Abdominal incisions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from Schwartz's Principles of Surgery. Let me compile a thorough answer.
Abdominal Incisions
Abdominal Wall Anatomy - Foundation
Before choosing an incision, understanding the abdominal wall layers is essential. From superficial to deep:
- Skin
- Subcutaneous tissue - superficial fatty layer (Camper's fascia) + deep membranous layer (Scarpa's fascia)
- External oblique - fibers run inferomedially ("hands in pockets")
- Internal oblique - fibers run superomedially
- Transversus abdominis - fibers run transversely
- Transversalis fascia
- Extraperitoneal fat
- Parietal peritoneum
The rectus abdominis runs vertically in its sheath (linea semilunaris laterally, linea alba medially). The rectus sheath has an important landmark: the arcuate line (semicircular line of Douglas), below which all aponeurotic layers pass anterior to the rectus, leaving the posterior rectus uncovered by a fascial layer.
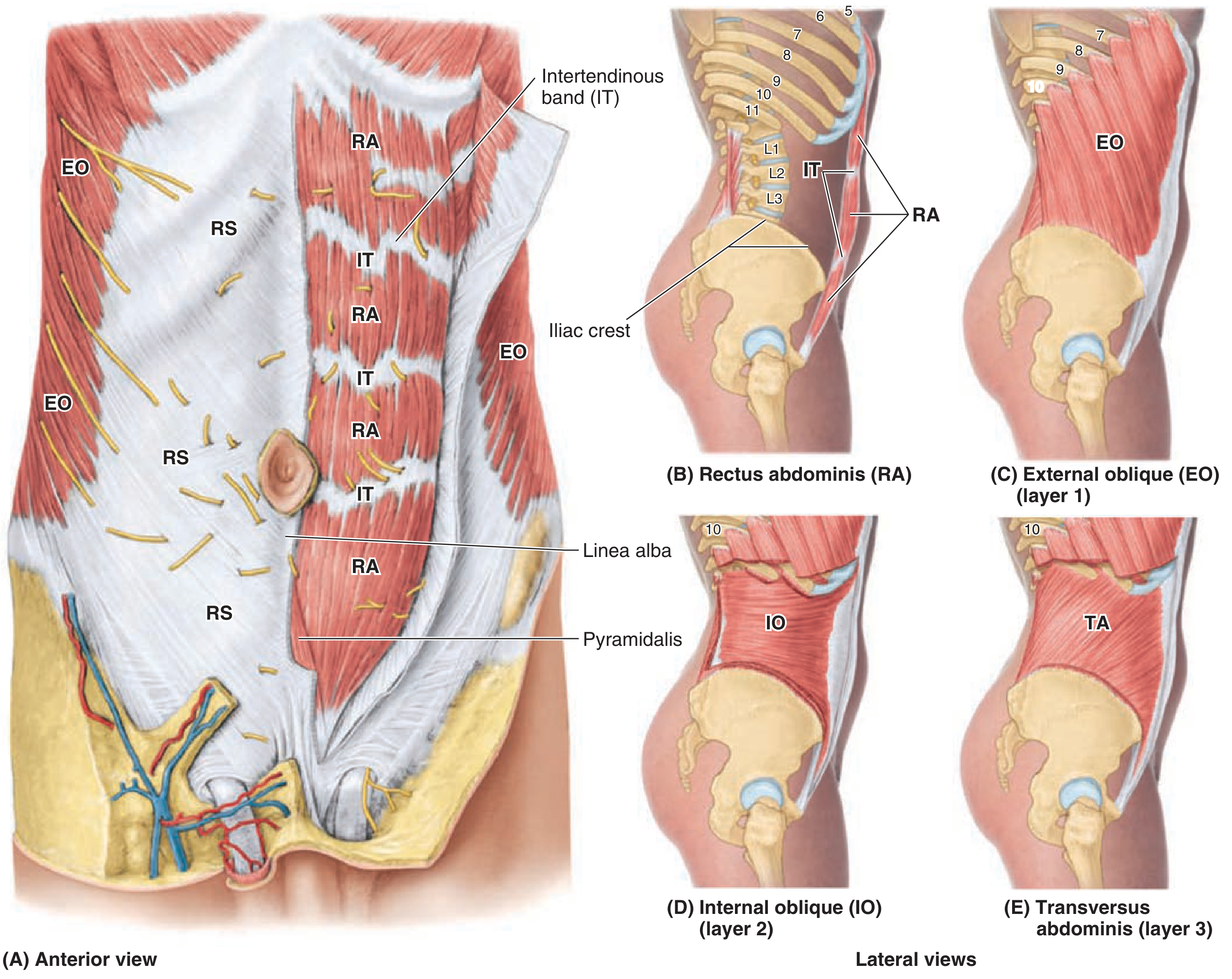
Anterior abdominal wall muscles with rectus sheath reflected on left side (Schwartz's Principles of Surgery)
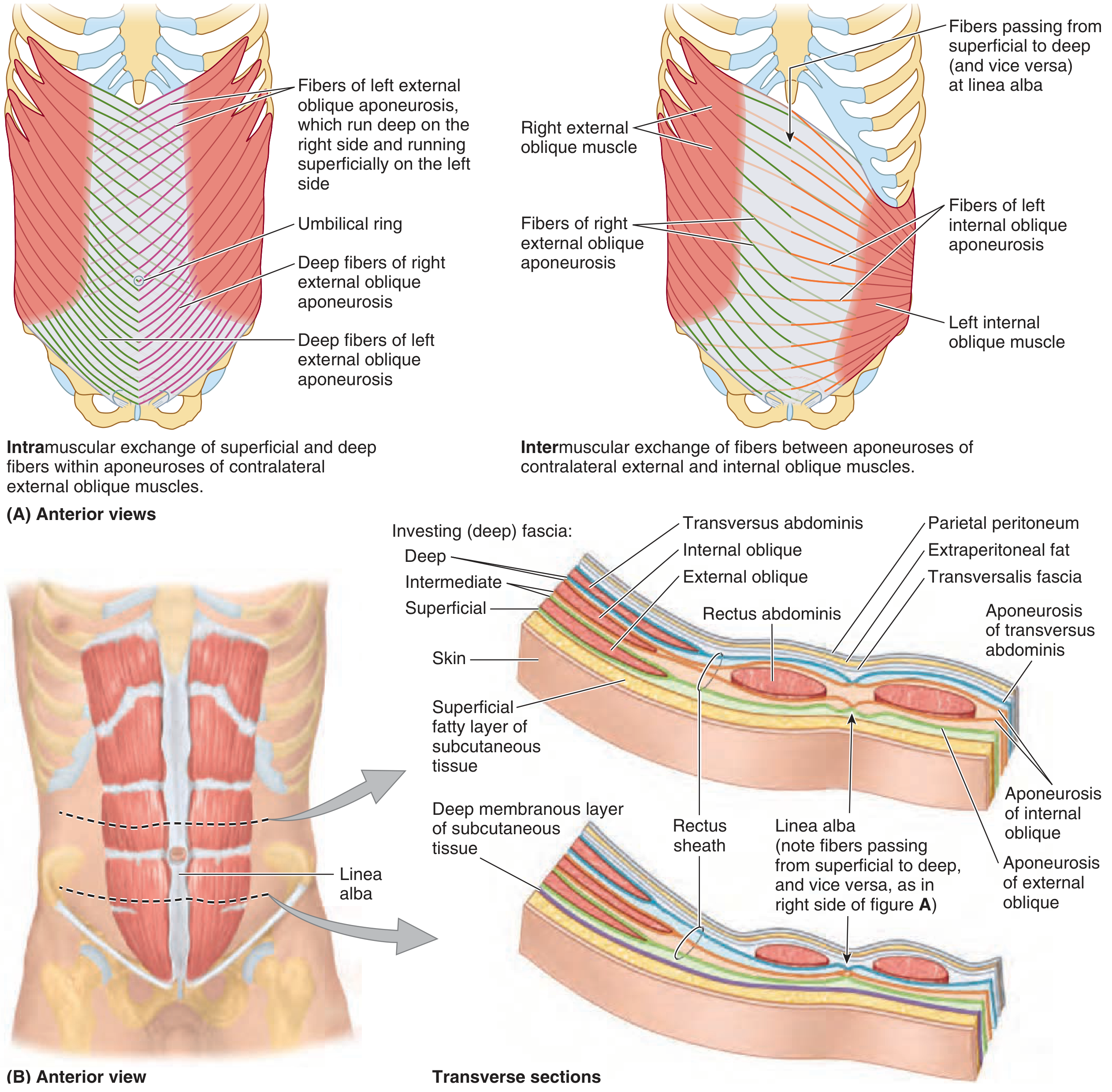
Cross-sectional anatomy above and below the arcuate line (Schwartz's Principles of Surgery)
General Principles
- Incisions should be located in proximity to the operative target
- The goal is adequate exposure with minimal perturbation of abdominal wall function
- Two general types: longitudinal vs. transverse/oblique
- No clear evidence of superiority between types; choice remains surgeon-dependent
- Transverse incisions may have lower incisional hernia rates but higher wound infection rates
Types of Abdominal Incisions
Here is the classic reference diagram showing all major incision positions:
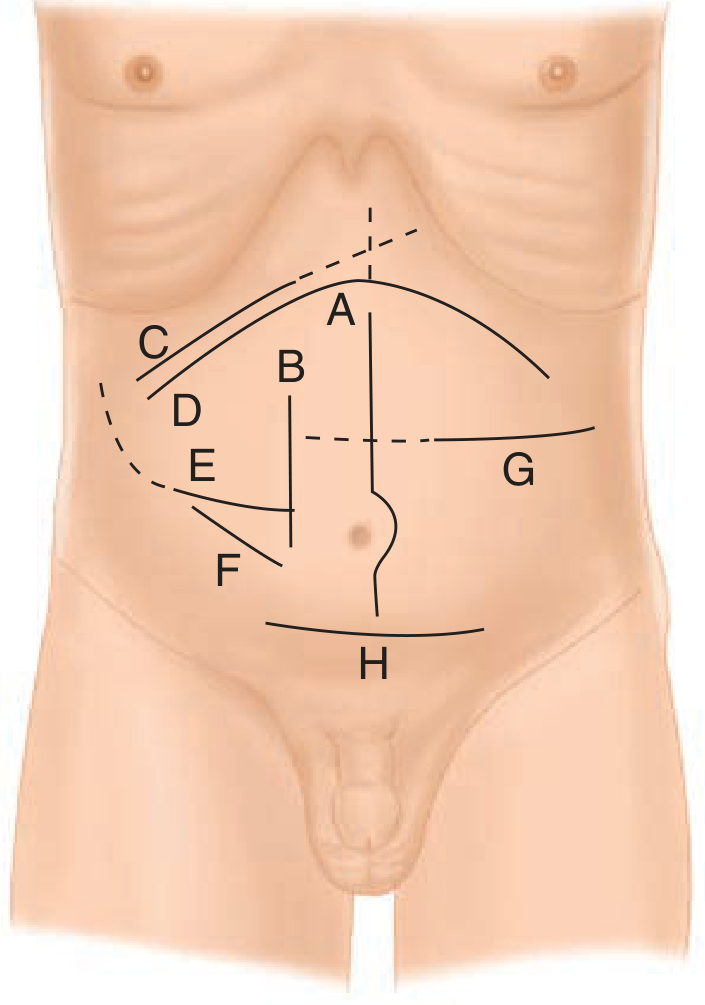
A. Midline | B. Paramedian | C. Right subcostal with saber-slash extension (dashed) | D. Bilateral subcostal/chevron with Mercedes-Benz extension (dashed) | E. Rocky-Davis | F. McBurney | G. Transverse | H. Pfannenstiel (Schwartz's Principles of Surgery, Fig. 35-4)
1. Midline Incision (Median Laparotomy)
| Feature | Details |
|---|---|
| Direction | Longitudinal, along linea alba |
| Layers cut | Skin, subcutaneous tissue, linea alba, peritoneum |
| Muscles cut | None (passes through avascular linea alba) |
| Access | Most intraabdominal organs; some retroperitoneal structures |
| Advantage | Quick, minimal bleeding, easily extensible, no nerve/vessel injury |
| Disadvantage | Higher incisional hernia risk than transverse |
| Variants | Upper midline (xiphoid to umbilicus), lower midline (umbilicus to pubis), full midline |
Closure: Fascia is reapproximated using sutures placed 1 cm from the edge, 1 cm apart. Recent European RCTs show reduced hernia rates with shorter stitch width (5-8 mm). Prophylactic mesh is under investigation.
2. Paramedian Incision
| Feature | Details |
|---|---|
| Position | Lateral to midline, through rectus sheath or pararectus |
| Variants | Through-and-through rectus (medial), pararectus (lateral to sheath) |
| Disadvantage | Restricts access to contralateral abdomen/pelvis; risks damage to rectus musculature, vessels (epigastric vessels), and nerves |
| Use | Largely superseded by midline in modern practice |
3. Transverse Incision
| Feature | Details |
|---|---|
| Direction | Horizontal |
| Advantage | Follows Langer's lines (better cosmesis), less respiratory compromise, lower hernia rate |
| Disadvantage | Limited exposure; muscles must be divided or split |
| Use | Pediatric surgery; specific upper/lower abdominal access |
4. Subcostal Incision (Kocher's Incision)
| Feature | Details |
|---|---|
| Position | Parallel and 2-3 cm below costal margin |
| Layers | Skin, external oblique, internal oblique, transversus, transversalis fascia |
| Access | Liver, gallbladder, spleen, pancreas, adrenal glands |
| Right subcostal | Cholecystectomy, right hepatectomy |
| Left subcostal | Splenectomy, left adrenalectomy |
| Closure | Two layers: deep (internal oblique + transversus + transversalis fascia) and superficial (anterior rectus sheath + external oblique aponeurosis) |
| Extension | "Saber slash" = right subcostal extended medially; bilateral subcostal = chevron incision |
Bilateral subcostal (Chevron/Roof-top incision): Used for liver transplantation, bilateral adrenalectomy, pancreaticoduodenectomy. A Mercedes-Benz modification adds a midline extension superiorly for access to upper abdomen or lower mediastinum.
5. McBurney's Incision
| Feature | Details |
|---|---|
| Position | Oblique, centered at McBurney's point (1/3 of the way from ASIS to umbilicus) |
| Type | Muscle-splitting (grid-iron) incision |
| Access | Appendix |
| Advantage | Muscle fibers of external oblique, internal oblique, and transversus are split (not cut) along their fiber direction - preserves function |
| Extension | Weir's extension (medially) or Rutherford-Morrison extension (laterally and superiorly) for better access |
Rocky-Davis incision is a transverse variant at the same point, allowing muscle splitting in a cosmetically superior transverse direction.
6. Pfannenstiel Incision
| Feature | Details |
|---|---|
| Position | Transverse skin incision in suprapubic region (2-3 cm above pubic symphysis) |
| Steps | Transverse skin + subcutaneous incision → transverse incision of anterior rectus sheath → sheath dissected off rectus muscles superiorly and inferiorly → rectus muscles separated in midline → longitudinal access through transversalis fascia/peritoneum |
| Access | Pelvis - uterus, bladder, iliac vessels, rectum |
| Use | Cesarean section, hysterectomy, bladder surgery, prostatectomy |
| Closure | Peritoneum + rectus muscles + anterior rectus sheath |
| Advantage | Excellent cosmesis; low hernia rate; strong closure |
| Disadvantage | Limited access outside pelvis; slower than midline |
7. Gridiron vs. Lanz Incision
| Gridiron (McBurney) | Lanz | |
|---|---|---|
| Direction | Oblique (along EO fibers) | Transverse (horizontal) |
| Position | McBurney's point | Right iliac fossa (more transverse) |
| Cosmesis | Poorer | Better |
| Access | Adequate for appendix | Adequate for appendix |
Laparoscopic Port Site Incisions
- Port placement must be carefully planned based on approach angles, working distances to operative site, and distances between ports
- A nasogastric tube and Foley catheter should decompress stomach and bladder to reduce entry injury
- Hasson (open) technique: Direct visualization, systematic opening of each fascial layer - preferred in patients with prior surgery
- Veress needle (closed) technique: Blind entry confirmed by saline drop test or intraabdominal pressure measurement
- Retrospective data suggests fewer complications with Hasson, but small RCTs show no significant difference
Complications of Abdominal Incisions
| Complication | Notes |
|---|---|
| Hematoma/Seroma | Early; risk higher with oblique/muscle-dividing incisions |
| Surgical site infection (SSI) | Most common early complication of open abdominal surgery |
| Fascial dehiscence | Early (days 5-8); risk factors: infection, malnutrition, obesity, steroids, diabetes |
| Incisional hernia | Most common late/long-term complication |
| Nerve injury | Cutaneous nerves of abdominal wall (dermatomal distribution T7-L1) |
Closure of Abdominal Incisions
Risk factors for wound failure: diabetes mellitus, malnutrition, obesity, corticosteroid use.
Fascial Closure Options:
| Method | Description |
|---|---|
| Mass closure | Single layer closing all fascial layers en masse (±peritoneum) - preferred for efficiency |
| Layered closure | Separate anterior + posterior aponeurotic sheaths; some evidence of higher dehiscence |
| Continuous vs. interrupted | Continuous is faster; some debate on superiority |
| Suture material | Slowly absorbable (PDS - 180 days, Maxon - 180 days) preferred over rapidly absorbable (Vicryl 60-90 days) or nonabsorbable |
Suture material resorption times (Maingot's Abdominal Operations):
| Material | Resorption (days) |
|---|---|
| Catgut | 15 |
| Chromic catgut | 90 |
| Polyglycolic acid (Dexon) | 20 |
| Polyglactin (Vicryl) | 60-90 |
| Polydioxanone (PDS) | 180 |
| Polyglyconate (Maxon) | 180 |
| Nylon, Polypropylene, Polyethylene | Non-resorbable |
Quick Reference Summary
| Incision | Use | Key Feature |
|---|---|---|
| Midline | Universal access | Avascular linea alba; fastest entry |
| Paramedian | Limited modern use | Muscle risks |
| Subcostal (Kocher's) | Liver, GB, spleen | Parallel to costal margin |
| Chevron/Roof-top | Liver transplant, bilateral adrenal | Bilateral subcostal |
| McBurney/Gridiron | Appendectomy | Muscle-splitting |
| Rocky-Davis | Appendectomy | Transverse muscle-splitting |
| Pfannenstiel | OB/GYN, bladder, pelvis | Cosmetic; strong closure |
| Transverse | Pediatric, specific access | Follows Langer's lines |
Sources: - Schwartz's Principles of Surgery, 11th Ed., Ch. 35 | - Maingot's Abdominal Operations, Ch. 6
This is a shared conversation. Sign in to Orris to start your own chat.