Diagnostic criteria for arrhythmia associated with impaired automaticity Diagnostic criteria for an attack of atrial paroxysmal tachycardia
arrhythmia impaired automaticity diagnostic criteria ECG
atrial paroxysmal tachycardia attack diagnostic criteria ECG
sick sinus syndrome sinoatrial node automaticity bradycardia diagnosis criteria
focal atrial tachycardia paroxysmal SVT P wave morphology RP interval diagnosis
I. Arrhythmias Associated with Impaired Automaticity
Pathophysiology
A. Sick Sinus Syndrome (SSS) / Sinus Node Dysfunction
Diagnostic Criteria
| Feature | Criterion |
|---|---|
| Symptomatic sinus bradycardia | Resting HR < 50 bpm with correlating symptoms (dizziness, syncope, fatigue) |
| Sinus arrest / sinus pause | P–P pause > 3 seconds (or > 2 s with symptoms) without identifiable external cause |
| Sinoatrial exit block | Grouped beats with P–P intervals that are multiples of the basic P–P cycle (Type II); Wenckebach-type progressive shortening before a dropped P (Type I) |
| Tachycardia-bradycardia syndrome | Alternation between SVT (most often AF) and prolonged post-conversion pause > 3 s |
| Chronotropic incompetence | Failure to achieve ≥ 85% of age-predicted max HR during standard exercise test |
ECG Findings
- Persistent sinus bradycardia (HR < 40–50 bpm)
- Long, inappropriate sinus pauses
- Slow junctional escape rhythm (40–60 bpm) or ventricular escape (20–40 bpm) when sinus fails
- Post-tachycardia pauses in tachy-brady syndrome
B. AV Junctional Escape Rhythm
C. Idioventricular Escape Rhythm
D. General ECG Approach (Harrison's, p. 6937)
"The ECG is the cornerstone and most important diagnostic test… evidence suggesting underlying cardiac disease, such as prior MI, LVH, atrial disease, or baseline conduction system disease may suggest a diagnosis."
- Rate below expected escape rate for the pacemaker level in question
- P wave absence or abnormality (inverted, retrograde, absent)
- Escape morphology (narrow = junctional; wide = ventricular)
- AV dissociation without block (competing slow rhythms)
II. Diagnostic Criteria for an Attack of Atrial Paroxysmal Tachycardia (APT)
Clinical Diagnostic Criteria
| Feature | Criterion |
|---|---|
| Onset/offset | Abrupt ("paroxysmal") start and termination |
| Rate | Atrial rate 150–250 bpm (typically 150–200 bpm) |
| Regularity | Regular (occasionally slight irregularity possible, especially at onset) |
| Symptoms | Palpitations, dyspnea, chest discomfort, lightheadedness; may tolerate well or present with hemodynamic compromise |
| Response to vagal maneuvers / adenosine | Transiently slows ventricular rate by increasing AV block but does not terminate the tachycardia (distinguishes from AVNRT/AVRT) |
ECG Diagnostic Criteria
1. P Wave Morphology
- P waves present and precede each QRS (long RP tachycardia pattern typical)
- P wave morphology differs from sinus P wave — the axis depends on the focus location:
- High right atrium (near SA node): P wave resembles sinus; tall, upright in II, III, aVF
- Low right atrium / coronary sinus: Negative P in II, III, aVF (inferiorly directed focus)
- Left atrium: Negative P in V1 reversal, positive in inferior leads
2. RP/PR Relationship
- Typically long RP interval (RP > PR); P wave falls clearly before the next QRS
- RP > 70 ms (P wave visible before QRS, not buried within or immediately after it)
3. Rate and AV Conduction
- Atrial rate 150–250 bpm
- 1:1 AV conduction is common; variable block (2:1, Wenckebach) may occur at faster rates
- AV block during tachycardia does not terminate it — the atria continue at the same rate (hallmark distinguishing AT from AVNRT/AVRT)
4. QRS Complex
- Narrow (< 120 ms) unless aberrant conduction or pre-existing BBB
- Wide-complex APT can occur with BBB — must differentiate from VT
5. Warm-Up / Cool-Down Phenomenon
- Gradual acceleration at onset and gradual slowing at termination (distinguishes from AVNRT/AVRT, which start/stop abruptly)
Differential Diagnosis of SVT (Harrison's, p. 6993)
| SVT Type | Key Distinguishing Feature |
|---|---|
| Focal AT (APT) | P wave precedes QRS; long RP; AV block does not terminate; warm-up/cool-down |
| AVNRT | P wave within or just after QRS (pseudo R' in V1, pseudo S in inferior leads); short RP |
| Orthodromic AVRT | Retrograde P wave after QRS (RP > 70 ms); terminates with AV block; delta wave in sinus |
| Sinus tachycardia | P identical to sinus; gradual onset; responds to vagal maneuvers |
| Atrial flutter | Sawtooth flutter waves 250–350 bpm; fixed ratio AV block |
Summary Table
| Criterion | Impaired Automaticity Arrhythmias | Atrial Paroxysmal Tachycardia |
|---|---|---|
| Mechanism | Decreased phase-4 depolarization in SA node | Enhanced automaticity or triggered activity in ectopic atrial focus |
| Rate | < 50 bpm (bradycardia/escape) | 150–250 bpm |
| P wave | Absent, retrograde, or normal but slow | Present, abnormal morphology vs. sinus |
| QRS | Narrow (junctional) or wide (ventricular) | Narrow (usually) |
| Response to vagal/adenosine | May increase rate transiently (reflexive) | AV block without termination |
| Key ECG | Pauses, sinus arrest, escape rhythms | Long RP, abnormal P axis, warm-up phenomenon |
Diagnostic criteria for arrhythmia associated with impaired automaticity
impaired automaticity sinus node dysfunction bradyarrhythmia ECG diagnostic criteria
sick sinus syndrome sinus arrest sinoatrial block escape rhythm diagnosis
sinus bradycardia sinus arrest ECG impaired automaticity
Diagnostic Criteria for Arrhythmias Associated with Impaired Automaticity
Background: Mechanism
1. Sinus Bradycardia
Diagnostic Criteria
- Rate: < 60 bpm (clinically significant < 50 bpm)
- P wave: Normal morphology (upright in I, II, aVF; biphasic or inverted in V1), positive in inferior leads — confirming sinus origin
- PR interval: Normal (120–200 ms)
- QRS: Normal narrow complex, each preceded by a P wave
- Rhythm: Regular
Clinical significance
2. Sinus Node Dysfunction (Sick Sinus Syndrome)
"Intrinsic sinus node disease is sometimes referred to as sick sinus syndrome or sinus node dysfunction (SND) and can manifest as fatigue, exercise intolerance, or syncope resulting from either reduced heart rate or pauses. Electrocardiographic recording plays a central role in the diagnosis and management of SA node dysfunction. The correlation between symptoms and slow heart rate or pauses is essential in determining whether bradycardia may be considered pathologic and necessitating intervention."
Diagnostic Criteria
| Manifestation | ECG / Clinical Criterion |
|---|---|
| Symptomatic sinus bradycardia | HR persistently < 50 bpm with correlated symptoms |
| Sinus pause / sinus arrest | Sudden cessation of P waves; pause > 2–3 seconds; no P–QRS complexes during pause |
| Sinoatrial (SA) exit block | P–P intervals that are multiples of basic cycle (Type II); or Wenckebach-type progressive P–P shortening before a dropped beat (Type I) |
| Tachycardia-bradycardia syndrome | Alternating SVT (often AF/flutter) and prolonged post-conversion pauses > 3 s |
| Chronotropic incompetence | Failure to reach ≥ 85% age-predicted max HR during exercise testing |
3. Sinus Arrest vs. Sinoatrial Exit Block
"Sinus arrest results from failure of impulse formation within the sinus node. Sinoatrial exit block results from failure of sinus node activity to propagate to the atrium."
Differentiating the Two
| Feature | Sinus Arrest | SA Exit Block |
|---|---|---|
| Mechanism | Failure of impulse formation (true impaired automaticity) | Impulse forms but fails to propagate |
| Pause duration | Unrelated to basic P–P interval (not a multiple) | Pause = exact multiple of P–P interval (Type II) |
| ECG appearance | Irregular pause; no P wave; often followed by escape beat | Grouped beating pattern; missing P waves at predictable intervals |
| Type I (Wenckebach) | N/A | Progressive P–P shortening before dropped P wave |
| Type II (Mobitz) | N/A | Sudden dropped P wave; pause = 2× (or 3×) normal P–P |
ECG Example: Sinus Arrest with Sinus Bradycardia

4. Escape Rhythms (Subsidiary Pacemaker Activation)
A. AV Junctional Escape Rhythm
- Rate: 40–60 bpm
- QRS: Narrow (< 120 ms), normal morphology
- P waves: Absent, retrograde (negative in II, III, aVF), or dissociated from QRS
- Regularity: Regular
B. Idioventricular Escape Rhythm
- Rate: 20–40 bpm
- QRS: Wide (> 120 ms), LBBB or RBBB morphology
- P waves: Absent or AV dissociation present
- Regularity: Regular
- Indicates failure of both SA and AV nodal automaticity
5. Enhanced Vagotonia / Drug-Induced Impaired Automaticity
- Beta-blockers, calcium channel blockers, digoxin, amiodarone — suppress SA automaticity
- Vasovagal / carotid sinus hypersensitivity — transient excessive parasympathetic tone
- Hypothyroidism, hypothermia, hypoxia, hyperkalemia — metabolic suppression
Diagnostic Algorithm Summary
Bradyarrhythmia suspected
│
▼
12-lead ECG + rhythm strip
│
┌─────┴──────┐
Sinus Escape rhythm
bradycardia (junctional or ventricular)
│
├─ Asymptomatic → likely physiologic (athlete, sleep)
│
└─ Symptomatic → Holter / MCT monitoring
│
┌─────────┴──────────┐
Sinus arrest SA exit block
(pause ≠ multiple (pause = exact
of P–P) multiple of P–P)
│
Tachycardia-bradycardia?
│
Diagnose SSS / SND
Key Diagnostic Pearls
- Symptom-rhythm correlation is mandatory — incidental sinus bradycardia alone is not diagnostic of pathologic SND (Harrison's, p. 6949)
- A pause > 3 seconds while awake is generally considered pathologic
- Junctional escape during a pause is a normal protective response, not an additional pathology
- Distinguish sinus arrest (non-multiple pause) from SA exit block (multiple of P–P cycle) — both represent failure at different points of impulse generation/propagation
- Resting ECG is insufficient alone — prolonged monitoring is required for intermittent dysfunction
Diagnostic criteria for arrhythmia associated with impaired automaticity
impaired automaticity sinus node dysfunction bradyarrhythmia ECG diagnostic criteria
sick sinus syndrome sinus arrest sinoatrial block escape rhythm diagnosis ECG
sinus bradycardia sinus arrest sinoatrial block ECG impaired automaticity
Diagnostic Criteria for Arrhythmias Associated with Impaired Automaticity
Pathophysiological Basis
| Level | Rate |
|---|---|
| SA node | 60–100 bpm |
| AV junction (junctional) | 40–60 bpm |
| His-Purkinje / ventricular | 20–40 bpm |
Classification of Arrhythmias from Impaired Automaticity
1. Sinus Bradycardia
- Heart rate < 60 bpm (clinically significant when < 50 bpm)
- P wave: Normal sinus morphology — upright in I, II, aVF; biphasic/inverted in V1
- P–QRS relationship: Each P wave is followed by a QRS; PR interval 120–200 ms
- QRS: Narrow (< 120 ms), normal morphology
- Rhythm: Regular
2. Sinus Node Dysfunction (Sick Sinus Syndrome — SSS)
"Intrinsic sinus node disease is sometimes referred to as sick sinus syndrome or sinus node dysfunction (SND) and can manifest as fatigue, exercise intolerance, or syncope resulting from either reduced heart rate or pauses. The correlation between symptoms and slow heart rate or pauses is essential in determining whether bradycardia may be considered pathologic and necessitating intervention."
| Manifestation | Criterion |
|---|---|
| Symptomatic sinus bradycardia | HR persistently < 50 bpm with correlated symptoms |
| Sinus pause / sinus arrest | Sudden absence of P waves and QRS complexes; pause > 2–3 s; duration not a multiple of the basic P–P interval |
| SA exit block (Type I — Wenckebach) | Progressive shortening of P–P intervals before a dropped P wave cycle |
| SA exit block (Type II — Mobitz) | Sudden absent P wave; pause = exact multiple (2×, 3×) of the basic P–P interval |
| Tachycardia-bradycardia syndrome | Alternation of SVT (often AF/atrial flutter) with prolonged post-conversion pauses > 3 s |
| Chronotropic incompetence | Failure to achieve ≥ 85% of age-predicted maximum HR during standard exercise testing |
3. Sinus Arrest vs. Sinoatrial Exit Block — Key Distinction
| Feature | Sinus Arrest | SA Exit Block |
|---|---|---|
| Mechanism | Failure of impulse formation in the SA node (true impaired automaticity) | Impulse forms but fails to propagate to atrial myocardium |
| Pause duration | Unrelated to basic P–P interval (not a multiple) | Exact multiple of P–P interval (Type II) |
| ECG pattern | Irregular, unpredictable pause; often terminated by an escape beat | Grouped beating (bigeminy-like grouping); regularly missing P waves |
| Post-pause beat | Usually an escape (junctional or ventricular) | Next sinus beat resumes at expected interval |
ECG Illustration: Abnormal Sinus Rhythms
4. Escape Rhythms (Subsidiary Pacemaker Activation)
A. AV Junctional Escape Rhythm
- Rate: 40–60 bpm
- QRS: Narrow (< 120 ms), normal morphology
- P waves: Absent, retrograde (negative in II, III, aVF), or dissociated from QRS
- Rhythm: Regular
- Significance: Indicates SA node failure with intact AV junctional automaticity
B. Idioventricular Escape Rhythm
- Rate: 20–40 bpm
- QRS: Wide (> 120 ms), LBBB or RBBB morphology
- P waves: Absent or AV dissociation present
- Rhythm: Regular
- Significance: Failure of both SA node and AV junctional automaticity; hemodynamically unstable
5. Extrinsic Causes of Impaired Automaticity (Must Be Excluded)
| Cause | Mechanism |
|---|---|
| Beta-blockers, non-DHP calcium channel blockers, digoxin, amiodarone | Pharmacological suppression of phase-4 depolarization |
| Vagal hypersensitivity (vasovagal, carotid sinus syndrome) | Excessive parasympathetic tone |
| Hypothyroidism, hypothermia, hypoxia | Metabolic suppression |
| Hyperkalemia | Reduced resting membrane potential; depresses automaticity |
| Inferior MI (RCA occlusion) | Ischemia of SA nodal artery |
Diagnostic Algorithm
Bradyarrhythmia / pauses suspected
│
▼
12-lead ECG + rhythm strip
│
┌─────────┴──────────┐
Sinus bradycardia Escape rhythm present
│ (junctional or ventricular)
│
├─ Asymptomatic → Likely physiologic
│
└─ Symptomatic → Holter / MCT monitoring
│
┌────────┴─────────┐
Sinus arrest SA exit block
(pause ≠ multiple (pause = exact
of P–P) multiple of P–P)
│
Tachy-brady alternation?
│
Diagnose SSS / SND
Key Diagnostic Pearls
- Symptom-rhythm correlation is mandatory — asymptomatic sinus bradycardia alone does not constitute pathologic SND (Harrison's, p. 6949)
- A pause > 3 seconds while awake is generally considered pathologic and warrants investigation
- Sinus arrest (failure of impulse formation) is the purest expression of impaired automaticity
- SA exit block involves intact node firing but conduction failure — a distinction important for ablation and pacemaker planning
- Junctional escape during a pause is a normal protective response, not an independent pathology
- Resting ECG alone is insufficient for intermittent dysfunction — prolonged ambulatory monitoring is the diagnostic standard
Diagnostic criteria for arrhythmia associated with impaired automaticity
impaired automaticity sinus node dysfunction bradyarrhythmia diagnostic criteria ECG
sinus arrest sinoatrial exit block escape rhythm junctional idioventricular ECG criteria
sinus bradycardia sinus arrest sinoatrial block ECG rhythm strip
Diagnostic Criteria for Arrhythmias Associated with Impaired Automaticity
Pathophysiological Basis
| Level | Intrinsic Rate |
|---|---|
| SA node | 60–100 bpm |
| AV junction | 40–60 bpm |
| His-Purkinje / ventricle | 20–40 bpm |
Classification and Diagnostic Criteria
1. Sinus Bradycardia
- Heart rate < 60 bpm (clinically significant when persistently < 50 bpm)
- P wave: Normal sinus morphology — upright in I, II, aVF; biphasic or inverted in V1
- P–QRS relationship: Every P wave followed by a QRS; PR interval 120–200 ms
- QRS: Narrow (< 120 ms), normal morphology
- Rhythm: Regular
Pathologic only when symptomatic. Physiologic in athletes and during sleep.
2. Sinus Node Dysfunction (Sick Sinus Syndrome — SSS)
"Intrinsic sinus node disease… can manifest as fatigue, exercise intolerance, or syncope resulting from either reduced heart rate or pauses. The correlation between symptoms and slow heart rate or pauses is essential in determining whether bradycardia may be considered pathologic and necessitating intervention."
| Manifestation | Criterion |
|---|---|
| Symptomatic sinus bradycardia | HR persistently < 50 bpm with correlated symptoms (fatigue, presyncope, syncope) |
| Sinus pause / sinus arrest | Sudden absence of P waves + QRS complexes; pause > 2–3 seconds; duration not a multiple of the basic P–P interval |
| SA exit block — Type I (Wenckebach) | Progressive shortening of P–P intervals before a dropped P wave cycle |
| SA exit block — Type II (Mobitz) | Sudden absent P wave; pause = exact multiple (2×, 3×) of basic P–P interval |
| Tachycardia-bradycardia syndrome | Alternation between SVT (most often AF/flutter) and prolonged post-conversion pauses > 3 s |
| Chronotropic incompetence | Failure to reach ≥ 85% age-predicted maximum HR during exercise testing |
3. Sinus Arrest vs. Sinoatrial Exit Block — Critical Distinction
| Feature | Sinus Arrest | SA Exit Block |
|---|---|---|
| Mechanism | Failure of impulse formation in SA node (pure impaired automaticity) | Impulse forms but fails to propagate to atrial myocardium |
| Pause duration | Not a multiple of basic P–P interval | Exact multiple of P–P interval (Type II) |
| Type I variant | Not applicable | Progressive P–P shortening (Wenckebach) before a dropped cycle |
| Type II ECG sign | Unpredictable pause length | Sinus rate abruptly halves (every other beat blocked) |
| Post-pause beat | Escape beat (junctional or ventricular) | Next sinus beat resumes at expected interval |
"Type II second-degree SA block can be inferred on the ECG if the sinus rate abruptly transitions to a rate that is half the previous rate… Sinoatrial Wenckebach can be inferred from progressive shortening of the P–P interval leading up to a sinus pause." — Harrison's, p. 6956
ECG Illustration: Abnormal Sinus Rhythms Associated with Impaired Automaticity
4. Escape Rhythms (Subsidiary Pacemaker Activation)
A. AV Junctional Escape Rhythm
- Rate: 40–60 bpm
- QRS: Narrow (< 120 ms), normal morphology
- P waves: Absent, retrograde (negative in II, III, aVF), or dissociated from QRS
- Rhythm: Regular
- Significance: SA node failure with intact AV junctional automaticity
B. Idioventricular Escape Rhythm
- Rate: 20–40 bpm
- QRS: Wide (> 120 ms), LBBB or RBBB morphology
- P waves: Absent or AV dissociation present
- Rhythm: Regular
- Significance: Failure of both SA and AV junctional automaticity; often hemodynamically unstable
5. Extrinsic Causes to Exclude Before Diagnosing Intrinsic SND
| Cause | Mechanism |
|---|---|
| Beta-blockers, non-DHP CCBs, digoxin, amiodarone | Pharmacological suppression of phase-4 depolarization |
| Vagal hypersensitivity (vasovagal, carotid sinus syndrome) | Excessive parasympathetic tone |
| Hypothyroidism, hypothermia, hypoxia | Metabolic suppression of automaticity |
| Hyperkalemia | Reduced resting membrane potential; depresses pacemaker activity |
| Inferior MI (RCA/SA nodal artery occlusion) | Ischemic suppression of SA node |
Key Diagnostic Pearls
- Symptom-rhythm correlation is mandatory — incidental sinus bradycardia alone is not pathologic SND (Harrison's, p. 6949)
- Pauses > 3 seconds while awake are generally considered pathologic
- Sinus arrest is the purest expression of impaired automaticity (failure of impulse formation)
- SA exit block involves intact node firing with conduction failure — an important mechanistic distinction for management
- Junctional escape during a pause is a normal protective response, not an independent pathology
- Resting ECG alone is insufficient — prolonged ambulatory monitoring is the diagnostic standard for intermittent dysfunction
- Other SA block types require invasive electrophysiological study (EPS) for precise characterization (Harrison's, p. 6956)
ecg of arrythmia
ECG arrhythmia sinus bradycardia tachycardia atrial fibrillation flutter rhythm strip
ventricular tachycardia fibrillation heart block ECG
ECG of Arrhythmias
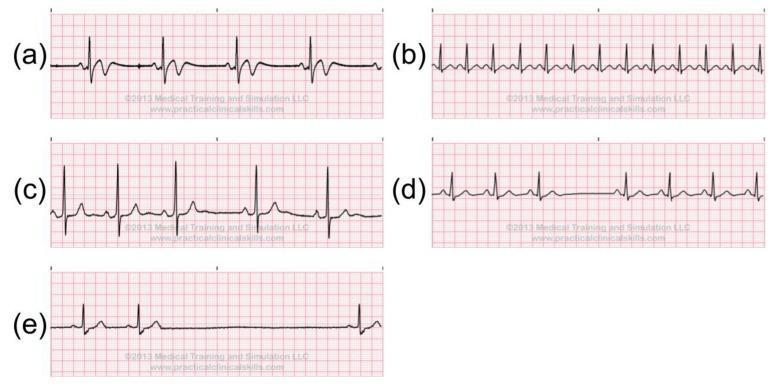
Overview: Multi-Arrhythmia Comparison Strip
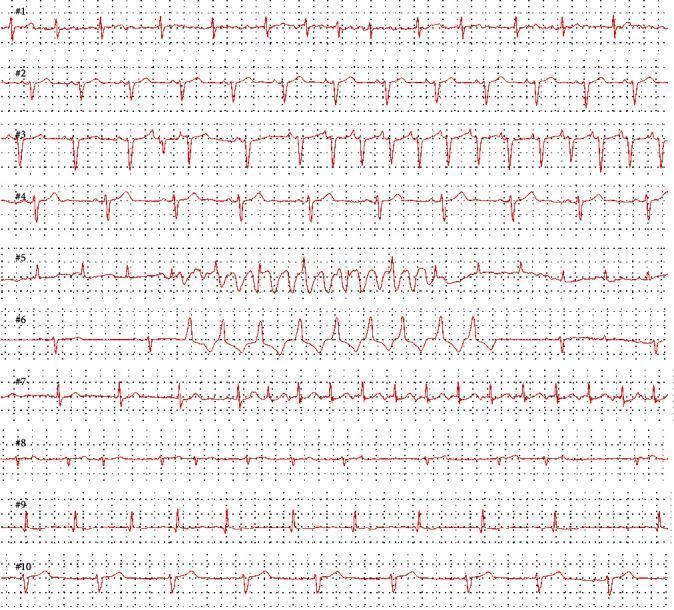
1. Bradyarrhythmias (Impaired Automaticity)
| Rhythm | Rate | P Wave | QRS | Key ECG Feature |
|---|---|---|---|---|
| Sinus bradycardia | < 60 bpm | Normal, upright in II | Narrow | Regular; widened R–R |
| Sinus arrest | < basic rate | Absent during pause | Absent during pause | Unpredictable pause; escape beat follows |
| SA exit block (Type II) | < basic rate | Absent (dropped cycle) | Absent | Pause = 2× or 3× P–P interval |
| Junctional escape | 40–60 bpm | Absent/retrograde | Narrow | Slow, regular; no preceding P wave |
| Idioventricular escape | 20–40 bpm | Dissociated | Wide (> 120 ms) | Very slow, wide QRS; AV dissociation |
2. Tachyarrhythmias
A. Supraventricular Tachycardias (SVT)
| Rhythm | Rate | P Wave | QRS | Key ECG Feature |
|---|---|---|---|---|
| Sinus tachycardia | 100–180 bpm | Normal, upright in II | Narrow | Gradual onset/offset; normal P axis |
| Focal atrial tachycardia (APT) | 150–250 bpm | Abnormal morphology; before QRS | Narrow | Long RP; AV block doesn't terminate it; warm-up/cool-down |
| Atrial flutter | 250–350 bpm (atrial) | Sawtooth flutter waves in II, III, aVF | Narrow | Regular 2:1 or 4:1 AV block; no isoelectric baseline |
| Atrial fibrillation | 350–600 bpm (atrial) | Absent; fibrillatory baseline (f waves) | Narrow | Irregularly irregular ventricular rate |
| AVNRT | 150–250 bpm | Within/just after QRS (pseudo-R' in V1) | Narrow | Short RP; abrupt onset/offset |
| AVRT (WPW) | 150–250 bpm | Retrograde, after QRS | Narrow (orthodromic) or wide (antidromic) | Delta wave in sinus; abrupt onset/offset |
B. Ventricular Arrhythmias
| Rhythm | Rate | P Wave | QRS | Key ECG Feature |
|---|---|---|---|---|
| Premature ventricular complex (PVC) | Underlying rate | Absent for PVC | Wide (> 120 ms), bizarre morphology | Early beat; full compensatory pause |
| Ventricular tachycardia (VT) | 100–250 bpm | AV dissociation | Wide (> 120 ms) | Monomorphic or polymorphic; fusion beats; capture beats |
| Ventricular fibrillation (VF) | > 300 bpm (chaotic) | Absent | No identifiable QRS | Chaotic, irregular undulations; no organized rhythm |
| Torsades de Pointes | 200–250 bpm | Absent | Wide; twisting QRS axis | Polymorphic VT with rotating amplitude around baseline; long QT precedes |
3. Conduction Disorders
| Rhythm | Rate | P Wave | QRS | Key ECG Feature |
|---|---|---|---|---|
| 1st-degree AV block | Normal | Normal | Normal | PR interval > 200 ms; all P waves conduct |
| 2nd-degree AV block — Mobitz I (Wenckebach) | Normal or slow | Normal | Normal | Progressive PR lengthening → dropped QRS |
| 2nd-degree AV block — Mobitz II | Normal or slow | Normal | May be wide | Sudden dropped QRS without PR prolongation |
| 3rd-degree (complete) AV block | Atrial: normal; Ventricular: 20–60 bpm | Normal, but no relation to QRS | Wide (ventricular escape) or narrow (junctional escape) | Complete AV dissociation; P and QRS independent |
| LBBB | Normal | Normal | Wide (> 120 ms); broad notched R in I, aVL, V5–V6; deep S in V1 | No septal Q in I, V5–V6 |
| RBBB | Normal | Normal | Wide (> 120 ms); RSR' (rabbit ears) in V1; wide S in I, V5–V6 | rSR' pattern in V1 |
ECG Reading Checklist for Any Arrhythmia
1. Rate → Atrial rate? Ventricular rate? Same or different?
2. Rhythm → Regular / irregular / irregularly irregular?
3. P waves → Present? Normal morphology? Relationship to QRS?
4. PR interval → Normal (120–200 ms)? Short? Long? Constant?
5. QRS width → Narrow (< 120 ms) = supraventricular
Wide (> 120 ms) = ventricular or aberrant SVT
6. QT interval → Prolonged? (risk of Torsades)
7. Axis → Normal / left / right deviation?
8. ST / T waves → Ischemia? Repolarization abnormality?
diagnostic criteria for an attack of atrial paroxysmal tachycardia
focal atrial tachycardia paroxysmal diagnostic criteria ECG P wave RP interval
atrial paroxysmal tachycardia ECG rhythm strip P wave morphology
Diagnostic Criteria for an Attack of Atrial Paroxysmal Tachycardia (APT)
Definition and Mechanism
Clinical Diagnostic Criteria
| Feature | Criterion |
|---|---|
| Onset / offset | Abrupt ("paroxysmal") start and termination |
| Symptoms | Palpitations, dyspnea, chest discomfort, lightheadedness; may be well-tolerated or cause hemodynamic compromise |
| Duration | Seconds to hours; recurrent episodes |
| Response to vagal maneuvers / adenosine | Transiently slows ventricular rate by increasing AV block — but does not terminate the tachycardia (atria continue at same rate) — distinguishing feature from AVNRT and AVRT |
ECG Diagnostic Criteria
12-Lead ECG — Paroxysmal SVT (Focal AT Pattern)
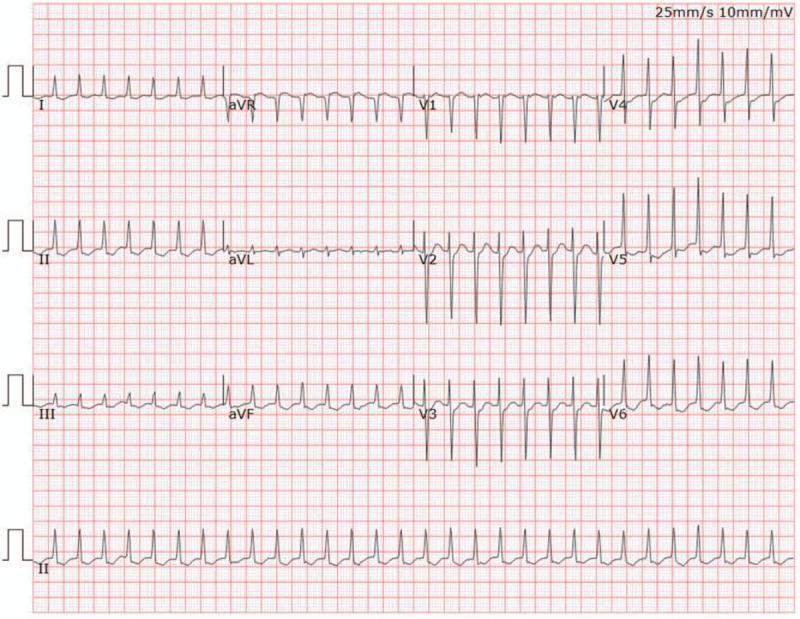
1. Rate
- Atrial rate 150–250 bpm (typically 150–200 bpm)
- Ventricular rate depends on AV conduction ratio (1:1 most common; 2:1 or Wenckebach block at faster rates)
2. Rhythm
- Regular (may be slightly irregular at onset — warm-up phenomenon)
3. P Wave — Most Diagnostically Important Feature
"It can be distinguished from sinus tachycardia by the P-wave morphology, which usually differs from sinus P waves depending on the location of the focus. Focal AT tends to originate in areas of complex atrial anatomy, such as the crista terminalis, valve annuli, atrial septum, and atrial muscle extending along cardiac thoracic veins."
| Focus Location | P Wave Appearance |
|---|---|
| High right atrium (near SA node) | Resembles sinus P wave; upright in II, III, aVF |
| Low right atrium | Negative/inverted in II, III, aVF (inferior activation) |
| Atrial septum | Narrower P wave duration than sinus; positive in V1 |
| Left atrium (free wall) | Monophasic positive P in V1; negative P in I and aVL (activation away from left atrial free wall) |
| Coronary sinus / pulmonary veins | Negative in inferior leads; positive in V1 |
4. RP / PR Relationship
- Long RP tachycardia: RP interval > PR interval (P wave falls well before the next QRS)
- PR interval shorter than RP interval — especially with rapid AV conduction from sympathetic tone (Harrison's, p. 7008)
- RP > 70 ms (P wave not buried within QRS — distinguishes from AVNRT)
5. QRS Complex
- Narrow (< 120 ms) — normal ventricular conduction
- Wide QRS possible with pre-existing bundle branch block or aberrant conduction — must differentiate from VT
6. AV Conduction Behavior
- 1:1 AV conduction at moderate rates; 2:1 or Wenckebach AV block at faster atrial rates
- AV block during tachycardia does NOT terminate it — the atria continue firing independently (hallmark distinguishing AT from AVNRT/AVRT where the AV node is part of the reentry circuit)
7. Warm-Up / Cool-Down Phenomenon
- Gradual acceleration at onset (first few beats slightly slower before reaching full rate)
- Gradual slowing at termination
- Indicates enhanced automaticity or triggered activity as the mechanism (absent in AVNRT/AVRT which start/stop abruptly)
Differential Diagnosis of SVT
| SVT Type | Rate | P Wave | RP Relationship | Response to Adenosine |
|---|---|---|---|---|
| Focal AT (APT) | 150–250 | Abnormal morphology; before QRS | Long RP (RP > PR) | AV block — tachycardia continues |
| AVNRT | 150–250 | Within or just after QRS (pseudo-R' in V1) | Short RP (RP < 70 ms) | Terminates |
| Orthodromic AVRT | 150–250 | Retrograde; after QRS | RP 70–150 ms | Terminates |
| Sinus tachycardia | 100–180 | Identical to sinus; upright in II | Long RP | Gradual slowing; resumes |
| Atrial flutter | 250–350 (atrial) | Sawtooth flutter waves; no isoelectric line | Fixed ratio block | Uncovers flutter waves; does not terminate |
Summary: Diagnostic Checklist for APT Attack
✔ Abrupt onset and offset (paroxysmal)
✔ Rate 150–250 bpm, regular
✔ P wave present, morphology differs from sinus
✔ Long RP pattern (RP > PR)
✔ Narrow QRS (< 120 ms)
✔ AV block with adenosine/vagal — tachycardia persists
✔ Warm-up at onset / cool-down at termination
✔ P wave axis localizes ectopic focus
Key Pearls
- The P wave morphology is the single most important ECG feature — it both confirms atrial origin and localizes the ectopic focus (Harrison's, p. 7008)
- Left atrial AT: positive monophasic P in V1 + negative P in I/aVL is a reliable localization pattern
- Septal AT: narrower-than-normal P wave duration is a subtle but useful clue
- Persistence of tachycardia despite AV block (spontaneous or induced) is the pathognomonic hallmark separating AT from all reentrant SVTs involving the AV node
- Incessant APT (> 10–15% of day) can cause tachycardia-induced cardiomyopathy — a reversible cause of dilated cardiomyopathy if detected and treated