Pseudo hypo parathyroid
Reading File
search_medical_text
pseudohypoparathyroidism pathophysiology types clinical features
search_medical_text
pseudohypoparathyroidism diagnosis management treatment Albright hereditary osteodystrophy
GradeResponse
GradeResponse
search_medical_text
pseudohypoparathyroidism type 1a 1b 2 GNAS mutation PTH resistance hypocalcemia
search_medical_image
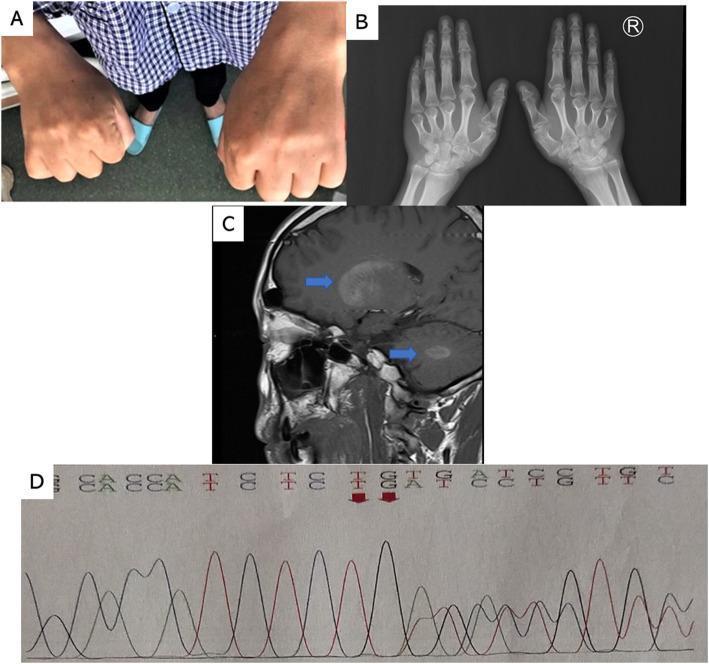
pseudohypoparathyroidism Albright hereditary osteodystrophy features brachydactyly
GradeResponse
Here is a comprehensive overview of Pseudohypoparathyroidism (PHP):
Pseudohypoparathyroidism (PHP)
Definition
PHP is a group of inherited endocrine disorders characterized by end-organ resistance to parathyroid hormone (PTH) — unlike true hypoparathyroidism, where PTH is deficient. In PHP, PTH levels are elevated (or high-normal), yet the kidney and other target tissues fail to respond appropriately, resulting in hypocalcemia and hyperphosphatemia.
Pathophysiology
The defect lies in the PTH receptor signaling cascade:
- PTH binds its receptor (PTH1R) → activates Gs-alpha (Gsα) protein → stimulates adenylyl cyclase → generates cAMP → downstream effects (phosphaturia, 1,25-OH₂D production, calcium reabsorption)
- In PHP, a mutation or imprinting defect in the GNAS gene (encoding Gsα) impairs this cascade
- Failure to produce 1,25(OH)₂D → impaired intestinal calcium absorption
- Impaired phosphate excretion → hyperphosphatemia
- Result: hypocalcemia despite elevated PTH
Classification
| Type | Mechanism | AHO Features | PTH Resistance | Other Hormone Resistance |
|---|---|---|---|---|
| PHP Type Ia (PHP1A) | Heterozygous loss-of-function GNAS mutation (maternal allele) | Present | Yes | TSH, LH/FSH, GHRH resistance also |
| PHP Type Ib (PHP1B) | Imprinting defect at GNAS locus (methylation abnormality) | Absent | Yes | Primarily PTH; sometimes mild TSH |
| PHP Type Ic | Gsα activity normal in vitro but AHO phenotype present | Present | Yes | Similar to Ia |
| PHP Type II | Normal urinary cAMP response to PTH but no phosphaturia | Absent | Partial (post-cAMP defect) | Usually isolated |
| Pseudopseudohypoparathyroidism (PPHP) | GNAS mutation (paternal allele) | Present | No | None |
Key distinction: In PHP1A, the mutated allele is maternally inherited (GNAS is imprinted — only maternal allele expressed in kidneys). In PPHP, the paternal allele is mutated → AHO features but normal calcium/phosphate metabolism.
Albright's Hereditary Osteodystrophy (AHO)
AHO is the somatic phenotype seen in PHP1A and PPHP:
- Brachydactyly — shortened 4th and 5th metacarpals/metatarsals (most characteristic)
- Short stature
- Obesity
- Round facies
- Subcutaneous ossifications (ectopic bone)
- Developmental delay / intellectual disability
- Dental anomalies
Clinical Features of Hypocalcemia in PHP
- Neuromuscular irritability: tetany, Chvostek's sign, Trousseau's sign
- Perioral and peripheral paresthesias
- Carpopedal spasm
- Seizures (in severe hypocalcemia)
- Prolonged QT interval on ECG
- Cataracts (chronic)
- Basal ganglia calcification (Fahr's syndrome-like appearance on CT/MRI)
Biochemical Profile
| Parameter | PHP | True Hypoparathyroidism |
|---|---|---|
| Serum Ca²⁺ | Low | Low |
| Serum PO₄ | High | High |
| PTH | Elevated | Low/undetectable |
| Urinary cAMP | Low/no rise after PTH | Rises normally |
| 1,25(OH)₂D | Low | Low |
| Magnesium | Normal | Check (hypoMg → ↓PTH) |
Diagnosis
- Biochemistry: Hypocalcemia + hyperphosphatemia + elevated PTH (confirms resistance, not deficiency)
- Ellsworth-Howard Test (historical): Exogenous PTH infusion → measure urinary cAMP and phosphate
- PHP1: blunted cAMP and phosphate response
- PHP2: normal cAMP but blunted phosphaturia
- GNAS molecular genetics: Sequencing for mutations/methylation defects
- Imaging: Hand X-ray (metacarpal shortening), brain CT (basal ganglia calcification), DXA (bone density)
- TSH/LH/FSH/IGF-1: Screen for multi-hormone resistance in PHP1A
Management
Hypocalcemia
- Calcium supplementation: Oral calcium carbonate or citrate (1–3 g elemental calcium/day)
- Active vitamin D (calcitriol): 0.25–2 µg/day — critical since 1α-hydroxylation is impaired
- Monitor: serum calcium, urine calcium/creatinine ratio (hypercalciuria risk)
- Acute tetany: IV calcium gluconate (10 mL of 10% solution slowly)
Multi-hormone resistance (PHP1A)
- Hypothyroidism: Levothyroxine replacement (TSH resistance common)
- Growth hormone deficiency: GH therapy if documented (GHRH resistance)
- Hypogonadism: Sex hormone replacement if indicated
AHO features
- No specific treatment for brachydactyly or short stature beyond GH therapy
- Weight management for obesity
- Subcutaneous ossifications: surgical excision if symptomatic
Key Pearls
- PHP is the only condition where PTH is high yet the patient is hypocalcemic and hyperphosphatemic — distinguish from vitamin D deficiency (phosphate is typically low/normal)
- PPHP has AHO features but normal calcium — same GNAS mutation, different parental origin (imprinting)
- Always check TSH in PHP1A — subclinical hypothyroidism is common and often overlooked
- Hypomagnesemia can mimic PHP by impairing PTH secretion AND causing PTH resistance — always check Mg²⁺ first
- Brain CT may show basal ganglia calcification due to chronic hypocalcemia
Sources: Harrison's Principles of Internal Medicine, 21st Edition (pp. 11614, 3188–3190)
This is a shared conversation. Sign in to Orris to start your own chat.