Action and function of estrogen
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I have all the information needed for a comprehensive, well-structured answer. Here is the complete response:
Estrogen: Actions and Functions
Types of Estrogen
Three major naturally occurring estrogens exist:
| Estrogen | Source | Relative Potency |
|---|---|---|
| Estradiol (E2) | Ovary (principal form in premenopausal women) | Most potent |
| Estrone (E1) | Metabolite/precursor of estradiol; primary circulating form after menopause (from DHEA conversion in adipose tissue) | ~1/3 of estradiol |
| Estriol (E3) | Placenta (major estrogen during pregnancy) | Least potent |
- Lippincott Illustrated Reviews: Pharmacology, p. 832
Mechanism of Action
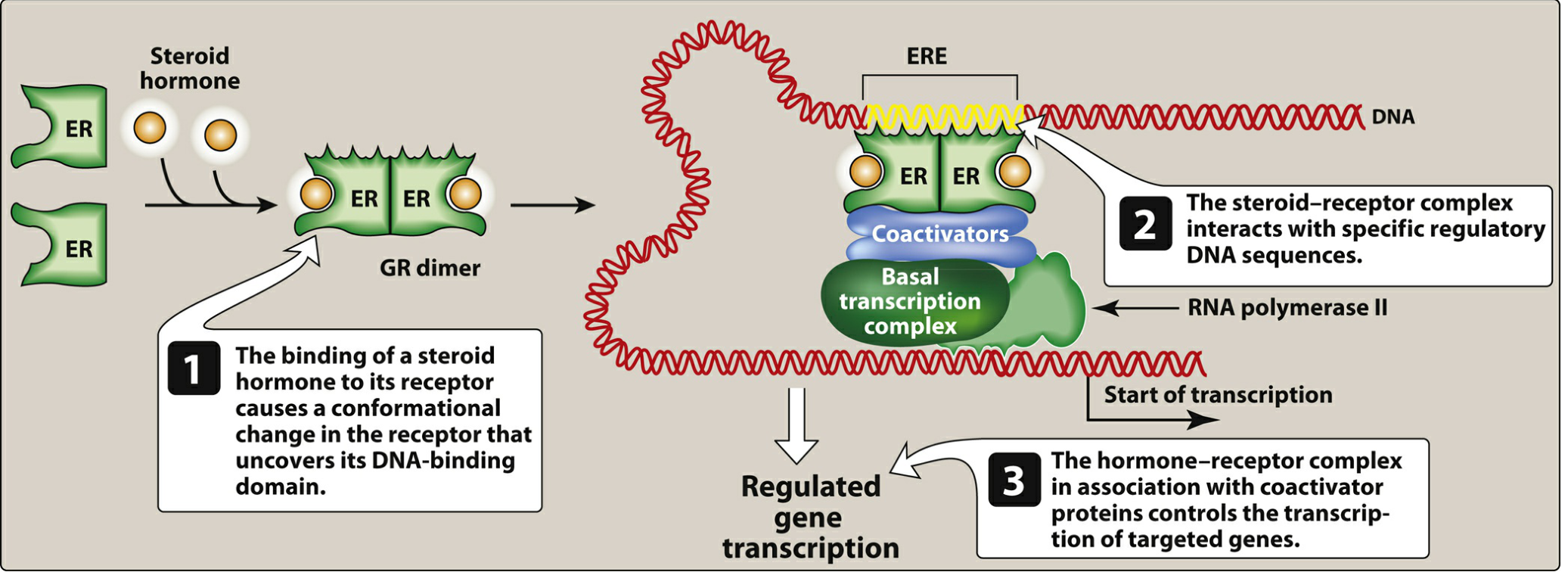
Estrogen acts primarily through a genomic (nuclear receptor) pathway:
- Free estradiol dissociates from sex hormone-binding globulin (SHBG) or albumin in plasma.
- It diffuses across the cell membrane and binds with high affinity to nuclear estrogen receptors (ERα or ERβ), which are inactive monomers bound to heat shock protein 90 (HSP90).
- Hormone binding causes a conformational change - HSPs dissociate, the receptor dimerizes (homodimers ERα/ERα, ERβ/ERβ, or ERα/ERβ heterodimers), and the dimer binds to estrogen response elements (EREs) on DNA.
- Together with coactivator proteins, the complex activates RNA polymerase II, initiating transcription of target genes and synthesis of specific proteins.
A non-genomic (rapid) pathway also exists via a G protein-coupled estrogen receptor (GPER/GPR30) at the membrane, producing faster effects not requiring gene transcription.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. [block13]
- Lippincott Illustrated Reviews: Pharmacology, p. 832
Estrogen Receptor Subtypes
| Receptor | Encoded by | Predominant Locations |
|---|---|---|
| ERα | ESR1 | Uterus, vagina, ovaries, mammary gland, hypothalamus, endothelium, vascular smooth muscle |
| ERβ | ESR2 | Prostate, ovaries, lung, brain, bone |
Both receptors can form homo- or heterodimers. ERβ, when co-expressed with ERα, often inhibits ERα-mediated transcriptional activation - this has implications in breast cancer biology.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Physiological Actions of Estrogen
1. Female Reproductive Tract
- Maturation and maintenance of the uterus, fallopian tubes, cervix, and vagina.
- In the uterus: causes cell proliferation, cell growth, and increased contractility; stimulates growth of the endometrium, glands, stroma, and spiral arteries during the follicular (proliferative) phase.
- In the cervix: makes mucus copious, watery, and elastic ("ferning" pattern on glass slide), allowing sperm penetration.
- In the fallopian tubes: stimulates ciliary activity and contractility to aid sperm transport.
- In the vagina: stimulates epithelial cell proliferation.
2. Secondary Sexual Characteristics at Puberty
- Responsible for development of female secondary sex characteristics: growth of the uterus, vagina, labia, pubic/axillary hair distribution, female fat distribution (hips/thighs/buttocks), and female body contour.
3. Breast Development
- Required for development of the breasts; stimulates ductal and stromal growth, fat deposition.
- Works in coordination with progesterone and prolactin for full lactation capability.
4. Hypothalamic-Pituitary Feedback
- Negative feedback during most of the follicular phase: suppresses GnRH (hypothalamus) and FSH/LH (anterior pituitary).
- Positive feedback at midcycle: when estradiol levels rise above ~200 pg/mL, it up-regulates GnRH receptors on the anterior pituitary and causes the LH/FSH surge, triggering ovulation.
- Up-regulates progesterone receptors in target tissues, preparing them to respond to progesterone (the follicular phase "primes" the luteal phase).
5. Bone
-
Reduces bone resorption by decreasing the bone-resorbing action of PTH.
-
Estrogen receptors are present on bone cells; estrogen has direct effects on bone remodeling.
-
Deficiency (as at menopause) leads to accelerated bone loss and osteoporosis.
-
Men with aromatase deficiency or absent ER show osteopenia and failure of epiphyseal closure, confirming estrogen's role in bone in both sexes.
-
Katzung's Basic and Clinical Pharmacology, 16th Edition
6. Cardiovascular Effects
- Increases HDL cholesterol, decreases LDL cholesterol (favorable lipid profile).
- Direct effects on vascular endothelium and smooth muscle.
- Note: The Women's Health Initiative demonstrated that hormone replacement therapy (HRT) significantly increases risks of heart disease and breast cancer; HRT is now reserved for short-term relief of vasomotor symptoms.
7. Skin and Connective Tissue
- Maintains skin thickness and collagen content; estrogen deficiency after menopause accelerates collagen loss.
8. CNS Effects
- Higher estrogen levels transiently increase CNS sensitivity to serotonin.
- Sexual dimorphisms in brain function partially reflect acute and reversible actions of sex steroid concentrations.
- Involved in thermoregulation - estrogen withdrawal leads to vasomotor instability ("hot flashes").
9. Metabolic Effects
- Increases hepatic production of sex hormone-binding globulin (SHBG), coagulation factors, and vitamin D-binding protein (DBP).
- Increases 1,25(OH)₂D levels in vivo (indirect effect via changes in PTH, calcium, and phosphate).
Summary Table: Actions of Estrogen on Target Tissues
| System | Key Actions |
|---|---|
| Uterus | Proliferation of endometrium, increased contractility, spiral artery growth |
| Cervix | Watery, elastic, "ferning" mucus |
| Vagina | Epithelial proliferation |
| Fallopian tubes | Ciliary activity, motility |
| Breast | Ductal development, fat deposition |
| Bone | Inhibits resorption, maintains density, epiphyseal closure |
| HPG axis | Negative feedback (usually), positive feedback at midcycle (LH surge) |
| Cardiovascular | ↑HDL, ↓LDL, vascular effects |
| CNS | ↑Serotonin sensitivity, thermoregulation |
| Liver | ↑SHBG, coagulation factors, DBP |
| Adipose | Fat distribution to female pattern |
- Costanzo Physiology, 7th Edition, Table 10.2
Therapeutic Uses
- Contraception - combined with a progestogen (oral, transdermal, vaginal).
- Menopausal hormone therapy - vasomotor symptoms, urogenital atrophy (short-term use preferred due to risks).
- Osteoporosis prevention - established efficacy, though now largely superseded by bisphosphonates and SERMs due to adverse effects.
Selective Estrogen Receptor Modulators (SERMs) (e.g., raloxifene, tamoxifen) were developed to capture bone/cardiovascular benefits while minimizing risks at breast and uterus - exploiting tissue-specific differences in ERα and ERβ expression.
- Lippincott Illustrated Reviews: Pharmacology, p. 832-833
- Katzung's Basic and Clinical Pharmacology, 16th Edition
This is a shared conversation. Sign in to Orris to start your own chat.