
Diagnosis and management
Reading File
search_medical_text
anterior STEMI ECG diagnosis ST elevation V1 V2 V3 V4 criteria
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 7569
search_medical_text
STEMI management reperfusion percutaneous coronary intervention thrombolysis guidelines
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 7584
search_medical_image
anterior STEMI ECG ST elevation precordial leads
Hugging Face pmc clinical VQA raw
Page 0
GradeResponse
GradeResponse
GradeResponse
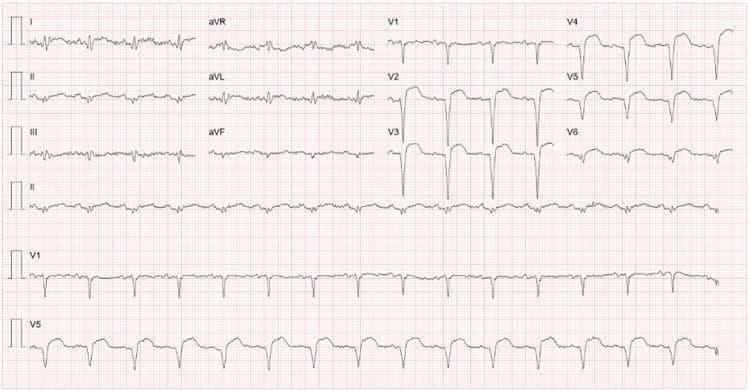
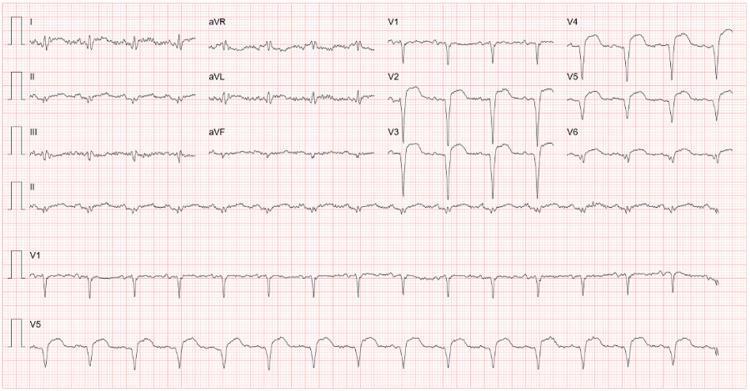
ECG Analysis
Patient: Mr. Aminul Islam, 25M | HR: 90 bpm | Date: April 02, 2026
ECG Findings
| Parameter | Value |
|---|---|
| Heart Rate | 90 bpm |
| PR Interval | 0.14 sec (normal) |
| QRS Duration | 0.076 sec (normal) |
| QT/QTc | 0.196 / 0.241 sec |
| P-QRS-T Axis | 69 / -29 / 45° |
Critical findings from the tracing:
- Massive ST elevation in the precordial leads: V1 (1.81 mm), V2 (4.96 mm), V3 (4.96 mm), V4 (3.29 mm), V5 (2.03 mm), V6 (1.86 mm)
- ST elevation in limb leads: Lead I (0.81 mm), Lead II (1.39 mm), aVL (0.13 mm), aVF (0.90 mm)
- Reciprocal changes: aVR shows ST depression (-1.06 mm), with inferior lead involvement suggesting extensive disease
- Tombstone morphology of ST segments visible in mid-precordial leads
Diagnosis
Extensive Anterior STEMI (ST-Elevation Myocardial Infarction)
The ST elevation from V1 through V6, involving the lateral leads (I, II, aVF), is consistent with proximal Left Anterior Descending (LAD) artery occlusion — sometimes called a "widowmaker" MI. The involvement extending to the lateral and inferior leads suggests either a wrap-around LAD or concomitant right coronary territory involvement, making this an extensive anterior MI.
The deep ST depression in aVR (−1.06 mm) further supports proximal LAD or left main occlusion.
Management
This is a time-critical emergency — "Door-to-balloon time" target: ≤90 minutes
Immediate (First 10 minutes)
- Activate the cardiac catheterization lab immediately — call STEMI alert
- IV access × 2, continuous cardiac monitoring, defibrillator at bedside
- 12-lead ECG confirmation and serial ECGs
- Oxygen — if SpO₂ <90% only (avoid hyperoxia)
- Aspirin 300 mg loading dose (chewed)
- P2Y12 inhibitor loading:
- Ticagrelor 180 mg PO (preferred), or
- Clopidogrel 600 mg PO if ticagrelor unavailable
- Sublingual nitroglycerine — if BP permits (avoid if hypotensive)
- Morphine 2–4 mg IV for pain relief (use cautiously — may delay P2Y12 absorption)
- Anticoagulation: Unfractionated heparin 60 U/kg IV bolus (max 4000 U)
- Labs: Troponin, CBC, BMP, coagulation profile, blood type & cross
Reperfusion Strategy (Harrison's, p. 7584)
| Strategy | Preferred When |
|---|---|
| Primary PCI (1st choice) | PCI-capable center available within 90 min of first medical contact |
| Fibrinolysis (fallback) | PCI not available within 120 min; symptom onset <12h; no contraindications |
Primary PCI is the gold standard — superior to thrombolysis in opening occluded arteries with better short- and long-term outcomes (Harrison's, p. 7584).
If fibrinolysis is chosen (no PCI available):
- Alteplase (tPA): 15 mg IV bolus, then 0.75 mg/kg over 30 min, then 0.5 mg/kg over 60 min
- Streptokinase: 1.5 million units over 60 min
- Absolute contraindications: prior intracranial hemorrhage, active bleeding, recent surgery, severe uncontrolled hypertension
ICU/CCU Monitoring
- Continuous telemetry — this young patient with proximal LAD occlusion is at high risk for:
- Ventricular fibrillation / VT (peak risk first 24–48 h)
- Complete heart block
- Acute heart failure / cardiogenic shock
- Mechanical complications: free wall rupture, VSD, acute MR
Post-Reperfusion Medical Therapy
| Drug | Dose | Indication |
|---|---|---|
| Aspirin | 75–100 mg daily (lifelong) | Antiplatelet |
| Ticagrelor | 90 mg BD × 12 months | Antiplatelet (DAPT) |
| Beta-blocker (metoprolol) | 25–50 mg BD | Reduce remodeling, arrhythmia |
| ACE inhibitor (ramipril) | 2.5–10 mg daily | Reduce LV remodeling |
| Statin (atorvastatin) | 40–80 mg daily | Plaque stabilization |
| Aldosterone antagonist | If EF ≤40% + symptoms | Eplerenone/spironolactone |
Special Consideration — Young Patient (25 years old)
A STEMI at age 25 is uncommon and warrants investigation for:
- Cocaine/stimulant use (coronary spasm or thrombosis)
- Hypercoagulable state (antiphospholipid syndrome, Factor V Leiden)
- Familial hypercholesterolemia
- Spontaneous coronary artery dissection (SCAD)
- Coronary artery anomaly
- Kawasaki disease sequelae
Screen post-stabilization with lipid panel, thrombophilia workup, and toxicology if indicated.
⚠️ This ECG represents a life-threatening emergency requiring immediate activation of the STEMI protocol and urgent reperfusion.
This is a shared conversation. Sign in to Orris to start your own chat.