Immunomodulators
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have all the content I need for a thorough exam-focused summary. Let me compile the comprehensive response.
Immunomodulators - Comprehensive Exam Review
The 3-Signal Model of Immune Activation
Understanding the three-signal model is fundamental - all immunosuppressant drug classes target one or more of these signals.
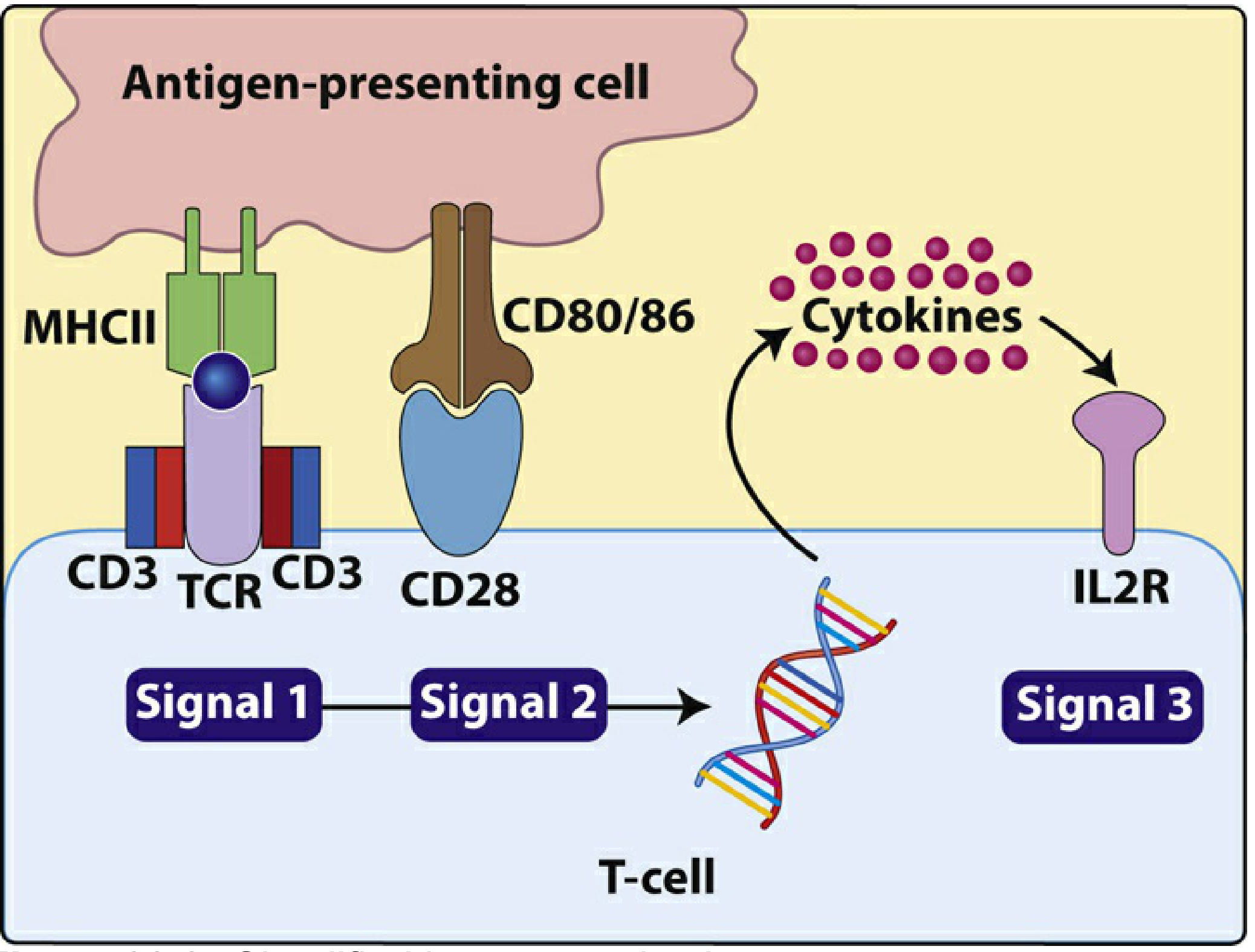
| Signal | What Happens | Target Receptor | Drugs That Block It |
|---|---|---|---|
| Signal 1 | Antigen (on APC via MHC II) binds T-cell receptor (TCR/CD3 complex) | CD3/TCR | Anti-thymocyte globulins, alemtuzumab |
| Signal 2 | CD80/86 on APC binds CD28 on T cell (costimulation) | CD28/CD80/86 | Belatacept (CTLA-4 fusion protein) |
| Signal 3 | IL-2 binds IL-2R (CD25) → mTOR activation → T-cell proliferation | IL-2R / mTOR | mTOR inhibitors (sirolimus, everolimus); IL-2R antibodies (basiliximab) |
The calcium-calcineurin pathway is activated by Signals 1+2 and drives IL-2 production - this is where calcineurin inhibitors act.
Class 1 - Calcineurin Inhibitors (CNIs)
Mechanism: Block calcineurin → prevent dephosphorylation of NFAT → no IL-2 gene transcription → no T-cell activation.
| Drug | Key Points |
|---|---|
| Cyclosporine (NEORAL, SANDIMMUNE) | Binds cyclophilin → complex inhibits calcineurin. SE: nephrotoxicity, hypertension, hirsutism, gingival hyperplasia, hyperlipidemia, tremor, neurotoxicity. Metabolized by CYP3A4/P-gp - many drug interactions. Uses: transplant rejection prophylaxis, psoriasis, rheumatoid arthritis, dry eye disease |
| Tacrolimus (PROGRAF) | Binds FKBP-12 → complex inhibits calcineurin. SE: nephrotoxicity, neurotoxicity, GI complaints, hypertension, glucose intolerance/diabetes. Metabolized by CYP3A. More potent than cyclosporine. Uses: transplant rejection prophylaxis |
| Pimecrolimus / Tacrolimus (topical) | Topical calcineurin inhibitors for atopic dermatitis. Inhibit T-lymphocyte activation and prevent cytokine release. FDA black box warning re: long-term risk of malignancy (animal data). Tacrolimus 0.03% approved for children >2 years |
Key exam point: Both CNIs have a narrow therapeutic index - therapeutic drug monitoring (TDM) is mandatory. CYP3A4 inhibitors (azole antifungals, macrolides, grapefruit) increase levels; CYP3A4 inducers (rifampin, phenytoin) decrease levels.
Class 2 - mTOR Inhibitors
Mechanism: Bind FKBP-12 → complex inhibits mTOR → blocks IL-2-driven cell cycle progression (G1 → S phase) → prevents T-cell proliferation (Signal 3 blockade).
| Drug | Key Uses | Key Side Effects |
|---|---|---|
| Sirolimus (rapamycin, RAPAMUNE) | Transplant rejection prophylaxis, GVHD prevention/treatment, sirolimus-coated coronary stents (prevent restenosis) | Hyperlipidemia, thrombocytopenia, poor wound healing, pulmonary toxicity, mouth ulcers |
| Everolimus (ZORTRESS) | Transplant rejection prophylaxis, oncology (various cancers) | Similar to sirolimus |
Key exam point: mTOR inhibitors are used in combination with CNIs to reduce CNI doses (and CNI nephrotoxicity). They also require TDM due to narrow therapeutic index.
Class 3 - Antiproliferatives (Antimetabolites)
These block lymphocyte proliferation by inhibiting nucleic acid synthesis.
| Drug | Mechanism | Key Points |
|---|---|---|
| Azathioprine (IMURAN) | Prodrug → 6-mercaptopurine (6-MP) → thioinosinic acid → incorporated into DNA → blocks chain elongation | Dose-limiting SE: bone marrow suppression (leukopenia). Xanthine oxidase metabolizes 6-MP - avoid with allopurinol (reduce dose 75%) and contraindicated with febuxostat. |
| Mycophenolate mofetil (CELLCEPT) | Prodrug → mycophenolic acid (MPA) → reversible non-competitive inhibitor of inosine monophosphate dehydrogenase (IMPDH) → blocks de novo guanosine synthesis → selectively blocks T- and B-cell proliferation (lymphocytes lack salvage pathway) | Has largely replaced azathioprine. SE: GI distress (nausea, vomiting, diarrhea), bone marrow suppression (anemia, leukopenia, thrombocytopenia), increased infections. Enterohepatic recirculation prolongs effect. |
| Mycophenolate sodium (MYFORTIC) | Active form (MPA); enteric-coated to reduce GI side effects | Equivalent efficacy to MMF |
| Methotrexate | Inhibits dihydrofolate reductase → blocks purine and pyrimidine synthesis. Also anti-inflammatory (adenosine release) | Used in RA, psoriasis, IBD, prevention of GVHD. SE: hepatotoxicity, pulmonary fibrosis, mucositis, bone marrow suppression. Requires folate supplementation. |
Class 4 - Costimulation Blocker
| Drug | Mechanism | Key Points |
|---|---|---|
| Belatacept (NULOJIX) | CTLA-4-Ig fusion protein - binds CD80/CD86 on APCs → prevents CD28 engagement → blocks Signal 2 | IV infusion only. Approved for kidney transplantation (with basiliximab + MMF + corticosteroids). Avoids CNI nephrotoxicity. Contraindicated in EBV-seronegative patients (risk of post-transplant lymphoproliferative disorder, PTLD - especially CNS). |
Class 5 - Antibodies (Biologics)
Polyclonal Antibodies (Induction / Anti-rejection)
| Drug | Target | Use |
|---|---|---|
| Anti-thymocyte globulin (equine) - ATGAM | T lymphocytes | Induction, treatment of acute rejection |
| Anti-thymocyte globulin (rabbit) - THYMOGLOBULIN | T lymphocytes | More potent than equine; preferred in high-risk patients |
Monoclonal Antibodies
| Drug | Target | Type | Key Use | Key Side Effects |
|---|---|---|---|---|
| Basiliximab (SIMULECT) | IL-2R (CD25) - blocks Signal 3 | Chimeric (mouse/human) | Induction in renal transplantation | Well tolerated |
| Rituximab (RITUXAN) | CD20 on B cells | Chimeric | B-cell lymphomas, RA, GVHD, antibody-mediated rejection | Infusion reactions, progressive multifocal leukoencephalopathy (PML), hepatitis B reactivation |
| Alemtuzumab (CAMPATH) | CD52 on T and B cells | Humanized | Induction, CLL, MS | Profound lymphodepletion, infusion reactions, autoimmune cytopenias |
| Belimumab (BENLYSTA) | BLyS (B-lymphocyte stimulator) | Fully human | Systemic lupus erythematosus (SLE) | Infection, depression, infusion reactions |
TNF Inhibitors (used in autoimmune diseases)
| Drug | Type | Key Uses | Key Risks |
|---|---|---|---|
| Etanercept (ENBREL) | Soluble TNF receptor fusion protein | RA, psoriasis, psoriatic arthritis, ankylosing spondylitis | Infection, TB reactivation |
| Infliximab (REMICADE) | Chimeric IgG1 anti-TNF antibody | RA, IBD (Crohn's, UC), psoriasis, AS | TB reactivation (screen before use), hepatotoxicity |
| Adalimumab (HUMIRA) | Fully human anti-TNF antibody | RA, IBD, psoriasis, AS, uveitis | Infection, TB reactivation |
Key exam point on TNF inhibitors: Screen all patients for latent TB (TB test + CXR) before initiating. Contraindicated in active TB, serious infections, and Class III-IV heart failure. Risk of demyelinating disease, lymphoma.
IL Blockers
| Drug | Target | Key Use |
|---|---|---|
| Tocilizumab (ACTEMRA) | IL-6 receptor | RA, giant cell arteritis, cytokine release syndrome (CRS) |
| Secukinumab (COSENTYX) | IL-17A | Psoriasis, ankylosing spondylitis, psoriatic arthritis |
| Ustekinumab (STELARA) | IL-12 and IL-23 (p40 subunit) | Psoriasis, psoriatic arthritis, Crohn's disease |
| Dupilumab (DUPIXENT) | IL-4 receptor alpha (blocks IL-4 and IL-13) | Atopic dermatitis, asthma, eosinophilic esophagitis |
| Mepolizumab (NUCALA) | IL-5 | Eosinophilic asthma |
| Canakinumab | IL-1β | Periodic fever syndromes, gout flares |
Class 6 - JAK Inhibitors (Small Molecule Targeted Therapy)
Mechanism: Inhibit Janus kinases (JAK1, JAK2, JAK3, TYK2) → block cytokine-driven STAT phosphorylation → reduce immune cell proliferation and cytokine production.
| Drug | Selectivity | Key Uses | Key Adverse Effects |
|---|---|---|---|
| Tofacitinib (XELJANZ) | JAK1/JAK3 | RA, psoriatic arthritis, ulcerative colitis | Infections, herpes zoster reactivation, thrombosis, ↑ malignancy risk (black box warning); CYP2C19/CYP3A4 interactions |
| Baricitinib (OLUMIANT) | JAK1/JAK2 | RA, COVID-19 (severe) | Similar to tofacitinib + thromboembolism risk |
| Upadacitinib (RINVOQ) | JAK1 selective | RA, atopic dermatitis | Similar |
Class 7 - Corticosteroids (as Immunosuppressants)
Mechanism: Bind glucocorticoid receptor → translocates to nucleus → suppresses NF-κB → ↓ transcription of proinflammatory cytokines (IL-1, IL-6, TNF-α) → broad effects on cellular immunity.
- Uses: transplant rejection, autoimmune diseases, GVHD, asthma, IBD, SLE, RA, MS relapses
- SE: hyperglycemia, hypertension, Cushingoid habitus, weight gain, osteoporosis, glaucoma, cataracts, adrenal suppression (with long-term use - must taper slowly)
- Prednisone is a prodrug converted to prednisolone in the liver (inactive in severe hepatic disease)
Class 8 - Topical Immunomodulators (Dermatology)
| Drug | Mechanism | Use |
|---|---|---|
| Imiquimod (ALDARA 5%, ZYCLARA 3.75%) | TLR-7/8 agonist → stimulates mononuclear cells to release IFN-α, IL-1, IL-6, IL-8, TNF-α | Genital warts, actinic keratoses, superficial basal cell carcinoma |
| Crisaborole (EUCRISA) | PDE-4 inhibitor (non-steroidal) | Mild-moderate atopic dermatitis ≥2 years |
| Apremilast (OTEZLA) | PDE-4 inhibitor (oral) | Psoriasis, psoriatic arthritis, oral ulcers in Behcet's |
Summary: Drug Classification by Mechanism
SIGNAL 1 BLOCKERS: Anti-thymocyte globulins, alemtuzumab
SIGNAL 2 BLOCKERS: Belatacept (CTLA-4 fusion protein)
CALCINEURIN INH: Cyclosporine, Tacrolimus → block IL-2 production
IL-2R BLOCKERS: Basiliximab (Signal 3)
mTOR INHIBITORS: Sirolimus, Everolimus → block IL-2 driven proliferation
ANTIMETABOLITES: Azathioprine (purine analog), Mycophenolate (IMPDH inhibitor)
CORTICOSTEROIDS: Broad cytokine suppression (NF-κB inhibition)
B-CELL DEPLETION: Rituximab (anti-CD20)
TNF INHIBITORS: Etanercept, Infliximab, Adalimumab
IL BLOCKERS: Tocilizumab (IL-6R), Dupilumab (IL-4Ra), Secukinumab (IL-17A)
JAK INHIBITORS: Tofacitinib, Baricitinib, Upadacitinib
High-Yield Exam Associations
| Association | Answer |
|---|---|
| Nephrotoxicity + hirsutism + gingival hyperplasia | Cyclosporine |
| Nephrotoxicity + diabetes mellitus + neurotoxicity | Tacrolimus |
| Blocks de novo guanosine synthesis (IMPDH) | Mycophenolate |
| Prodrug → 6-MP → inhibits DNA chain elongation | Azathioprine |
| Contraindicated with allopurinol (or reduce dose) | Azathioprine |
| Contraindicated in EBV-seronegative transplant patients | Belatacept |
| Blocks CD80/86 (costimulation signal 2) | Belatacept |
| Used in SLE (blocks BLyS) | Belimumab |
| Screen for latent TB before use | All TNF inhibitors |
| Sirolimus-eluting stent purpose | Prevents restenosis (inhibits endothelial proliferation) |
| TDM required (narrow therapeutic index) | CNIs + mTOR inhibitors |
| Fully human monoclonal antibody (ends in -umab) | Adalimumab, belimumab |
| Chimeric antibody (ends in -ximab) | Rituximab, infliximab, basiliximab |
Sources: Lippincott Illustrated Reviews: Pharmacology, Ch. 38; Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology, 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.