
Read and diagnosis
Reading File
search_medical_text
ECG ST elevation criteria STEMI diagnosis anterior inferior leads
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 6804
search_medical_image
STEMI ECG ST elevation anterior leads V1 V2 V3
Hugging Face pmc clinical VQA raw
Page 0
GradeResponse
GradeResponse
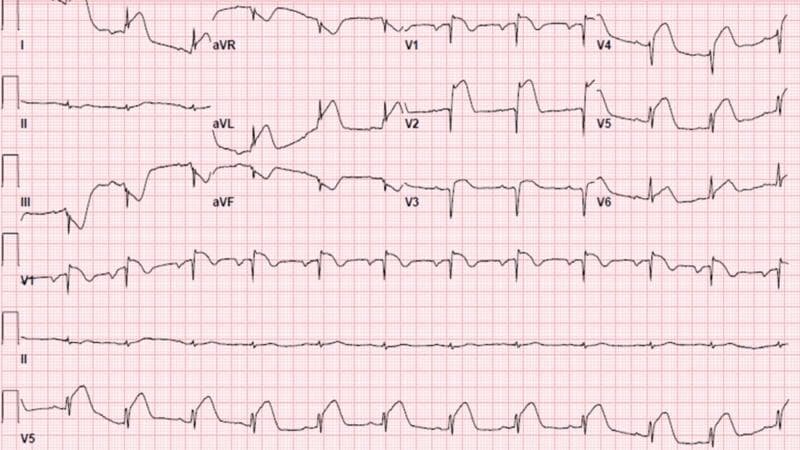
ECG Analysis — Mr. Aminul Islam, 25M
Patient & Technical Data (from the strip)
| Parameter | Value |
|---|---|
| Patient ID | 1260/98 |
| Age/Sex | 25 years, Male |
| Date/Time | April 02, 2026 — 13:12:53 |
| Heart Rate | 90 bpm |
| RR Interval | 0.66 sec |
| PR Interval | 0.14 sec (normal) |
| QRS Duration | 0.076 sec (narrow) |
| QT / QTc | 0.196 / 0.241 sec |
| P-QRS-T Axis | 69° / -29° / 45° |
ST-Level Measurements (machine-reported)
| Lead | ST Level (mm) |
|---|---|
| I | +0.81 |
| II | +1.39 |
| III | +0.45 |
| aVR | -1.06 |
| aVL | +0.13 |
| aVF | +0.90 |
| V1 | +1.81 |
| V2 | +4.96 |
| V3 | +4.96 |
| V4 | +3.29 |
| V5 | +2.03 |
| V6 | +1.86 |
Key ECG Findings
- Massive ST elevation across the precordial leads — most pronounced in V2–V3 (nearly 5 mm each), extending through V1–V6. This is the dominant and most alarming finding.
- Concave/saddle-shaped ST morphology — visible in the precordial leads, which could suggest either early repolarization or acute anterior STEMI (morphology differentiation is critical here).
- Inferior ST elevation — leads II (+1.39 mm) and aVF (+0.90 mm) are also elevated.
- aVR depression (−1.06 mm) — reciprocal, consistent with widespread ST elevation.
- Narrow QRS (76 ms) — no bundle branch block.
- Normal PR interval (140 ms) — sinus rhythm.
- HR 90 bpm — normal sinus rate.
- T-wave axis −29° — mildly abnormal.
Differential Diagnosis
Given a 25-year-old male with this degree of ST elevation, the differential must include:
1. 🔴 Acute Anterior STEMI (Most Dangerous — Must Rule Out First)
- ST elevation in V1–V6 + inferior leads with aVR depression fits a proximal LAD occlusion pattern
- The magnitude (up to 5 mm) is clinically significant
- Even in a young patient, this must be the working diagnosis until proven otherwise
- Per Harrison's (p. 6804): "Acute transmural anterior wall ischemia is reflected by ST elevations in precordial leads V₁–V₆ and leads I and aVL"
2. 🟡 Early Repolarization (Benign Pattern — Common in Young Males)
- Very common in young men aged 17–40
- Typically shows concave ("smiley face") ST elevation in V2–V5, often with notching at the J-point
- ST elevation usually ≤2–3 mm; the 4.96 mm values here are atypically large for benign ER
- No reciprocal depression (aVR depression here could be reciprocal)
3. 🟡 Pericarditis (Acute)
- Diffuse saddle-shaped ST elevation in multiple leads
- Usually associated with PR depression (not clearly documented here)
- Typically spares aVR (aVR depression fits pericarditis)
- Clinical context: chest pain, fever, pleuritic pain
4. 🟠 Brugada Pattern (Less Likely)
- Causes ST elevation in V1–V3 specifically, not the full precordial distribution seen here
⚠️ Clinical Assessment
This ECG is NOT normal and requires urgent clinical correlation.
The combination of:
- ST elevation up to ~5 mm in V2–V3
- Inferior lead elevation (II, aVF)
- aVR depression
- Young male patient
...raises serious concern for an acute coronary event (anterior STEMI), particularly involving the LAD artery. Early repolarization and pericarditis remain on the differential, but the ST magnitudes are too large to dismiss without further workup.
Recommended Immediate Actions
| Priority | Action |
|---|---|
| 🔴 STAT | Serial ECGs every 15–30 minutes to detect dynamic changes |
| 🔴 STAT | High-sensitivity Troponin I/T (baseline + 1h + 3h) |
| 🔴 STAT | Cardiology consultation / activate cath lab if STEMI confirmed |
| 🟡 Urgent | Echocardiography — assess wall motion abnormality |
| 🟡 Urgent | CRP, ESR, CBC — support/exclude pericarditis |
| 🟡 Urgent | Detailed history: chest pain quality, onset, radiation, fever, recent viral illness |
| 🟢 Routine | Electrolytes, renal function |
Reference ECG — Anterior STEMI Pattern
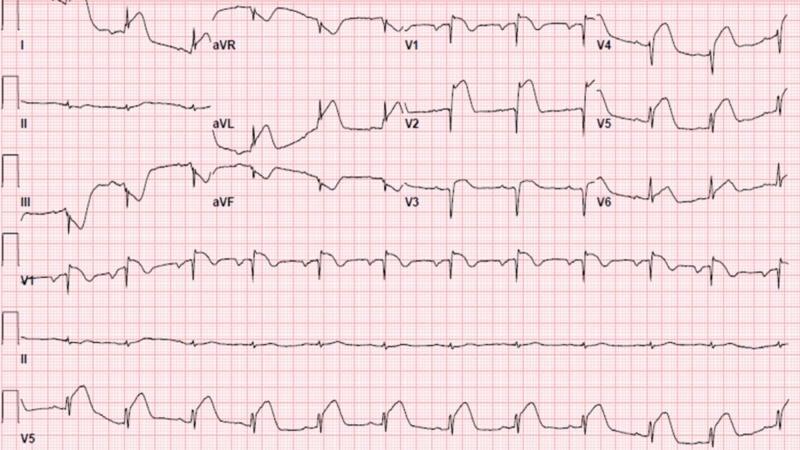
Disclaimer: This ECG analysis is for educational and clinical support purposes only. It does not constitute a final medical diagnosis. A qualified physician must evaluate the patient, correlate clinically, and make all treatment decisions.
This is a shared conversation. Sign in to Orris to start your own chat.