Different Transport modes esp. active (NA+ K+ ATPase pump) & facilitated diffusion,Edema ) • Homeostasis • Nerve & Muscle • action potential , refractory period ,all or none law , SALTATORY CONDUCTION , WALLERIAN DEGENERATION , strength duration curve , • Steps of Transmission across NM JUNCTION (Important) along with applied Myasthenia gravis • Excitation contraction coupling (Important) including Sarcoplasmic reticular system (Important) + Molecula
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, structured physiology notes covering all the topics you listed, drawn directly from Guyton & Hall, Costanzo Physiology, Medical Physiology, and Goodman & Gilman's.
PHYSIOLOGY MASTER NOTES
PART 1: MEMBRANE TRANSPORT MODES
A. Types of Transport (Overview)
| Type | Energy | Direction | Examples |
|---|---|---|---|
| Simple diffusion | None | Down gradient | O2, CO2, lipid-soluble drugs |
| Facilitated diffusion | None (carrier/channel) | Down gradient | Glucose (GLUT), water (AQP) |
| Primary active transport | ATP directly | Against gradient | Na-K ATPase, Ca-ATPase |
| Secondary active transport | Ion gradient (indirect) | Against gradient | SGLT (glucose-Na cotransport) |
B. Na⁺-K⁺ ATPase Pump (Primary Active Transport)
This is the most important active transporter in the body.
Structure: A membrane-bound pump with 2 subunits (alpha + beta). The alpha subunit has the catalytic + transport function.
Mechanism (electrogenic):
- 3 Na⁺ bind to intracellular sites on the pump
- ATP is hydrolyzed → pump becomes phosphorylated (conformational change)
- 3 Na⁺ are expelled to the extracellular space
- 2 K⁺ bind from extracellular side
- Dephosphorylation → pump returns to original conformation
- 2 K⁺ enter the cell
- Net result: 3 Na⁺ out, 2 K⁺ in per cycle - electrogenic (generates a net outward positive current)
Functions:
- Maintains resting membrane potential (cell interior negative)
- Prevents cell swelling (by controlling intracellular osmolality)
- Powers secondary active transport (provides Na gradient used by SGLT, NHE, etc.)
- Maintains excitability of nerve and muscle cells
Inhibited by: Ouabain, cardiac glycosides (digoxin) - these bind the extracellular K⁺ site
Source: Guyton and Hall Textbook of Medical Physiology, Comprehensive Clinical Nephrology 7e
C. Facilitated Diffusion
- Movement down the electrochemical gradient using a carrier protein or channel - no energy required
- Shows saturation kinetics (Vmax) and specificity
- Examples:
- GLUT-1 to GLUT-5 - glucose entry into cells (GLUT-4 is insulin-dependent in muscle/fat)
- Aquaporins (AQP) - water channels
- Ion channels (Na⁺, K⁺, Ca²⁺, Cl⁻ channels)
Differences from simple diffusion:
- Carrier-mediated (shows saturation, competitive inhibition)
- Faster rates at low concentrations
- Can be regulated (e.g., GLUT-4 insertion stimulated by insulin)
D. Edema - Pathophysiology
Edema = excess fluid in interstitial compartment. Governed by Starling forces:
Net filtration = Kf [ (Pc - Pi) - σ(πc - πi) ]
Where: Pc = capillary hydrostatic pressure, Pi = interstitial hydrostatic pressure, πc = capillary oncotic pressure, πi = interstitial oncotic pressure
Causes of edema:
| Mechanism | Cause | Example |
|---|---|---|
| ↑ capillary hydrostatic pressure | Venous obstruction, heart failure | Pitting edema in CCF |
| ↓ plasma oncotic pressure | Hypoalbuminemia | Nephrotic syndrome, liver failure, kwashiorkor |
| ↑ capillary permeability | Inflammation, burns, anaphylaxis | Angioedema |
| Lymphatic obstruction | Filariasis, post-mastectomy | Lymphedema (non-pitting) |
| Na⁺ retention | ↑ aldosterone | Renal edema |
Key rule: Pitting edema = high protein content (exudate in inflammation) or low protein (transudate in CCF, nephrotic). Lymphedema = non-pitting, protein-rich.
PART 2: HOMEOSTASIS
Homeostasis = the tendency of the body to maintain a stable internal environment despite external changes.
Components of a homeostatic control system:
- Receptor/sensor - detects deviation from set point
- Control center (integrating center) - processes and compares to set point
- Effector - corrects the deviation
Types of feedback:
- Negative feedback - most common; opposes the change (e.g., thermoregulation, blood pressure, blood glucose)
- Positive feedback - amplifies the change (e.g., childbirth oxytocin surge, LH surge at ovulation, blood clotting cascade)
Important set points:
- Core body temp: 37°C
- Blood pH: 7.35-7.45
- Plasma osmolality: 280-295 mOsm/kg
- Blood glucose: 70-100 mg/dL (fasting)
PART 3: NERVE & MUSCLE PHYSIOLOGY
A. Action Potential
The action potential is a rapid reversal of membrane polarity that propagates along a nerve or muscle fiber.
Resting membrane potential: -70 mV (nerve), -90 mV (skeletal muscle), -85 mV (cardiac muscle)
- Maintained by: K⁺ leakage outward, Na-K ATPase pump
Phases of action potential (nerve):
| Phase | Ion involved | Gate status |
|---|---|---|
| Resting | K⁺ dominant | Na⁺ channels closed |
| Depolarization (rising) | Na⁺ rapid influx | Na⁺ activation gates OPEN |
| Overshoot | +30 mV | Peak depolarization |
| Repolarization (falling) | K⁺ efflux + Na⁺ inactivation | Na⁺ inactivation gates close; K⁺ channels open |
| After-hyperpolarization | Excess K⁺ efflux | K⁺ channels slow to close |
| Return to resting | Na-K pump | Gradual restoration |
Threshold: ~-55 mV. If this is not reached, no action potential fires.
B. All-or-None Law
"Once threshold is reached, the action potential fires with maximum amplitude regardless of the strength of the stimulus. Subthreshold stimuli produce no response."
- The size and duration of an action potential are constant for a given neuron
- Stimulus strength is coded not by AP amplitude but by frequency of firing
- The law applies to: nerve fibers, skeletal muscle fibers, cardiac muscle
C. Refractory Period
Absolute Refractory Period (ARP):
- No stimulus, however strong, can produce another AP
- Na⁺ activation gates are open OR Na⁺ inactivation gates are closed (h gates shut)
- Duration: ~1-2 ms in nerve; 200-300 ms in cardiac muscle (protective - prevents tetanus)
Relative Refractory Period (RRP):
- Follows ARP; a stronger-than-normal stimulus CAN fire another AP
- K⁺ channels still open; membrane hyperpolarized
- Corresponds to repolarization/after-hyperpolarization phase
Clinical significance of cardiac ARP: The long ARP in cardiac muscle prevents summation and tetanus, ensuring effective pumping function.
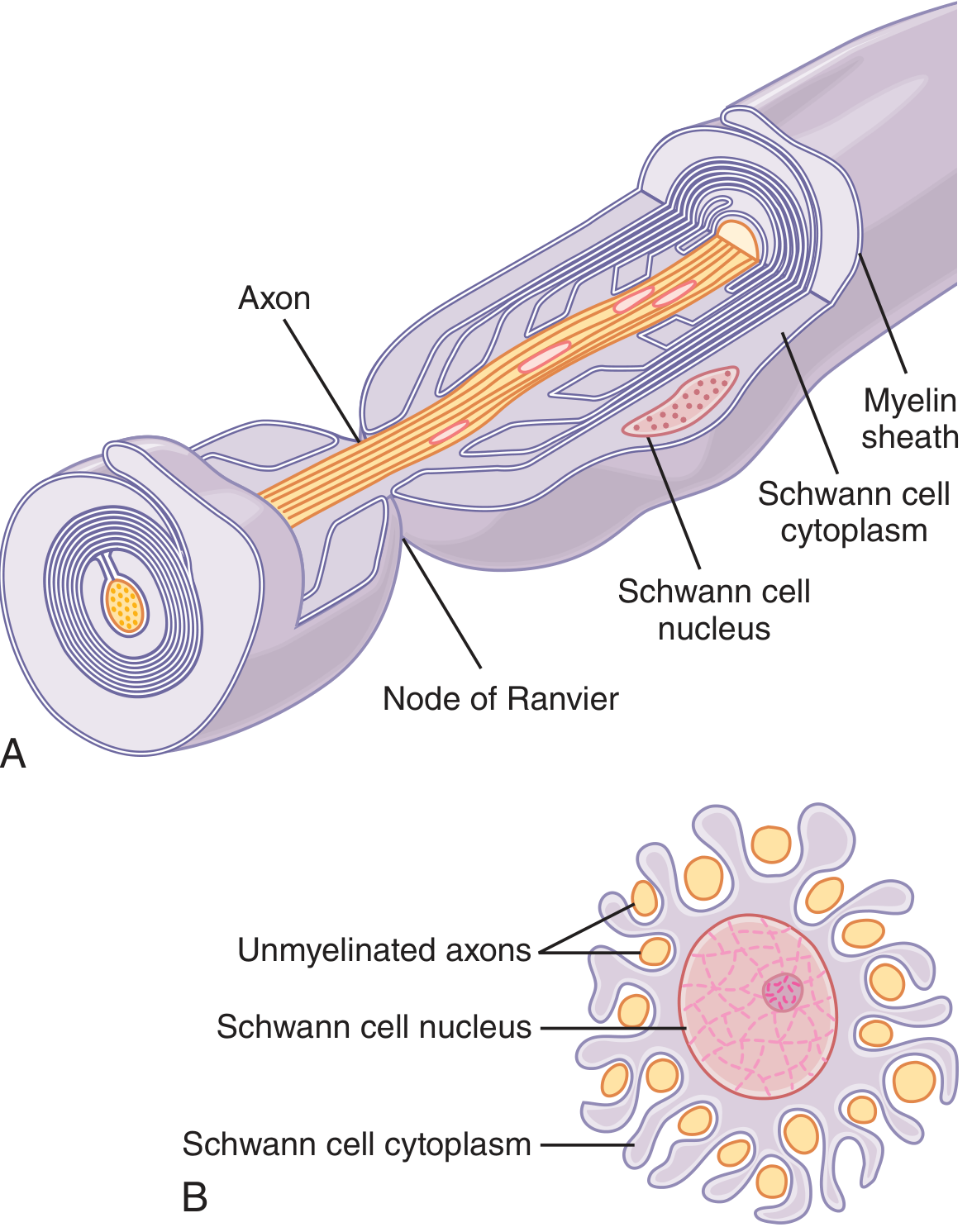
D. Saltatory Conduction
In myelinated fibers, the myelin sheath (deposited by Schwann cells, lipid substance = sphingomyelin) acts as an insulator, reducing ion flow through covered membrane by ~5000-fold.
Nodes of Ranvier = small uninsulated gaps (2-3 µm) between adjacent Schwann cells, occurring every 1-3 mm.
Saltatory conduction mechanism:
- Action potential can only occur at the nodes (where ion channels are concentrated)
- Current flows from one depolarized node to the next resting node through extracellular fluid
- The AP "jumps" from node to node (saltus = jump)
Advantages of saltatory conduction:
- Speed - conduction velocity up to 100-120 m/s (vs. 0.5-2 m/s in unmyelinated fibers)
- Energy efficiency - ion exchange only at nodes, less Na-K pump activity needed
- Protection - if one node is blocked, current can jump 2-3 nodes
Source: Guyton and Hall Textbook of Medical Physiology
E. Wallerian Degeneration
After a peripheral nerve is cut or severely injured (grade II-V), the axon segment distal to the injury degenerates - this is Wallerian degeneration.
Timeline of events:
Distal segment (main events):
- Hours: Disruption of axonal plasma membrane → rapid influx of Ca²⁺ and Na⁺
- This activates proteolytic enzymes (calpains) - cascade resembling apoptosis
- Day 3: Schwann cells retract from nodes of Ranvier
- Days 3-7: Schwann cells and macrophages digest myelin (phagocytosis)
- The entire axonal process takes ~1 week
- Schwann cells proliferate and form Bands of Büngner (guides for regeneration)
Proximal segment (cell body changes = Chromatolysis):
- Nucleus moves eccentrically
- Nissl substance (rough ER) dissolves/disperses
- Cell body swells
- Upregulation of transcription factors: switches from maintenance mode to protein synthesis mode
- Key protein upregulated: c-Jun (in Schwann cells)
Nerve regeneration:
- Axon sprouts grow from proximal stump at ~1-4 mm/day
- Collateral sprouting from intact axons reinnervates denervated muscle
- Remyelination occurs with thinner myelin and shorter internodes
Applied: Nerve conduction studies show loss of compound action potential distal to lesion. EMG shows denervation fibrillations at 2-3 weeks.
Source: Bradley and Daroff's Neurology in Clinical Practice
F. Strength-Duration Curve
This curve relates the minimum stimulus intensity (strength) needed to fire an AP to the duration for which that stimulus is applied.
Key concepts:
- Rheobase: The minimum stimulus strength (intensity/current) that can trigger an AP when applied for an infinite (very long) duration
- Chronaxie: The minimum duration of a stimulus needed to fire an AP when applied at twice the rheobase intensity
- Chronaxie is a measure of tissue excitability
- Short chronaxie = more excitable (e.g., motor nerve: ~0.05 ms)
- Long chronaxie = less excitable (e.g., cardiac muscle: ~2 ms)
Relationship: Strength × Duration = constant (hyperbolic curve)
Clinical use:
- Distinguish nerve vs. muscle excitability (denervated muscle has longer chronaxie)
- Assess nerve injuries (Wallerian degeneration raises chronaxie)
- Design electrical stimulation parameters in physiotherapy
PART 4: NEUROMUSCULAR JUNCTION (NMJ) TRANSMISSION ⭐ IMPORTANT
Anatomy of the Motor End Plate
- Presynaptic terminal: axon terminal filled with ~300,000 ACh vesicles + mitochondria
- Synaptic cleft: 20-30 nm wide, contains acetylcholinesterase (AChE)
- Postsynaptic membrane: muscle membrane with deep subneural clefts (increase surface area) and nicotinic ACh receptors (nAChR) concentrated at the mouths of clefts
Step-by-Step Transmission
Step 1 - Action potential arrives at nerve terminal
- AP travels down the motor neuron to the presynaptic terminal
Step 2 - Ca²⁺ entry into presynaptic terminal
- Depolarization opens voltage-gated P-type (and L-type) Ca²⁺ channels at active zones
- Ca²⁺ flows from extracellular fluid into the nerve terminal
- No Ca²⁺ = no ACh release (critical concept)
- Doubling [Ca²⁺] increases quantal ACh release 16-fold
Step 3 - ACh vesicle mobilization and fusion
- Ca²⁺ activates Ca²⁺-calmodulin-dependent protein kinase
- This phosphorylates synapsin proteins that anchor vesicles to the cytoskeleton
- Vesicles are freed → move to active zones → dock → fuse with membrane (exocytosis)
- ~125 vesicles released per AP (each vesicle = 1 quantum = ~10,000 ACh molecules)
Step 4 - ACh diffuses across cleft and binds nAChRs
- Nicotinic ACh receptors are ligand-gated ion channels (pentameric: 2α, 1β, 1γ, 1δ)
- ACh binds 2 alpha subunits → channel opens
- Na⁺ flows in >> K⁺ flows out → End-plate potential (EPP) generated
Step 5 - End-plate potential triggers muscle AP
- EPP is large enough (always suprathreshold) to depolarize adjacent voltage-gated Na⁺ channels
- Full muscle AP fires (All-or-None)
Step 6 - ACh termination by AChE
- Acetylcholinesterase in the cleft hydrolyzes ACh → acetate + choline
- Choline is taken back up by presynaptic terminal (reused for ACh synthesis)
- This terminates the signal within milliseconds
Applied: Myasthenia Gravis (MG) ⭐
Definition: Acquired autoimmune disorder of the NMJ postsynaptic membrane.
Pathophysiology:
- Autoantibodies (IgG) directed against nicotinic ACh receptors (nAChR) on the postsynaptic muscle membrane
- Antibodies against the Main Immunogenic Region (MIR) of the α subunit
- Mechanism of receptor loss: complement activation + accelerated internalization and destruction of receptors
- Result: Reduced surface density of nAChR → reduced EPP amplitude → failure of NMJ transmission
Key electrophysiology: Miniature end-plate potential (MEPP) amplitude is reduced (fewer receptors), but frequency is normal (quantal release from nerve is intact)
Clinical features:
- Fatigable muscle weakness - worse with repeated use, better after rest
- Ptosis, diplopia (extraocular muscles most commonly affected first)
- Dysphagia, dysarthria, dyspnea
- Bimodal age: women in 20s (thymic hyperplasia) | men in 60s (thymoma)
- Crisis = respiratory muscle weakness → respiratory failure
Two forms:
- Ocular MG - only extraocular muscles
- Generalized MG - all skeletal muscles
Diagnosis:
- Anti-AChR antibodies (positive in ~85%)
- Anti-MuSK antibodies (seronegative MG)
- Tensilon (edrophonium) test - short-acting AChE inhibitor → transient improvement
- Repetitive nerve stimulation: decremental response (amplitude decreases with repeated stimulation)
- Single-fiber EMG: increased jitter
Treatment:
| Approach | Drugs/Methods |
|---|---|
| Enhance ACh | Pyridostigmine (AChE inhibitor) - must titrate carefully |
| Immunosuppression | Corticosteroids, azathioprine, mycophenolate |
| Remove antibodies | Plasmapheresis, IVIG |
| Surgery | Thymectomy (especially if thymoma; 75% improvement) |
Cholinergic crisis vs. Myasthenic crisis: Overdose of AChE inhibitor → excess ACh → persistent depolarization → Na⁺ channels inactivated → paradoxical weakness. Differentiated by edrophonium test (improves myasthenic; worsens cholinergic).
Lambert-Eaton Myasthenic Syndrome (LEMS) - contrast:
- Antibodies against presynaptic voltage-gated Ca²⁺ channels (not AChR)
- Less ACh released
- Weakness improves with repeated use (more Ca²⁺ accumulates)
- Associated with small cell lung cancer
- Incremental response on repetitive nerve stimulation
Sources: Medical Physiology (Boron & Boulpaep); Goodman & Gilman's Pharmacological Basis; Miller's Anesthesia
PART 5: EXCITATION-CONTRACTION COUPLING (ECC) ⭐ IMPORTANT
Molecular Basis of Muscle Contraction (Sliding Filament Theory)
Sarcomere components:
- Thick filament: Myosin (tail + globular head with actin-binding site + ATPase activity)
- Thin filament: Actin + Tropomyosin + Troponin complex
- Troponin C (TnC) - binds Ca²⁺
- Troponin I (TnI) - inhibitory subunit
- Troponin T (TnT) - binds tropomyosin
- At rest: tropomyosin blocks the myosin-binding sites on actin
The Transverse Tubule (T-Tubule) - Sarcoplasmic Reticulum (SR) System
- T-tubules = invaginations of sarcolemma running transversely → carry AP to cell interior
- In skeletal muscle: T-tubule at A-I junction (2 per sarcomere)
- SR surrounds myofibrils; terminal cisternae abut T-tubules
- Triad = 1 T-tubule flanked by 2 terminal cisternae of SR
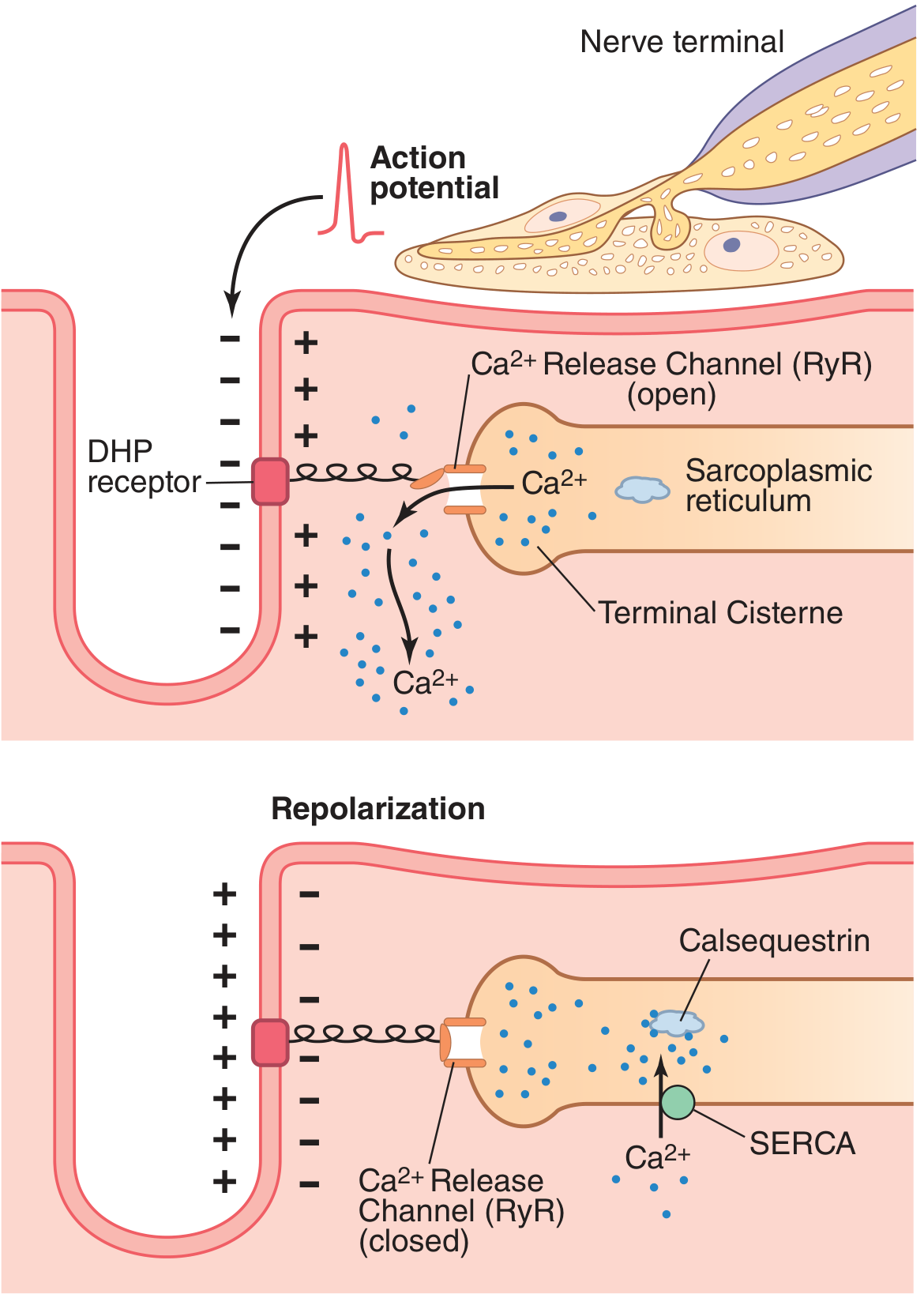
Steps of ECC in Skeletal Muscle
Step 1: Muscle AP spreads along sarcolemma → travels into T-tubules
Step 2: Depolarization of T-tubule detected by Dihydropyridine Receptors (DHPR) = voltage sensors (L-type Ca²⁺ channels) on T-tubule membrane
Step 3: DHPR undergoes conformational change → mechanically linked to Ryanodine Receptors (RyR1) on SR terminal cisternae
Step 4: RyR1 channels open → massive Ca²⁺ release from SR into cytosol
- Ca²⁺ concentration rises from <10⁻⁷ M (resting) to 2×10⁻⁴ M (500-fold increase)
- This is 10× the level needed for maximum contraction
Step 5 - Cross-bridge cycle:
- Ca²⁺ binds Troponin C
- Conformational change in troponin complex → tropomyosin shifts → exposes myosin-binding sites on actin
- Myosin head (with ADP + Pi) attaches to actin → forms cross-bridge
- Power stroke - myosin head pivots → thin filament pulled toward M line (ADP + Pi released)
- New ATP binds → cross-bridge detaches
- ATP hydrolysis re-cocks the myosin head (high-energy configuration)
- Cycle repeats as long as Ca²⁺ is present
In rigor mortis (after death): no ATP → myosin remains attached to actin permanently
Step 6 - Relaxation:
- After AP ends, SERCA (Sarcoplasmic Reticulum Ca²⁺-ATPase) pump actively pumps Ca²⁺ back into SR
- SR concentrates Ca²⁺ ~10,000-fold using ATP
- Calsequestrin inside SR binds up to 40 Ca²⁺ per molecule (storage protein)
- Ca²⁺ concentration in cytosol falls back below threshold → tropomyosin re-blocks actin sites → relaxation
Key Difference: Skeletal vs. Cardiac ECC
| Feature | Skeletal Muscle | Cardiac Muscle |
|---|---|---|
| Ca²⁺ source | SR only (DHPR is voltage sensor, mechanically linked to RyR1) | SR + extracellular (CICR - Ca²⁺-induced Ca²⁺ release via L-type channels) |
| T-tubule location | A-I junction | Z line |
| Ca²⁺ requirement | Independent of extracellular Ca²⁺ | Depends on extracellular Ca²⁺ entry (trigger Ca²⁺) |
| DHPR-RyR coupling | Mechanical (direct) | Calcium-mediated (indirect CICR via RyR2) |
Sources: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7e; Miller's Anesthesia
QUICK PHARMACOLOGY LINKS
| Agent | Mechanism at NMJ |
|---|---|
| Succinylcholine | Depolarizing NMJ blocker (binds nAChR, persistent depolarization) |
| Rocuronium/vecuronium | Non-depolarizing NMJ blocker (competitive antagonist at nAChR) |
| Neostigmine/Pyridostigmine | AChE inhibitor → ↑ ACh (reverses NDMR block, treats MG) |
| Botulinum toxin | Cleaves SNARE proteins → blocks ACh vesicle exocytosis |
| 4-Aminopyridine | K⁺ channel blocker → prolongs AP → more Ca²⁺ entry → more ACh release |
| Ouabain/Digoxin | Inhibits Na-K ATPase |
Primary sources: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7e; Medical Physiology (Boron & Boulpaep); Goodman & Gilman's Pharmacological Basis of Therapeutics; Miller's Anesthesia 10e; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.