Differential diagnosis for spleenic infarcts
Reading File
search_medical_text
splenic infarct differential diagnosis etiology causes
search_medical_image
splenic infarct CT imaging findings
GradeResponse
GradeResponse
Differential Diagnosis of Splenic Infarcts
Splenic infarction results from either arterial occlusion (embolic/thrombotic) or venous obstruction. The DDx is best organized by mechanism:
Embolic (most common cause overall)
| Condition | Key Features |
|---|---|
| Infective endocarditis | Septic emboli; often multiple infarcts; fever, new murmur |
| Atrial fibrillation | Cardioembolism; left atrial thrombus |
| Dilated cardiomyopathy | LV thrombus source |
| Prosthetic heart valves | Thrombus or vegetation |
| Left atrial myxoma | Tumor embolism; rare but classic |
| Aortic atherosclerosis | Cholesterol/atheroembolism |
Hematological / Thrombotic
| Condition | Key Features |
|---|---|
| Sickle cell disease | Repeated microvascular occlusion → autosplenectomy; most common cause in younger patients |
| Myeloproliferative neoplasms (PV, ET, MF) | Massive splenomegaly + thrombocytosis; high risk |
| Antiphospholipid syndrome | Hypercoagulable; arterial and venous thrombosis |
| Protein C/S deficiency, Factor V Leiden | Thrombophilia screen warranted |
| Paroxysmal nocturnal hemoglobinuria (PNH) | Unusual-site thrombosis |
| TTP / HUS | Microangiopathic occlusion |
| Polycythemia vera | Hyperviscosity + splenomegaly |
Vascular / Local Causes
| Condition | Key Features |
|---|---|
| Splenic artery aneurysm / thrombosis | May be incidental; risk of rupture |
| Splenic vein thrombosis | Associated with pancreatitis, pancreatic carcinoma, post-surgical |
| Portal hypertension | Venous congestion and stasis |
| Vasculitis (e.g., PAN, SLE) | Inflammatory arterial occlusion |
Infiltrative / Structural (splenomegaly → infarction)
| Condition | Key Features |
|---|---|
| Lymphoma / leukemia | Massive splenic infiltration → infarct |
| Metastatic disease to spleen | Rare; may cause segmental infarction |
| Gaucher's disease | Splenic infiltration by glucocerebrosides |
| Amyloidosis | Splenic infiltration |
Iatrogenic / Procedural
- Spleen-preserving distal pancreatectomy
- Splenic artery embolization
- Post-liver/pancreatic transplant vascular complications
Classic Imaging Finding
The characteristic CT appearance is a wedge-shaped hypodensity with its base at the splenic capsule and apex pointing toward the hilum — reflecting the end-arterial vascular anatomy of the spleen.
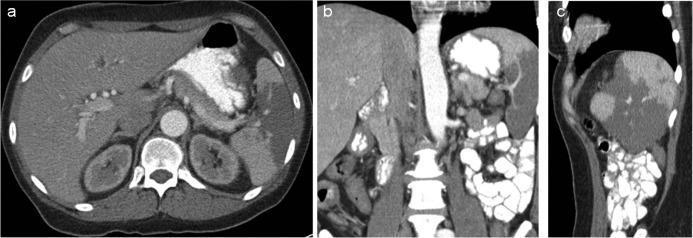
Contrast-enhanced CT showing a well-defined wedge-shaped area of hypodensity in the splenic parenchyma with a peripheral base, consistent with splenic infarction. This pattern is characteristic of embolic occlusion (e.g., septic embolus from endocarditis).
Clinical Approach
- Young patient + multiple infarcts: think sickle cell, thrombophilia, endocarditis
- Atrial fibrillation: cardioembolism first
- Massive splenomegaly: myeloproliferative disease, lymphoma
- Pancreatitis history: splenic vein thrombosis
- Fever + bacteremia: septic emboli from endocarditis
Workup typically includes echocardiography, hypercoagulable panel, CBC with differential, and blood cultures depending on the clinical context. (Bailey and Love's Surgery, 28th ed., p. 1244)
This is a shared conversation. Sign in to Orris to start your own chat.