Differential diagnosis of sinus arrhythmia
Reading File
search_medical_text
sinus arrhythmia differential diagnosis ECG
search_medical_text
irregular heart rhythm differential diagnosis respiratory non-respiratory sinus arrhythmia
GradeResponse
GradeResponse
The retrieval was limited, so I'll synthesize a comprehensive answer drawing from the retrieved content and established medical knowledge.
Differential Diagnosis of Sinus Arrhythmia
Sinus arrhythmia refers to a cyclical variation in the sinus rate producing an irregular rhythm where all beats remain of sinus origin (normal P wave morphology: upright in I, II, III; biphasic in V₁). The key diagnostic challenge is distinguishing it from other causes of an irregular rhythm.
Types of Sinus Arrhythmia
| Type | Mechanism | Key Feature |
|---|---|---|
| Respiratory (phasic) | Vagal tone fluctuates with respiration; rate increases with inspiration, decreases with expiration | Rate variation disappears with breath-holding — most common, physiologic |
| Non-respiratory | Vagal fluctuations unrelated to breathing | Does not resolve with breath-holding; seen in digitalis toxicity, inferior MI, increased ICP |
| Ventriculophasic | P-P interval containing a QRS is shorter than one without | Seen in complete heart block; not a true primary sinus arrhythmia |
Differential Diagnosis
1. Atrial Fibrillation (AF)
- Irregularly irregular rhythm with no discernible P waves; fibrillatory baseline
- Most important to exclude — sinus arrhythmia is regularly irregular (cyclic), while AF has no pattern
- Rate can be similar; look for organized P waves on 12-lead ECG
2. Wandering Atrial Pacemaker (WAP)
- P wave morphology changes (≥3 distinct P wave morphologies) as pacemaker shifts among atrial foci, AV node
- Rate usually 60–100 bpm; PR interval varies
- May coexist with sinus arrhythmia; key differentiator is changing P wave axis
3. Multifocal Atrial Tachycardia (MAT)
- Like WAP but rate >100 bpm
- ≥3 distinct P wave morphologies, variable P-P, PR, and R-R intervals
- Commonly associated with COPD, hypomagnesemia
4. Sinoatrial (SA) Exit Block
- Type I (Wenckebach): progressive P-P shortening before a dropped P wave (pause < 2× the preceding P-P)
- Type II: sudden pause that is a exact multiple of the basic P-P interval
- P wave morphology is normal (sinus origin), but rhythm is not cyclically modulated by respiration
5. Sinus Pause / Sinus Arrest
- Abrupt cessation of sinus activity; pause is not a multiple of the normal P-P interval
- May be followed by an escape beat (junctional or ventricular)
- Distinguished from sinus arrhythmia by abruptness and longer pause duration
6. Premature Atrial Complexes (PACs)
- Irregular rhythm from early ectopic beats; P wave has different morphology from sinus P
- Non-compensatory pause follows; bigeminal PACs can mimic alternating rhythm
7. Premature Junctional Complexes (PJCs)
- Retrograde P waves (inverted in II, III, aVF) or absent P waves preceding QRS
- Irregular rhythm but morphologically distinct
8. Second-degree AV Block (Mobitz I / Wenckebach)
- Progressive PR prolongation then dropped QRS; P-P interval is regular
- Can create apparent R-R irregularity; careful P wave analysis resolves it
9. Atrial Flutter with Variable Block
- "Sawtooth" flutter waves at ~300 bpm; variable ventricular response creates irregular rhythm
- F waves clearly visible in II, III, aVF, and V₁
Differentiating Features at a Glance
| Feature | Sinus Arrhythmia | AF | WAP | SA Block | PACs |
|---|---|---|---|---|---|
| P waves present | ✓ (normal) | ✗ | ✓ (variable) | ✓ | ✓ (abnormal) |
| P wave morphology | Constant | None | ≥3 types | Constant | Changes with ectopic |
| Varies with respiration | ✓ (respiratory type) | ✗ | ✗ | ✗ | ✗ |
| Pause pattern | Gradual, cyclic | — | — | Mathematic multiple | Non-compensatory |
| PR interval | Constant | — | Variable | Constant | May differ |
Clinical Approach
- Obtain a 12-lead ECG — identify P wave morphology and axis (sinus P: upright I, II, aVF)
- Ask patient to hold breath — if irregularity resolves, respiratory sinus arrhythmia is confirmed
- Assess PR interval — constant PR with normal P morphology strongly supports sinus arrhythmia
- Measure P-P intervals — gradual cyclical variation vs. abrupt pauses vs. missing P waves
- Longer rhythm strips (lead II or V₁) help characterize periodicity
Clinical Significance
- Respiratory sinus arrhythmia is a normal, benign finding, particularly in young, healthy individuals and athletes; it reflects healthy vagal tone and heart rate variability
- Non-respiratory sinus arrhythmia warrants investigation for underlying causes (digitalis toxicity, inferior wall MI, elevated ICP, sinus node dysfunction)
- Treatment is directed at the underlying cause, not the arrhythmia itself
(Harrison's Principles of Internal Medicine, 21st ed., p. 6998 — sinus node anatomy and P wave characterization)
Ecg changes explained
search_medical_text
sinus arrhythmia ECG changes P wave RR interval variation
search_medical_image
sinus arrhythmia ECG rhythm strip
GradeResponse
GradeResponse
search_medical_text
ECG interpretation P wave PR interval QRS normal sinus rhythm criteria
search_medical_image
normal sinus rhythm ECG P wave QRS complex
GradeResponse
GradeResponse
Here is a thorough breakdown of the ECG changes in sinus arrhythmia, building on the previous differential discussion.
ECG Changes in Sinus Arrhythmia
The Baseline: What Normal Sinus Rhythm Looks Like
Before identifying sinus arrhythmia, understanding the normal ECG is essential.
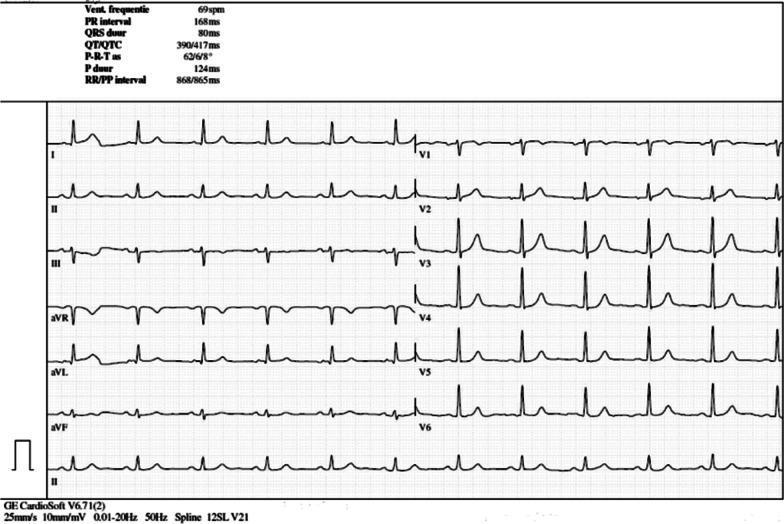
Normal sinus rhythm at 69 bpm — regular P waves before every QRS, PR 168 ms, narrow QRS 80 ms, normal axis. (Harrison's, p. 6923)
Core ECG Features of Sinus Arrhythmia
1. P Wave — Normal and Constant
| Parameter | Finding |
|---|---|
| Morphology | Upright in leads I, II, aVF |
| Morphology in V₁ | Biphasic (positive-negative) |
| Axis | 0° to +75° (normal sinus axis) |
| Duration | < 120 ms |
| Consistency | Same shape in every beat — this is the critical distinguishing point |
- Because the pacemaker never leaves the sinus node, P wave morphology and axis do not change from beat to beat
- A changing P wave axis immediately suggests wandering atrial pacemaker, not sinus arrhythmia
2. PR Interval — Normal and Constant
- Normal range: 120–200 ms
- Does not lengthen or shorten between beats
- Constancy of the PR interval confirms the impulse is consistently conducting through the AV node without delay
- Variable PR would suggest WAP, MAT, or a conduction abnormality
3. R-R Interval — The Defining Feature
This is where sinus arrhythmia announces itself.
| Criterion | Value |
|---|---|
| Definition of irregularity | Variation in P-P (and R-R) interval > 120 ms (or >10% of the mean P-P) between the longest and shortest cycle |
| Pattern | Cyclic and gradual — rate accelerates smoothly then decelerates smoothly |
| In respiratory type | Rate increases during inspiration (R-R shortens), decreases during expiration (R-R lengthens) |
| In non-respiratory type | Same cyclic variation but not linked to breathing |
Key distinction: The variation is phasic and predictable, not random (which would suggest AF) and not abrupt (which would suggest a pause or block).
4. QRS Complex — Normal
- Narrow: < 120 ms
- Morphology is identical in every beat (same ventricular conduction)
- Aberrant QRS would suggest a bundle branch block or ventricular ectopy, neither of which is part of sinus arrhythmia
5. ST Segment and T Waves — Normal
- No ST elevation or depression
- T waves upright and concordant with QRS in lateral leads
- These are unaffected by sinus arrhythmia per se
6. QTc Measurement — Special Consideration
Because R-R intervals vary, QTc calculation is affected. Bazett's formula (QTc = QT / √RR) is inaccurate when R-R variability is high. The correct approach is to use a representative (median) R-R interval, not the shortest R-R, to avoid overestimating the QTc. (Management of the Patient with a Prolonged QT Interval, p. 2)
Summary ECG Checklist for Sinus Arrhythmia
| ECG Parameter | Expected Finding |
|---|---|
| Rhythm | Irregularly irregular, but cyclically so |
| P waves | Present before every QRS; normal, constant morphology |
| P wave axis | Normal (upright I, II, aVF) |
| PR interval | Normal (120–200 ms), constant |
| QRS | Narrow (< 120 ms), identical morphology each beat |
| R-R variation | > 120 ms difference between longest and shortest |
| Pattern of variation | Gradual, phasic; correlates with respiration |
| ST/T waves | Normal |
| Response to breath-holding | Irregularity resolves (respiratory type) |
Practical ECG Reading Tip
On a rhythm strip, mark out consecutive P-P intervals with calipers:
- Gradual lengthening then shortening in a cyclic pattern = sinus arrhythmia
- Sudden drop (missing P) = sinus pause or SA block
- No visible P waves = AF
- Different P wave shapes = WAP or PACs
The hallmark is that every beat is still "sinus" — the pacemaker never moves, the impulse just fires a little faster or slower with each breath.
This is a shared conversation. Sign in to Orris to start your own chat.