ± scolex
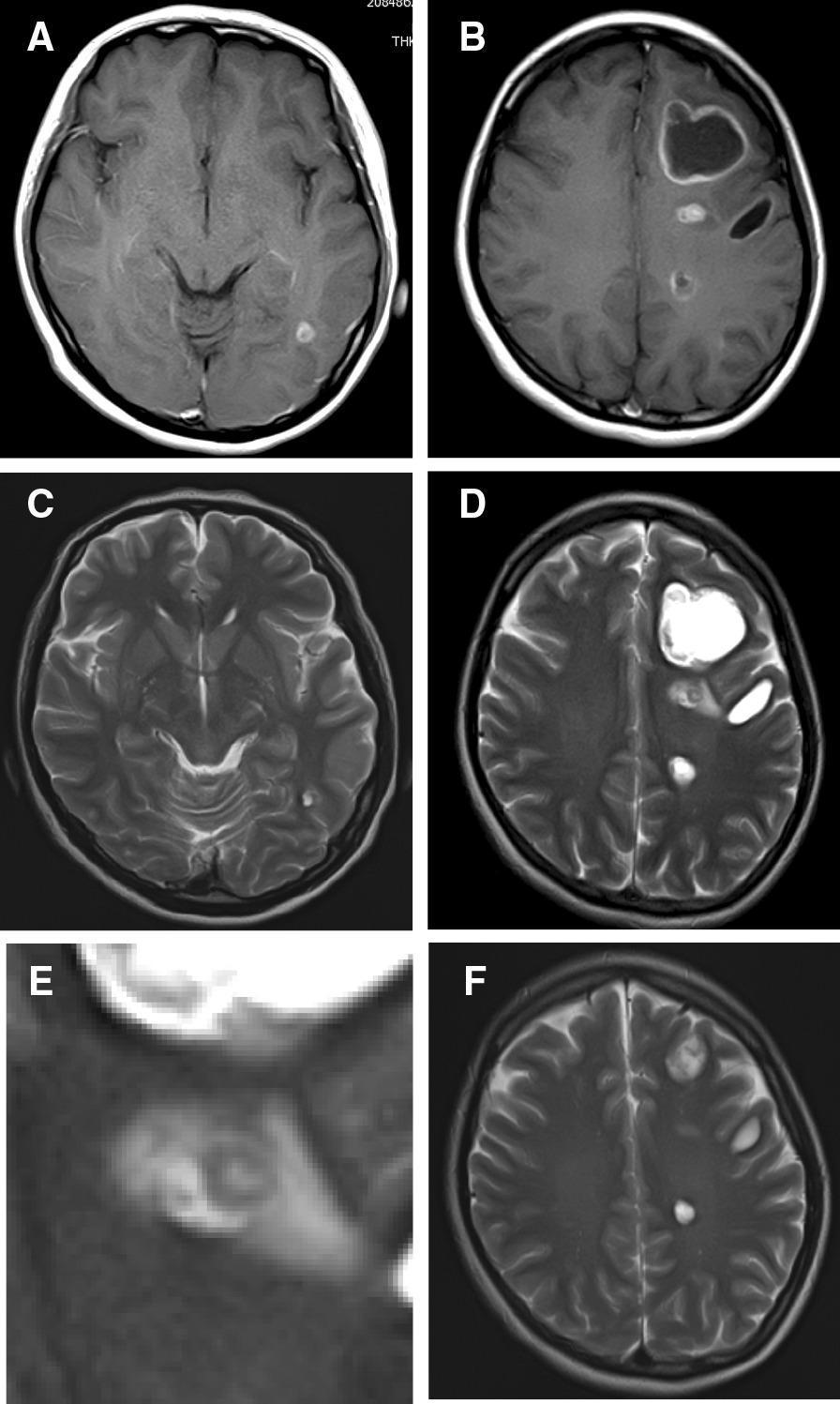
MRI (superior for active lesions):
- "Hole with dot" sign = cyst + scolex = pathognomonic
- Ring-enhancing lesions with perilesional edema in colloidal stage
- FLAIR: scolex appears hyperintense
- Identifies all 4 stages clearly

Serology
- EITB (Enzyme-Linked Immunoelectrotransfer Blot) on serum — most specific (~99%)
- Less sensitive with single/calcified cysts
- CSF ELISA also used
CSF
- May show eosinophilia, elevated protein, low glucose (basal form)
- Rarely needed; lumbar puncture contraindicated if ↑ ICP
Del Brutto Diagnostic Criteria (2017 IDSA/ASTMH)
- Absolute criterion: Histopathology OR cyst with scolex on imaging
- Major criteria: Imaging lesions compatible with NCC + positive serology
- Minor criteria: Hydrocephalus, enhancement, clinical features, exposure history
8. TREATMENT
Framework: Match treatment to stage + form + number
| Situation | Treatment |
|---|---|
| Single enhancing lesion (most common in India/children) | Albendazole × 1–2 weeks + steroids; AEDs for seizure control |
| 1–2 viable parenchymal cysts | Albendazole monotherapy + steroids |
| >2 viable parenchymal cysts | Albendazole + Praziquantel (combination) + steroids |
| Calcified cysts only | No antiparasitic (dead larvae); AEDs if seizures persist |
| Cysticercotic encephalitis | Steroids only — NO antiparasitics (will worsen edema) |
| Intraventricular cyst | Neuroendoscopic removal (3rd/lateral ventricle); surgery/shunt (4th ventricle) |
| Subarachnoid/Racemose | Prolonged albendazole ± praziquantel + steroids + shunt if hydrocephalus |
| Ocular cysticercosis | Surgical removal (antiparasitics worsen inflammation) |
Drug Details
| Drug | Dose | Mechanism |
|---|---|---|
| Albendazole | 15 mg/kg/day ÷ 2 doses × 8–28 days | Better CNS penetration; preferred |
| Praziquantel | 50–100 mg/kg/day ÷ 3 doses | Disrupts tegument; less penetration than albendazole |
| Dexamethasone / Prednisolone | Always with antiparasitics | Reduces inflammatory edema from dying larvae |
| AEDs (levetiracetam, carbamazepine) | For seizure control | Not indefinite unless seizures persist |
Why steroids with antiparasitics? Killing the larvae triggers a surge of host inflammation → can cause cerebral edema, increased ICP, paradoxical worsening. Steroids blunt this.
Albendazole > Praziquantel because praziquantel levels are reduced by dexamethasone and by coadministration with antiepileptics (enzyme induction).
9. SINGLE ENHANCING LESION (SEL) — High-yield for India/Pediatrics
- Most common presentation in India and pediatric patients
- 1–2 cm ring-enhancing or disc-enhancing lesion on CT/MRI
- Differential: NCC vs. tuberculoma (both common in India!)
- NCC favored if: scolex visible, no basal meningeal enhancement, EITB positive
- Tuberculoma favored if: satellite lesions, basal enhancement, contact with TB
- SEL resolves in 80–90% within 3–6 months with albendazole + steroids
10. COMPLICATIONS
| Complication | Mechanism |
|---|---|
| Epilepsy (most common) | Perilesional gliosis + calcification → seizure focus |
| Obstructive hydrocephalus | Intraventricular cyst blocking CSF flow |
| Communicating hydrocephalus | Basal arachnoiditis → impaired CSF reabsorption |
| Stroke | Vasculitis from basal NCC → lacunar infarcts |
| Cysticercotic encephalitis | Massive immune response to dying larvae |
| Cognitive decline | Chronic multiple lesion disease |
11. PREVENTION
- Proper cooking of pork (>65°C destroys cysticerci)
- Handwashing and good hygiene (breaks feco-oral transmission of eggs)
- Sanitation — toilet access, no open defecation
- Mass drug administration: albendazole/praziquantel in endemic areas (experimental)
- Porcine vaccination: Ox-fax vaccine against T. solium in pigs
12. MEMORY HOOKS
| Hook | Fact |
|---|---|
| "Hole with dot" | Cyst + scolex on imaging = pathognomonic |
| Vegetarian can get NCC | From eggs, not pork |
| Seizures when larva dies, not when alive | Immune response at colloidal/granular stage |
| Steroids alone in encephalitic form | Antiparasitics worsen edema |
| Albendazole > Praziquantel | Better CNS penetration + not antagonized by steroids |
| Calcified = no antiparasitics | Dead parasite; treat seizures symptomatically |
| Ocular & intraventricular = surgery | Antiparasitics dangerous in eye; endoscopy for ventricles |
| India = SEL + TB differential | Must distinguish NCC from tuberculoma |
Sources: Bradley & Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology; Tintinalli's Emergency Medicine; Washington Manual of Medical Therapeutics; IDSA/ASTMH 2018 Clinical Practice Guidelines for NCC
Let me know if you want to go deeper on any section — lifecycle diagram, differential of ring-enhancing lesions, pediatric encephalitic form, or practice MCQs on NCC!
This is a shared conversation. Sign in to Orris to start your own chat.