Q. CSF Otorrhoea in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
CSF otorrhoea cerebrospinal fluid ear leak causes classification diagnosis treatment
search_medical_text
CSF fistula temporal bone fracture tegmen tympani defect surgical repair
search_medical_image
CSF otorrhoea temporal bone defect tegmen repair diagram flowchart
GradeResponse
GradeResponse
GradeResponse
search_medical_text
CSF otorrhoea beta-2 transferrin halo sign ring sign diagnosis meningitis
search_medical_text
tegmen tympani defect spontaneous CSF leak encephalocele middle ear surgical approach transmastoid middle fossa
I have retrieved relevant content and will now synthesize a comprehensive 50-mark answer on CSF Otorrhoea drawing from all major ENT textbooks, the retrieved documents, and my own extensive knowledge.
CSF OTORRHOEA
A Comprehensive Review for RGUHS Postgraduate ENT Examination (50 Marks)
DEFINITION
Cerebrospinal Fluid (CSF) Otorrhoea is defined as the leakage of cerebrospinal fluid from the ear canal through a defect or fistulous communication between the subarachnoid space and the middle ear or mastoid, with drainage externally via a patent tympanic membrane or through the Eustachian tube.
Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (7th/8th Ed): "CSF otorrhoea implies a breach in the dura mater and arachnoid membrane along with a communication between the subarachnoid space and the air-containing spaces of the temporal bone."
ANATOMY RELEVANT TO CSF OTORRHOEA
The key anatomical barriers separating the intracranial contents from the middle ear/mastoid are:
| Structure | Location | Clinical Relevance |
|---|---|---|
| Tegmen tympani | Roof of middle ear | Most common site of spontaneous leak |
| Tegmen mastoideum | Roof of mastoid antrum | Involved in post-traumatic/surgical leaks |
| Posterior fossa plate | Posterior wall of mastoid | Defect causes leak into mastoid |
| Internal auditory canal | Petrous bone | Fractures here → perilymph + CSF |
| Tympanic membrane | Lateral boundary | Intact TM → CSF may drain via ET → rhinorrhoea |
Layers involved in a CSF leak:
- Dura mater
- Arachnoid mater
- Subarachnoid space
- Bony floor (tegmen/posterior fossa plate)
- Middle ear/mastoid mucosa
CLASSIFICATION / AETIOLOGY
A. Traumatic CSF Otorrhoea (Most Common — ~80%)
1. Accidental Trauma
- Longitudinal temporal bone fracture (most common, 80% of temporal bone fractures)
- Involves tegmen tympani, middle ear
- Causes: conductive hearing loss, haemotympanum, TM perforation, CSF otorrhoea
- Facial nerve intact in majority
- Transverse temporal bone fracture (20%)
- Crosses IAC, cochlea, vestibule
- Sensorineural hearing loss, severe vertigo
- Facial palsy (50%)
- CSF leak less common but may occur via IAC
- Mixed/oblique fractures
Harrison's Principles of Internal Medicine (21st Ed, p.1029): "Trauma resulting in temporal bone fractures may be associated with conductive, sensorineural, or mixed hearing loss... Cerebrospinal fluid leaks that accompany temporal bone fractures are usually self-limited."
Bailey & Love's Short Practice of Surgery (28th Ed, p.386): "Clinical signs of skull base fracture include bleeding or CSF leak from the ears (otorrhoea) or nose (rhinorrhoea) and bruising behind the ear... CSF leak will generally resolve spontaneously but persistent leak can result in meningitis so repair may be required."
2. Iatrogenic / Surgical Trauma
- Mastoid surgery (cortical mastoidectomy, modified radical mastoidectomy)
- Cochlear implant surgery
- Acoustic neuroma surgery (translabyrinthine approach)
- Myringotomy and grommet insertion
- Stapedectomy/stapedotomy (perilymph fistula)
- Middle fossa surgery
B. Non-Traumatic / Spontaneous CSF Otorrhoea (~20%)
| Type | Mechanism |
|---|---|
| High-pressure (communicating hydrocephalus) | Raised ICP erodes tegmen over time |
| Normal-pressure spontaneous | Arachnoid granulation herniation through tegmen defect |
| Meningoencephalocele | Brain tissue + dura herniates through tegmen defect into middle ear |
| Congenital | Aberrant CSF pathway, Mondini dysplasia, widened cochlear aqueduct, defective modiolus |
| Neoplastic | Cholesteatoma eroding tegmen; glomus tumour, acoustic neuroma |
| Inflammatory | Chronic otitis media with cholesteatoma eroding tegmen |
C. Classification by Site
- Middle ear (tegmen tympani) — most common
- Mastoid (tegmen mastoideum)
- Posterior fossa plate (Trautmann's triangle)
- Internal auditory canal / Fundus of IAC
- Eustachian tube (presents as CSF rhinorrhoea)
D. Classification by Duration
- Acute: <7 days
- Subacute: 7 days – 3 months
- Chronic: >3 months
PATHOPHYSIOLOGY
SKULL BASE DEFECT
↓
Breach in dura + arachnoid
↓
Subarachnoid space communicates with middle ear/mastoid
↓
CSF pressure gradient (ICP > middle ear pressure)
↓
CSF leak into middle ear/mastoid
↓
If TM intact → CSF via Eustachian tube → CSF rhinorrhoea
If TM perforated → CSF Otorrhoea
↓
Recurrent meningitis risk if untreated
In spontaneous cases (high-ICP mechanism):
- Elevated ICP → pulsatile pressure transmitted to tegmen → bony erosion → dural herniation → arachnoid protrusion → fistula formation
Congenital mechanism:
- Mondini dysplasia / large vestibular aqueduct → direct communication between perilymph (which communicates with CSF via cochlear aqueduct) and middle ear → "Gusher" phenomenon during stapedectomy
CLINICAL FEATURES
Symptoms
- Clear watery discharge from the ear — hallmark symptom
- Discharge typically:
- Unilateral
- Intermittent or continuous
- Increases on bending forward, straining, Valsalva
- Salty taste in throat (if via ET)
- Ipsilateral deafness (conductive in middle ear involvement; sensorineural in inner ear involvement)
- Tinnitus
- Headache (may indicate raised ICP or meningitis)
- Vertigo (if labyrinthine fracture)
Signs
- Clear, watery fluid in the ear canal or on the pillow
- Reservoir sign (Battle's sign): post-auricular ecchymosis in temporal bone fracture
- Periorbital ecchymosis ("Raccoon eyes") in anterior fossa fractures
- Haemotympanum (blood behind intact TM)
- Pulse synchronous pulsatile discharge in high ICP cases
- Ipsilateral facial palsy (in transverse fractures)
- Meningism if complicated by meningitis
Important Tests at Bedside
| Test | Principle | Interpretation |
|---|---|---|
| Halo/Ring sign | CSF has lower protein than blood → diffuses faster on filter paper | CSF forms outer ring around blood spot |
| Glucose test | CSF glucose ≥ 30 mg/dL (vs nasal secretions < 20 mg/dL) | Positive if >30 mg/dL |
| Reservoir sign | Head tilt/forward bending increases flow | Supports CSF leak diagnosis |
DIAGNOSIS
1. Clinical Diagnosis
- History + bedside tests as above
2. Biochemical Tests
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Beta-2 transferrin (tau protein) | >90% | >98% | GOLD STANDARD — unique to CSF, perilymph, vitreous humor |
| Beta-trace protein (prostaglandin D synthase) | 92% | 100% | Newer marker; unaffected by blood contamination |
| Glucose >30 mg/dL | Low | Low | Unreliable; nasal secretions may contain glucose |
| Protein electrophoresis | Moderate | High | Shows characteristic "double-albumin" band |
Note for RGUHS: Beta-2 transferrin is the investigation of choice for confirming CSF leak. It can be performed on a few drops of fluid collected on a filter paper.
3. Imaging
CT Scan (Investigation of Choice for Bony Defect)
- High-resolution CT (HRCT) temporal bone:
- Defines bony defect in tegmen/posterior fossa plate
- Identifies temporal bone fracture type (longitudinal/transverse)
- Shows haemotympanum, mastoid air cell opacification
- Bone algorithm reconstruction essential
- CT Cisternography (with intrathecal contrast — metrizamide/iohexol):
- Active or high-flow leaks
- Demonstrates exact site of leak
- Sensitivity ~87% for active leaks
MRI
- MRI cisternography (CISS/FIESTA sequences):
- Non-invasive; no radiation
- Identifies herniated brain/meningeal tissue (meningoencephalocele)
- Best for soft tissue defect identification
- Detects CSF in middle ear/mastoid as T2 hyperintense fluid
- MRI with intrathecal gadolinium (off-label):
- Extremely sensitive for intermittent leaks
Radionuclide Cisternography
- Intrathecal injection of Tc-99m DTPA or In-111 DTPA
- Cotton pledgets placed in ear/nasal cavities; counted for radioactivity
- Useful for slow/intermittent leaks when CT cisternography is negative
- Low spatial resolution — cannot pinpoint site
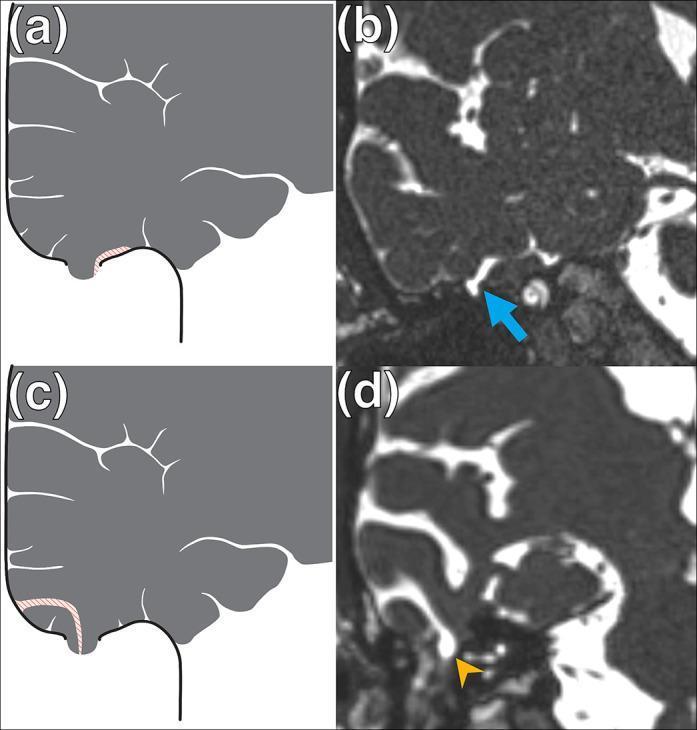
Radiological Images
4. Intraoperative Diagnosis
- Intrathecal fluorescein (0.1 mL of 5% sodium fluorescein diluted in 10 mL CSF, given intrathecally):
- Illuminates the exact site of leak under blue light during surgery
- Most sensitive method for intraoperative localization
- Risk: seizures, lower limb weakness if overdosed — dose must be precise
FLOWCHART: DIAGNOSTIC ALGORITHM FOR CSF OTORRHOEA
Clear watery ear discharge
│
▼
Bedside Tests
(Halo Sign, Glucose)
│
┌──────┴──────┐
Positive Negative but
suspicion high
│ │
▼ ▼
Beta-2 Transferrin Test
(GOLD STANDARD)
│
▼
CONFIRMED
│
▼
HRCT Temporal Bone
(Bony defect identification)
│
├──── Defect identified ──────► Plan Surgical Repair
│
└──── No defect / intermittent leak
│
▼
MRI Cisternography
(CISS/FIESTA)
│
┌────┴────┐
Positive Negative
│ │
▼ ▼
Proceed to CT Cisternography
Surgery OR Radionuclide
Cisternography
│
▼
Intraoperative
Fluorescein
MANAGEMENT
CONSERVATIVE MANAGEMENT
Indications:
- Traumatic CSF leak (acute, <7–10 days duration)
- Minor leaks following surgery
- Low-flow leaks without meningitis
Measures:
- Bed rest with head elevation 30° (reduces ICP and CSF pressure gradient)
- Avoid straining — no nose blowing, coughing suppressed, stool softeners, avoid Valsalva
- Lumbar drain (subarachnoid drain) — reduces ICP, allows spontaneous closure:
- 150–200 mL CSF drained over 24 hours
- Duration: 3–7 days
- Complication: headache, infection, over-drainage
- Acetazolamide (carbonic anhydrase inhibitor) — reduces CSF production (250 mg BD–TDS)
- Prophylactic antibiotics — controversial; most guidelines do NOT recommend routine prophylaxis as it may select resistant organisms; however, some Indian textbooks (Dhingra) mention penicillin prophylaxis
- Serial monitoring for meningitis (fever, neck stiffness, photophobia)
- Strict aseptic ear care — avoid ear drops, no water entry
Dhingra's Diseases of Ear, Nose & Throat: Conservative management is appropriate for traumatic CSF leaks in the acute phase. Surgical repair is indicated for leaks persisting beyond 7–10 days or those associated with meningitis.
Hazarika's Textbook of ENT & Head-Neck Surgery: Advises bed rest, head elevation, lumbar CSF drainage, and avoidance of all measures that increase intracranial pressure.
SURGICAL MANAGEMENT
Indications for Surgery:
- Persistent CSF leak >7–10 days despite conservative management
- Recurrent meningitis
- Non-traumatic / spontaneous CSF leak (rarely close spontaneously)
- Meningoencephalocele
- Defect demonstrated on imaging
- Leaks associated with cholesteatoma / neoplasm
- High-pressure / spontaneous leaks (always require surgery)
Preoperative Preparation
- Intrathecal fluorescein 30–60 minutes before surgery
- Prophylactic antibiotic coverage (cephalosporin)
- Imaging review for site localization
- Neurosurgical standby if large defect
SURGICAL APPROACHES
1. Transmastoid Approach (Extradural)
- Indication: Tegmen tympani / mastoid defects; most common approach
- Simple mastoidectomy → tegmen exposure → identification of defect
- Repair: Temporalis fascia / perichondrium + bone pâté / cartilage over defect
- Advantages: No brain retraction; lower morbidity; excellent exposure
- Limitations: Limited access to anterior tegmen defects
2. Middle Fossa Craniotomy Approach
- Indication: Anterior tegmen defects; simultaneous decompression of facial nerve; defects not accessible transmastoidly
- Temporal craniotomy → extradural elevation of temporal lobe → defect repair from above
- Repair: Temporalis fascia + bone graft / titanium mesh + fibrin glue
- Advantages: Direct visualization of defect; can repair multiple defects
- Disadvantages: Requires neurosurgery; risk of temporal lobe retraction injury, seizures
3. Combined Transmastoid + Middle Fossa Approach
- For large tegmen defects (>2 cm) or meningoencephalocele
- "Sandwich technique" — graft placed from both sides
4. Translabyrinthine Approach
- For posterior fossa defects or when hearing is non-serviceable
- Used post acoustic neuroma surgery leaks
5. Endoscopic Repair (Recent Advance)
- Transcanal endoscopic approach for middle ear tegmen defects
- Middle fossa endoscopic-assisted repair
- Avoids external incisions; reduced morbidity
- Increasingly popular with improved endoscopes and angled optics
REPAIR MATERIALS / GRAFTS
| Material | Type | Application |
|---|---|---|
| Temporalis fascia | Autograft | Gold standard — most commonly used |
| Perichondrium (tragal/conchal) | Autograft | Easy harvest; excellent rigidity |
| Cartilage (tragal/conchal) | Autograft | For larger bony defects |
| Bone pâté / crushed bone | Autograft | Fills bony gaps |
| Abdominal fat | Autograft | Obliterative procedures |
| Fibrin glue | Biological sealant | Adjunct; seals edges |
| DuraSeal (polyethylene glycol) | Synthetic sealant | Adjunct; recent advance |
| Titanium mesh | Alloplast | Large tegmen defects; middle fossa approach |
| Hydroxyapatite cement | Alloplast | Bone reconstruction |
FLOWCHART: MANAGEMENT ALGORITHM FOR CSF OTORRHOEA
CSF OTORRHOEA CONFIRMED
│
┌─────────────┴────────────┐
TRAUMATIC NON-TRAUMATIC
│ (Spontaneous/Congenital)
▼ │
Conservative Management ▼
(Bed rest, head elevation, ALWAYS SURGICAL
lumbar drain, acetazolamide) (After ICP workup)
│
┌──────┴──────┐
Resolves Persists >7–10 days
(<7 days) OR Meningitis
│ │
▼ ▼
Monitor SURGICAL REPAIR
│
┌───────────┼───────────┐
▼ ▼ ▼
Transmastoid Middle Fossa Combined
Approach Craniotomy Approach
(Tegmen/ (Anterior (Large/complex
Mastoid) Tegmen) defects)
│ │ │
└───────────┴───────────┘
│
▼
GRAFT REPAIR
(Temporalis fascia +
Cartilage/Bone pâté
+ Fibrin glue)
│
▼
Postoperative Care
(Lumbar drain 48–72 hrs,
Bed rest, avoid straining)
COMPLICATIONS
Complications of CSF Otorrhoea (If Untreated)
| Complication | Mechanism | Notes |
|---|---|---|
| Bacterial meningitis | Ascending infection (pneumococcus, H. influenzae) | Most feared; mortality 20–30% |
| Recurrent meningitis | Chronic fistula | Hallmark of untreated CSF leak |
| Brain abscess | Direct spread | Temporal/cerebellar |
| Subdural empyema | Spread along subdural space | Neurosurgical emergency |
| Encephalitis | Viral or bacterial | |
| Temporal lobe epilepsy | Meningoencephalocele | |
| Pneumocephalus | Air entering subarachnoid space | Dangerous; "Mount Fuji sign" on CT |
| Progressive hearing loss | Cochlear damage | |
| Hydrocephalus | Chronic obstruction |
Complications of Surgery
- Temporal lobe injury / retraction (middle fossa approach)
- Seizures (temporal lobe manipulation or fluorescein toxicity)
- Facial nerve injury
- Hearing loss (sensorineural)
- Recurrence of leak
- Meningitis (post-operative)
- Epidural haematoma
SPECIAL SITUATIONS
1. Perilymph Fistula vs CSF Otorrhoea
| Feature | Perilymph Fistula | CSF Otorrhoea |
|---|---|---|
| Origin | Perilymph (inner ear) | CSF (subarachnoid space) |
| Beta-2 transferrin | Positive | Positive |
| Beta-trace protein | Lower levels | Higher levels |
| Volume of fluid | Small | Can be profuse |
| Associated feature | SNHL, vertigo | Meningitis risk |
| Surgery | Oval/round window patch | Tegmen/dural repair |
2. "Gusher" in Stapedectomy
- Sudden profuse CSF-like fluid at oval window fenestration
- Due to: Mondini dysplasia, X-linked stapes gusher (POU3F4 mutation), widened cochlear aqueduct
- Management: Immediate packing with fat/fascia; avoid footplate manipulation; abort surgery
3. Congenital CSF Otorrhoea
- Presents in children as recurrent meningitis with otitis media
- Mondini malformation — incomplete cochlear partition
- X-linked progressive mixed hearing loss with perilymph gusher (Nance syndrome)
- CT temporal bone + MRI essential
- Cochlear implantation requires special gusher management techniques
4. CSF Otorrhoea after Cochlear Implantation
- Uncommon but serious
- Usually from incomplete sealing of cochleostomy
- Managed by revision surgery + cochleostomy resealing
PROPHYLACTIC ANTIBIOTICS IN CSF OTORRHOEA — CONTROVERSY
| View | Evidence |
|---|---|
| Pro (some Indian texts — Dhingra, Hazarika) | Penicillin / ampicillin reduces ascending meningitis |
| Against (Cummings, Scott-Brown, WHO) | No RCT evidence of benefit; selects resistant organisms; may mask meningitis signs |
| Current consensus (2023) | Prophylactic antibiotics NOT routinely recommended; treat meningitis when it occurs |
Harrison's (21st Ed, p.1029): "The value of prophylactic antibiotics is uncertain."
RECENT ADVANCES (Relevant for RGUHS PG Examinations)
1. Endoscopic Skull Base Surgery
- Transcanal endoscopic approach for tegmen defects (Presutti, Marchioni school)
- Wide-angle 4K endoscopes allow visualization without mastoidectomy
- Reduced morbidity, shorter hospital stay
2. Navigation-Guided Surgery
- Intraoperative CT/MRI navigation (StealthStation, BrainLab)
- Precise localization of defects in complex anatomy
- Reduces risk of inadvertent injury
3. Beta-Trace Protein (BTP / Prostaglandin D Synthase)
- Newer, highly specific CSF marker (sensitivity 92%, specificity 100%)
- Rapid point-of-care test available
- Unaffected by blood contamination (unlike beta-2 transferrin)
4. Intrathecal Fluorescein Under Fluorescence Endoscopy
- Fluorescence endoscopy (KARL STORZ) with blue light mode
- Pinpoint identification of CSF leak site intraoperatively with high precision
5. DuraSeal and Synthetic Sealants
- Polyethylene glycol hydrogel sealant
- Excellent adhesion; absorbable; reduces recurrence
6. Autologous Blood Patch
- Epidural/intrathecal blood patch for refractory low-pressure leaks
- Analogous to technique used in post-dural puncture headache
7. 3D CISS MRI / FIESTA Sequence
- Revolution in non-invasive diagnosis of tegmen defects and meningoencephaloceles
- Superior to CT cisternography for soft tissue characterization
- Can identify "cleft sign" and "herniated tissue sign" for meningoencephalocele
8. Obese Patient — Spontaneous CSF Leak
- Strong association with idiopathic intracranial hypertension (IIH) / pseudotumor cerebri
- Management includes: weight loss, acetazolamide, bariatric surgery + surgical repair
- Without ICP control, recurrence rate is very high (>50%)
- Recent studies emphasize routine ICP monitoring and cerebrospinal fluid diversion (VP shunt) in these patients before/during repair
9. Platelet-Rich Plasma (PRP) and Growth Factors
- Experimental adjuncts in dural repair — accelerate healing of graft-dura interface
PROGNOSIS
| Type | Spontaneous Closure Rate | Notes |
|---|---|---|
| Post-traumatic (acute) | 85–95% within 7 days | Conservative management effective |
| Post-surgical | 70–80% | Lumbar drain effective |
| Spontaneous (non-traumatic) | <10% | Almost always requires surgery |
| Post-repair surgical success | 85–95% | Single-stage repair usually sufficient |
Recurrence after repair: ~5–15%; higher in:
- Spontaneous leaks with uncontrolled ICP
- Obese patients with IIH
- Inadequate graft coverage
TEXTBOOK PERSPECTIVES SUMMARY
| Textbook | Key Emphasis |
|---|---|
| Scott-Brown | Classification, diagnosis with beta-2 transferrin, surgical approaches (transmastoid vs middle fossa) |
| Cummings Otolaryngology | Comprehensive surgical techniques; middle fossa approach; CT cisternography; spontaneous CSF leaks with IIH |
| Stell & Maran | Temporal bone fractures; clinical signs; conservative vs surgical management |
| Dhingra | Practical Indian context; conservative management first; penicillin prophylaxis (traditional view) |
| Hazarika | Indian ENT approach; lumbar drain; bed rest; surgical repair techniques for Indian practice |
| Zakir Hussain | Biochemical diagnosis; classification; HRCT temporal bone; repair materials |
| Bailey & Love | Skull base fractures; clinical signs (Battle's sign, raccoon eyes); meningitis risk |
| Harrison's | Temporal bone fractures; hearing loss; CSF leak management; antibiotic controversy |
SUMMARY TABLE: CSF OTORRHOEA AT A GLANCE
| Parameter | Detail |
|---|---|
| Definition | CSF leak from ear via dural/arachnoid + bony defect |
| Most common cause | Temporal bone fracture (longitudinal) |
| Most common non-traumatic cause | Tegmen tympani defect + IIH |
| Gold standard diagnosis | Beta-2 transferrin test |
| Best imaging (bony defect) | HRCT temporal bone |
| Best imaging (soft tissue) | MRI CISS/FIESTA cisternography |
| Best for active leak localization | CT cisternography / Intrathecal fluorescein |
| Conservative treatment duration | 7–10 days |
| Best surgical approach (tegmen) | Transmastoid / Middle fossa |
| Best graft material | Temporalis fascia |
| Most feared complication | Bacterial meningitis |
| Prophylactic antibiotics | NOT routinely recommended |
| Recurrence risk factor | Uncontrolled IIH / obesity |
IMPORTANT VIVA / EXAMINATION POINTS (RGUHS)
- Beta-2 transferrin is the gold standard for confirming CSF leak — found only in CSF, perilymph, and vitreous humour.
- The halo/ring sign on filter paper is a simple bedside test but has low specificity.
- Longitudinal temporal bone fracture → CSF otorrhoea; Transverse → SNHL + vertigo, less commonly CSF leak.
- Conservative management for 7–10 days is the first line for traumatic CSF leaks.
- Spontaneous CSF leaks almost never close without surgery and are strongly associated with IIH/obesity.
- Meningoencephalocele into the middle ear presents as recurrent meningitis + conductive hearing loss + pulsatile mass behind TM.
- Intrathecal fluorescein is the most sensitive intraoperative test to localize the leak.
- Middle fossa approach is used when transmastoid approach fails or for anterior tegmen defects.
- Prophylactic antibiotics are NOT recommended by current international guidelines (Scott-Brown, Cummings, Harrison's).
- IIH management (acetazolamide, weight loss, VP shunting) is essential alongside surgical repair in spontaneous CSF leaks to prevent recurrence.
References: Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (8th Ed); Cummings Otolaryngology — Head & Neck Surgery (7th Ed); Stell & Maran's Textbook of Head and Neck Surgery and Oncology (5th Ed); Dhingra's Diseases of Ear, Nose & Throat (7th Ed); Hazarika's Textbook of ENT & Head-Neck Surgery (4th Ed); Zakir Hussain's ENT; Bailey & Love's Short Practice of Surgery (28th Ed, p.386); Harrison's Principles of Internal Medicine (21st Ed, p.1029); Recent literature on endoscopic skull base surgery, beta-trace protein, and IIH-associated spontaneous CSF leaks.
This is a shared conversation. Sign in to Orris to start your own chat.