Mi
It looks like your message got cut off! Could you finish your thought? What would you like help with?
MI
Reading File
search_medical_text
myocardial infarction STEMI NSTEMI pathophysiology diagnosis management
search_medical_text
acute MI ECG findings troponin biomarkers treatment reperfusion
search_medical_image
myocardial infarction ECG ST elevation coronary anatomy
GradeResponse
GradeResponse
GradeResponse
Myocardial Infarction (MI)
Overview
A myocardial infarction occurs when prolonged ischemia leads to irreversible cardiomyocyte death, most commonly due to rupture of an atherosclerotic plaque with superimposed thrombosis occluding a coronary artery. The umbrella term Acute Coronary Syndrome (ACS) encompasses:
| Syndrome | ECG | Biomarkers |
|---|---|---|
| Unstable Angina (UA) | No persistent STE | Negative |
| NSTEMI | No persistent STE | Positive (elevated troponin) |
| STEMI | Persistent ST elevation | Positive |
Epidemiologically, NSTEMIs now outnumber STEMIs (Harrison's, p. 7562).
Pathophysiology
- Atherosclerotic plaque forms in coronary artery wall (lipid core + fibrous cap)
- Plaque rupture or erosion exposes subendothelial collagen → platelet activation + aggregation
- Thrombus formation → partial (NSTEMI/UA) or complete (STEMI) occlusion
- Ischemia → injury → infarction cascade if flow not restored
- Myocyte necrosis releases intracellular proteins (troponin, CK-MB) into bloodstream
Clinical Presentation
- Classic: crushing/pressure-like chest pain radiating to left arm, jaw, or back; diaphoresis, nausea, dyspnea
- Atypical (women, elderly, diabetics): fatigue, epigastric discomfort, syncope, no chest pain ("silent MI")
- Killip classification grades hemodynamic severity (I–IV)
Diagnosis
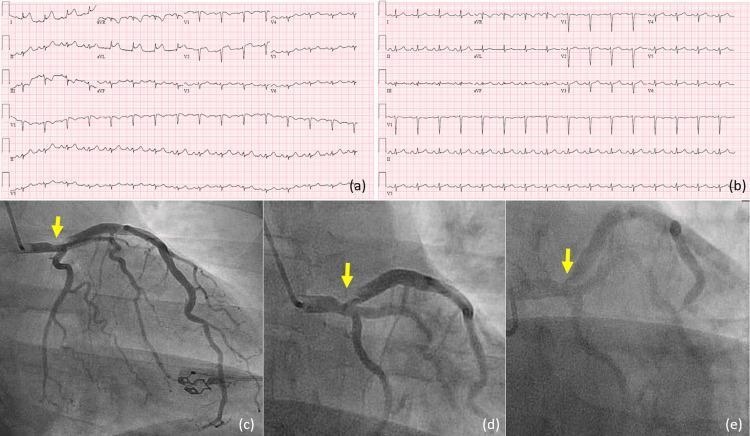
ECG (pivotal triage tool — Harrison's, p. 7562)
The 12-lead ECG is the centerpiece of ACS decision-making:
| Finding | Significance |
|---|---|
| ST elevation ≥1 mm in ≥2 contiguous limb leads | STEMI |
| ST elevation ≥2 mm in ≥2 contiguous precordial leads | STEMI |
| New LBBB | STEMI-equivalent |
| ST depression, T-wave inversions | NSTEMI/UA |
| Hyperacute T-waves | Early/hyperacute MI |
Beyond traditional STE, recognized patterns of Acute Coronary Occlusion MI (ACOMI) include subtle findings in posterior, inferior, high lateral, and right ventricular walls — requiring supplemental leads (V7–V9, V3R/V4R) to detect (Diagnosing and Managing ACS, p. 21).
High lateral MI can present with STE in non-contiguous leads (I, aVL) due to occlusion of the first diagonal branch of the LAD — the "South African flag sign."
Cardiac Biomarkers
- High-sensitivity Troponin I/T — gold standard; rises within 1–3 hours, peaks at 12–24 h
- CK-MB — useful for reinfarction (shorter half-life)
- Serial troponins at 0/1h or 0/3h for rapid rule-in/rule-out protocols
Imaging
- Echocardiography: regional wall motion abnormalities, EF assessment, mechanical complications
- Coronary angiography: defines anatomy, guides PCI
- Cardiac MRI: viability, infarct size, microvascular obstruction
Management
STEMI — Time is Myocardium
Goal: door-to-balloon ≤90 min (PCI-capable center) or door-to-needle ≤30 min (fibrinolysis)
| Strategy | Indication |
|---|---|
| Primary PCI | Preferred if available within 120 min of first medical contact |
| Fibrinolysis (tPA, tenecteplase) | No PCI available within 120 min; administer within 12h of symptom onset |
| CABG | Left main disease, failed PCI, mechanical complications |
NSTEMI/UA — Risk-Stratify First
- TIMI or GRACE score to guide invasive vs. conservative strategy
- Early invasive (<24h): high-risk features (elevated troponin, dynamic ECG changes, hemodynamic instability)
- Conservative: low-risk patients
Pharmacotherapy
| Drug Class | Agents | Role |
|---|---|---|
| Antiplatelet | Aspirin + P2Y12 inhibitor (ticagrelor, prasugrel, clopidogrel) | Dual antiplatelet therapy (DAPT) |
| Anticoagulant | Heparin (UFH/LMWH), bivalirudin, fondaparinux | Acute phase |
| Beta-blocker | Metoprolol, carvedilol | Reduce myocardial oxygen demand, prevent arrhythmia |
| ACE inhibitor/ARB | Ramipril, lisinopril | Reduce remodeling; start within 24h if EF reduced |
| Statin | High-intensity (atorvastatin 40–80 mg) | Plaque stabilization, mortality benefit |
| Nitroglycerin | SL or IV | Pain relief, preload reduction |
| Morphine | IV | Use cautiously (may delay P2Y12 absorption) |
Supplemental Oxygen
Administer only if SpO₂ <90%; routine O₂ in normoxic patients may be harmful.
Complications
| Time | Complication |
|---|---|
| Early (<24h) | VF, complete heart block, cardiogenic shock |
| 1–3 days | Free wall rupture, VSD, papillary muscle rupture (acute MR) |
| Days–weeks | Pericarditis (Dressler's syndrome), LV thrombus, heart failure |
| Long-term | LV remodeling, chronic heart failure, recurrent MI |
Prognosis
- In-hospital mortality for STEMI ~5–10% with modern reperfusion; significantly higher with cardiogenic shock (~50%)
- Key predictors of poor outcome: anterior location, delayed reperfusion, reduced EF, age, comorbidities
- Secondary prevention (DAPT, statin, beta-blocker, ACEI, cardiac rehab) substantially reduces recurrence
Sources: Harrison's Principles of Internal Medicine, 21st Ed. (p. 7562); Diagnosing and Managing Acute Coronary Syndromes (p. 21)
This is a shared conversation. Sign in to Orris to start your own chat.