I am a resident doctor teach me ecg from basic and how can i become expert in it
Reading File
Finding Sources
Finding Sources
Searching the Web
how to learn ECG interpretation systematically resident doctor guide 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent — I now have all the textbook material, images, and data I need to deliver a comprehensive ECG teaching guide. Let me compile it.
📖 ECG from Basics to Expertise — A Complete Resident's Guide
Based on Ganong's Review of Medical Physiology (26th ed.), Braunwald's Heart Disease, Tintinalli's Emergency Medicine, and the Harriet Lane Handbook.
PART 1: WHY THE ECG LOOKS THE WAY IT DOES
The Conduction System (Start Here)
Before reading a single trace, understand what generates the signal.
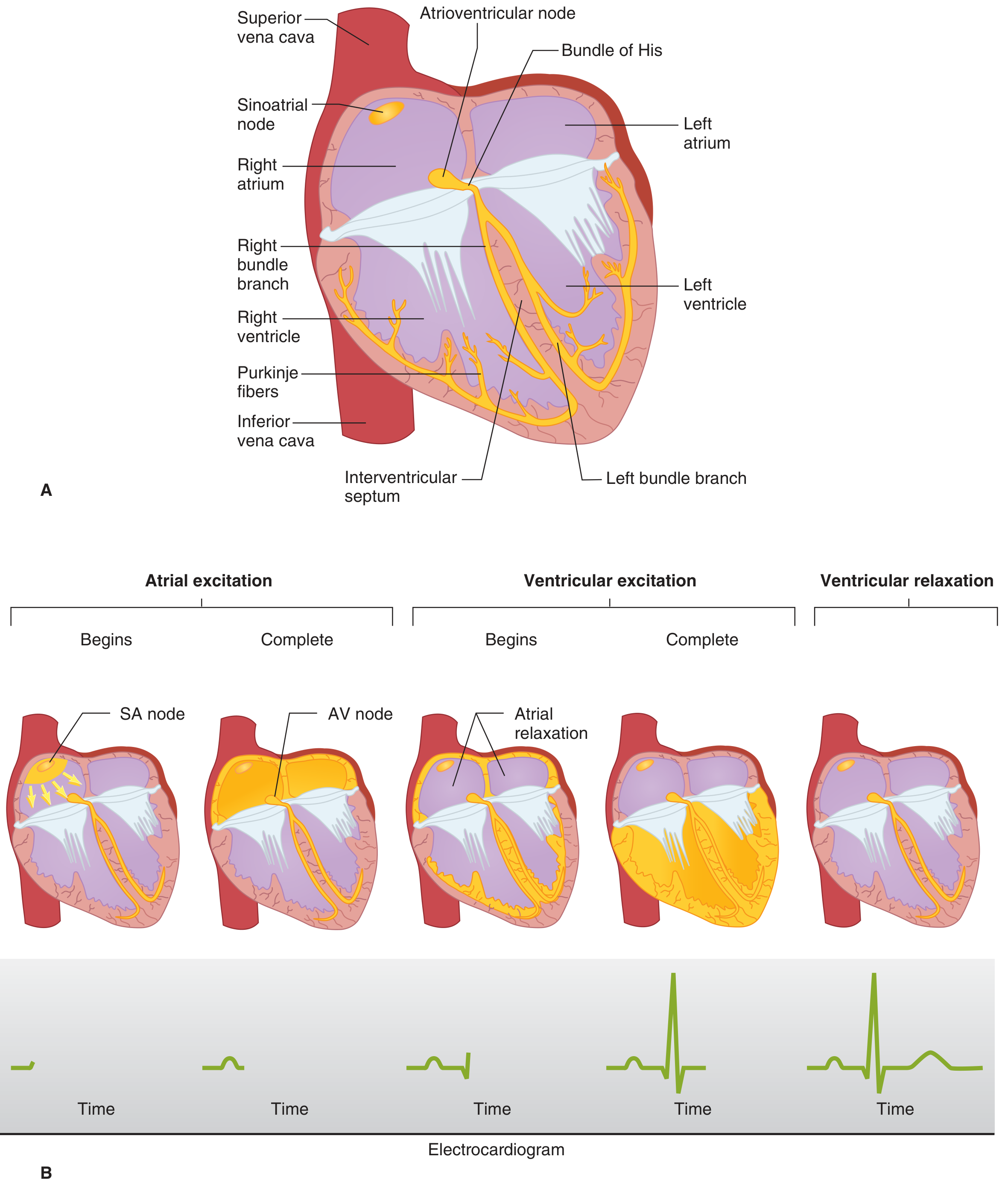
Normal spread of cardiac excitation (Ganong's Review of Medical Physiology, 26th ed.)
The impulse travels in this order:
| Structure | Conduction Speed | Clinical Relevance |
|---|---|---|
| SA node | 0.05 m/s | Slowest — pacemaker |
| Atrial pathways | 1 m/s | P wave |
| AV node | 0.05 m/s | Deliberate delay (~0.1 s) = PR segment |
| Bundle of His | 1 m/s | |
| Purkinje fibers | 4 m/s | Fastest — rapid ventricular activation |
| Ventricular muscle | 1 m/s | QRS complex |
Key concept: Depolarization moving toward an electrode → positive (upward) deflection. Moving away → negative (downward) deflection.
PART 2: THE ECG PAPER & RECORDING BASICS
- Paper speed: 25 mm/s
- 1 small square = 1 mm = 0.04 s
- 1 large square = 5 mm = 0.20 s
- Amplitude standard: 10 mm = 1 mV
The 12 Leads
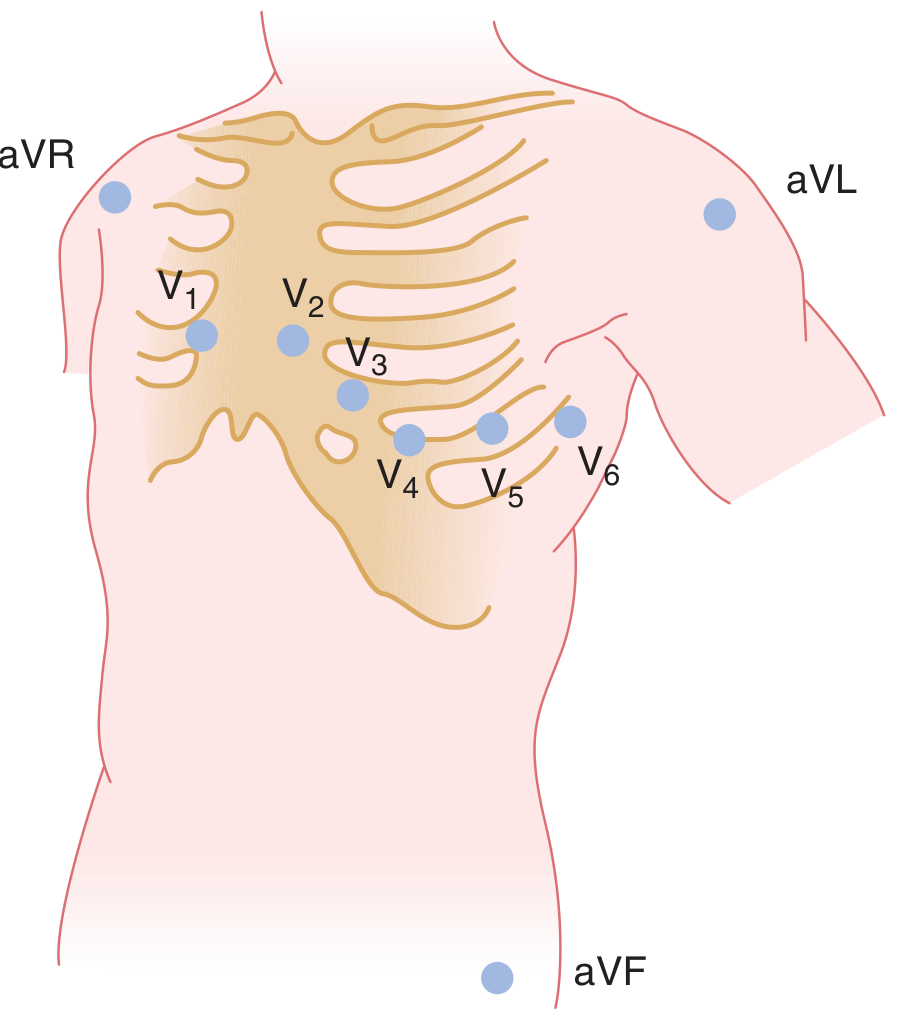
Lead placement (Ganong's, 26th ed.)
Limb leads (frontal plane):
- Bipolar: I (RA→LA), II (RA→LL), III (LA→LL)
- Augmented unipolar: aVR (right arm), aVL (left arm), aVF (left foot)
Precordial leads (horizontal plane):
- V1: Right sternal border, 4th ICS
- V2: Left sternal border, 4th ICS
- V3: Between V2 and V4
- V4: Left midclavicular line, 5th ICS
- V5: Left anterior axillary line
- V6: Left midaxillary line
Grouping leads by territory:
| Territory | Leads | Artery |
|---|---|---|
| Inferior | II, III, aVF | RCA (80%) |
| Lateral | I, aVL, V5, V6 | LCx |
| Anterior | V1–V4 | LAD |
| Septal | V1, V2 | LAD septal branches |
| Posterior | V7–V9 (or reciprocal in V1–V2) | RCA/LCx |
PART 3: THE WAVES, INTERVALS & SEGMENTS
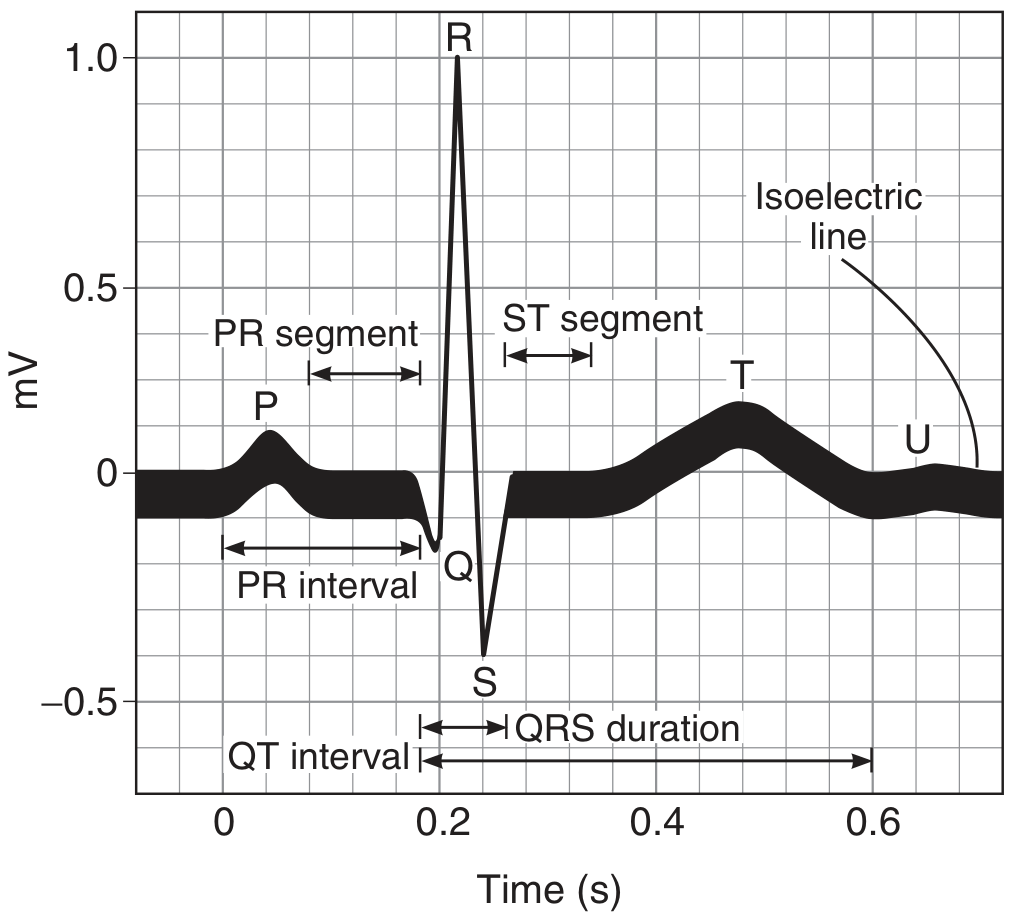
Standard ECG waves and intervals (Ganong's Review of Medical Physiology, 26th ed.)
Normal Values (Adults)
| Component | What It Represents | Normal Value |
|---|---|---|
| P wave | Atrial depolarization | Duration < 0.12 s, amplitude < 2.5 mm |
| PR interval | AV conduction time | 0.12–0.20 s (3–5 small squares) |
| QRS complex | Ventricular depolarization | < 0.12 s (< 3 small squares) |
| ST segment | Ventricular plateau phase | Isoelectric (±1 mm) |
| T wave | Ventricular repolarization | Same direction as QRS in most leads |
| QT interval | Total ventricular activity | < 0.44 s (men), < 0.46 s (women) |
| U wave | Possibly Purkinje/M-cell repolarization | Small, same direction as T wave |
QTc (Corrected QT)
Use Bazett's formula: QTc = QT / √RR
PART 4: A SYSTEMATIC 8-STEP APPROACH (Never Skip)
Train yourself to follow these in every single ECG — the discipline is what makes you expert.
Step 1: Rate
Quick method: 300 ÷ number of large boxes between two R waves
- 1 box = 300 bpm | 2 = 150 | 3 = 100 | 4 = 75 | 5 = 60 | 6 = 50
For irregular rhythms: Count QRS complexes in a 10-second strip × 6
Step 2: Rhythm
Ask three questions:
- Is there a P wave before every QRS?
- Is the P wave upright in leads I and aVF? (= sinus origin)
- Is the RR interval regular?
→ Sinus rhythm = upright P in I and aVF, P before every QRS, regular rate 60–100
Step 3: Axis
Use leads I and aVF:
| Lead I | aVF | Axis |
|---|---|---|
| ↑ (positive) | ↑ (positive) | Normal (0° to +90°) |
| ↑ (positive) | ↓ (negative) | Left axis deviation (> -30°: pathologic LAD) |
| ↓ (negative) | ↑ (positive) | Right axis deviation |
| ↓ (negative) | ↓ (negative) | Extreme/indeterminate axis |
Causes of LAD: LBBB, left anterior fascicular block, inferior MI, WPW (right-sided pathway)
Causes of RAD: RVH, RBBB, left posterior fascicular block, lateral MI, PE, normal in children
Step 4: P Wave
- Broad, notched P in lead II (P mitrale, > 0.12 s) → Left atrial enlargement
- Tall, peaked P in lead II (P pulmonale, > 2.5 mm) → Right atrial enlargement
- No visible P waves → Atrial fibrillation/flutter/junctional rhythm
Step 5: PR Interval
| Interval | Interpretation |
|---|---|
| < 0.12 s | Pre-excitation (WPW), junctional rhythm |
| 0.12–0.20 s | Normal |
| > 0.20 s | 1st degree AV block |
| Progressive lengthening then dropped QRS | Mobitz type I (Wenckebach) |
| Fixed PR + randomly dropped QRS | Mobitz type II |
| P and QRS completely dissociated | 3rd degree (complete) AV block |
Step 6: QRS Complex
- Width > 0.12 s = bundle branch block or ventricular rhythm
- RBBB pattern (RSR' in V1, slurred S in I and V6): RV depolarizes last via slow muscle spread
- LBBB pattern (broad notched R in I, V5, V6; QS in V1): LV depolarizes last — invalidates ischemia interpretation
- Q waves: Pathologic if > 0.04 s wide OR > 25% of R wave height in the same lead → old MI
- R wave progression: R should grow from V1→V5. Poor R wave progression → anterior MI
Step 7: ST Segment & T Wave
This is where life-threatening diagnoses live.
| Finding | Cause |
|---|---|
| ST elevation (> 1 mm limb leads, > 2 mm precordial) | STEMI, Brugada, early repolarization, pericarditis, LBBB |
| ST depression | NSTEMI, ischemia, digoxin effect, posterior MI (V1–V2) |
| Diffuse concave ST elevation + PR depression | Pericarditis |
| T wave inversion | Ischemia, PE (V1–V4 = right heart strain), hypertrophy, RBBB/LBBB |
| Peaked tall T waves | Hyperkalemia (earliest sign), hyperacute STEMI |
| Flat/inverted T waves in V1–V4 | RV strain (think PE) |
STEMI localization:
| Leads with STE | Territory | Culprit |
|---|---|---|
| II, III, aVF | Inferior | RCA |
| I, aVL, V5–V6 | Lateral | LCx |
| V1–V4 | Anterior | LAD |
| V1–V2 ST depression + tall R in V1 | Posterior | RCA/LCx |
Step 8: QT Interval & Other Findings
- Prolonged QT: Risk of torsades de pointes. Causes: drugs (antipsychotics, antiarrhythmics, antibiotics), hypokalemia, hypomagnesemia, hypocalcemia, congenital LQTS
- Short QT: Hypercalcemia, digoxin, short QT syndrome
- Delta wave (slurred QRS upstroke): Wolff-Parkinson-White syndrome
PART 5: COMMON ECG PATTERNS YOU MUST MASTER
Atrial Fibrillation
- Irregularly irregular RR intervals
- No distinct P waves — chaotic baseline
- Narrow QRS (unless aberrant conduction or pre-existing BBB)
Atrial Flutter
- Sawtooth flutter waves at ~300 bpm, typically 2:1 or 4:1 conduction
- Ventricular rate 150 bpm (2:1) or 75 bpm (4:1)
- Best seen in II, III, aVF
SVT (Narrow Complex Tachycardia)
- Rate 150–250 bpm, regular
- P waves often buried in QRS or retrograde
- Responds to adenosine (also diagnostic)
Ventricular Tachycardia (VT)
- Wide QRS (> 0.12 s), rate > 100 bpm
- AV dissociation = diagnostic
- Fusion beats and capture beats = pathognomonic
- Brugada criteria / Vereckei algorithm: helps distinguish VT from SVT with aberrancy
Hyperkalemia — Progressive Changes
- Peaked T waves (K > 5.5)
- Widened QRS (K > 6.5)
- Flattened/absent P waves (K > 7)
- Sine wave pattern → VF
Pulmonary Embolism — S1Q3T3
- S wave in lead I
- Q wave in lead III
- T wave inversion in lead III
- Sinus tachycardia (most common finding)
- Rightward axis, RBBB, T inversion V1–V4 (right heart strain)
Pericarditis
- Diffuse concave ("saddle-shaped") ST elevation in almost all leads
- PR depression (especially lead II) — very specific sign
- No reciprocal changes (unlike MI)
Left Ventricular Hypertrophy (Sokolow-Lyon criteria)
- S in V1 + R in V5 or V6 > 35 mm
- R in aVL > 11 mm
- Associated with ST depression and T wave inversion ("strain pattern") in lateral leads
PART 6: KEY DIAGNOSES FROM BRAUNWALD'S — CLINICAL ECG UTILITY
From Braunwald's Heart Disease: The ECG provides a class I recommendation in evaluating syncope. Specific diagnostic ECG findings include:
- QT prolongation → Long-QT syndrome
- Short PR + delta wave → Wolff-Parkinson-White syndrome
- RBBB + ST elevation in V1–V2 → Brugada syndrome
- T wave inversion in right precordial leads → Arrhythmogenic RV dysplasia (ARVC)
- High-grade AV block → Stokes-Adams attacks
From Tintinalli's Emergency Medicine: In chest pain — obtain a 12-lead ECG rapidly and compare to prior tracings. Dynamic ECG changes (new ST shifts or T-wave changes) in the setting of symptoms have 84% CAD prevalence with classic anginal symptoms.
PART 7: HOW TO BECOME AN EXPERT — ROADMAP
Phase 1 — Build the Foundation (Months 1–2)
- Memorize the 8-step systematic approach — apply it to every ECG you touch, even if it looks "obviously normal"
- Read: ECG Made Easy by Akhtar & Hampton — short, practical primer
- Ganong's physiology chapter on cardiac electrophysiology — understand WHY waveforms form
- Practice 5–10 ECGs daily on ECGWaves.com or Life in the Fast Lane ECG Library
Phase 2 — Pattern Recognition (Months 3–4)
- Master the STEMI mimics: early repolarization, LVH, LBBB, pericarditis, hyperkalemia, Brugada
- Learn Sgarbossa criteria for STEMI in LBBB/paced rhythms (modified: concordant STE ≥ 1 mm, or discordant STE ≥ 25% of S-wave depth)
- Use Dr. Smith's ECG Blog (https://hqmeded-ecg.blogspot.com) — expert commentary on real, difficult cases daily
Phase 3 — Advanced Interpretation (Months 5–8)
- Study Wellens' syndrome (biphasic/deep T inversion in V2–V3 = proximal LAD critical stenosis — do NOT stress test)
- Learn de Winter T waves (upsloping ST depression + tall T in precordial leads = LAD occlusion with no STE)
- Master AV block grades, fascicular blocks, and bifascicular/trifascicular block
- Attend a dedicated advanced ECG workshop (EP fellows often run these)
Phase 4 — Expert (Month 9+)
- Correlate every ECG with clinical outcome — build mental case libraries
- Read Marriott's Practical Electrocardiography or Chou's Electrocardiography in Clinical Practice
- Present ECGs at cardiology conferences / morbidity & mortality rounds
- Learn to interpret electrophysiology tracings in the cath lab context
Daily Habits of Expert ECG Readers
- Always read the ECG before looking at the computer interpretation (machines are wrong ~30% of the time)
- Commit to a written systematic interpretation — don't just glance
- Compare with prior ECGs — dynamic change is often more important than any single finding
- When in doubt: call cardiology; ECG misinterpretation in AMI is a major medicolegal issue
PART 8: QUICK REFERENCE CARD
| Interval | Normal | Prolonged → |
|---|---|---|
| PR | 0.12–0.20 s | AV block, > 0.20 s |
| QRS | < 0.12 s | BBB, hyperkalemia, VT |
| QTc | < 0.44 s (M), < 0.46 s (F) | Torsades risk |
| P wave duration | < 0.12 s | LAE |
| P wave amplitude | < 2.5 mm | RAE if ≥ 2.5 mm |
| Rate calculation | Boxes between R waves |
|---|---|
| 300 bpm | 1 box |
| 150 bpm | 2 boxes |
| 100 bpm | 3 boxes |
| 75 bpm | 4 boxes |
| 60 bpm | 5 boxes |
| 50 bpm | 6 boxes |
Sources:
- Ganong's Review of Medical Physiology, 26th ed. — Chapters 29 (cardiac electrophysiology, ECG basics)
- Braunwald's Heart Disease, 2-Volume Set — Chapter 71 (syncope workup and ECG role)
- Tintinalli's Emergency Medicine — Chapters 49, 51 (ACS, chest pain ECG interpretation)
- Harriet Lane Handbook, 23rd ed. — Chapter 7 (systematic ECG approach, normal parameters table)
The single most important habit: read every ECG systematically, every time — no shortcuts. That discipline, applied to thousands of traces over your residency, is what builds genuine expertise.
In aki patient how much infusion can we give in a day and how much fluid consumption through mouth can be given
Reading File
Finding Sources
Finding Sources
Searching the Web
AKI acute kidney injury daily fluid allowance IV infusion oral intake guidelines
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://www.ajkd.org/article/S0272-63861731141-1/fulltext
Finding Sources
Reading File
Searching PubMed
"acute kidney injury" AND "fluid management" AND "fluid restriction"
I now have excellent data from Brenner & Rector's The Kidney and Goldman-Cecil Medicine. Let me compile the complete, authoritative answer.
Fluid Management in AKI: IV Infusion + Oral Intake
This is one of the most practically important questions in nephrology ward work. The answer depends critically on whether the AKI is pre-renal/volume-depleted vs. established/oliguric/volume-overloaded. These two states require opposite approaches.
The Core Principle: Match Output + Replace Losses
The universal formula for fluid allowance in established AKI is:
Total daily fluid allowed = Previous day's urine output + Insensible losses (400–500 mL/day)
This covers both IV infusions AND oral intake combined.
| Loss Type | Amount |
|---|---|
| Insensible losses (skin + lungs) | ~400–500 mL/day (afebrile, atraumatic) |
| Extra per °C fever above 37°C | + 100–150 mL per degree |
| Extra for diarrhea/vomiting/drains | Add measured losses |
| Urine output (previous 24 hours) | Replace mL for mL |
Example: A patient made 300 mL urine in the last 24 hours, is afebrile, no abnormal losses:
- Total fluid budget = 300 + 500 = 800 mL/day (IV + oral combined)
Phase-Specific Management
Phase 1: Pre-renal AKI / Volume Depletion (Give Fluid Liberally)
If the patient is hypovolemic (dry mucous membranes, low JVP, hypotension, rising creatinine after vomiting/diarrhea/bleeding):
- Give IV fluid resuscitation to restore perfusion
- Use balanced crystalloids (Ringer's lactate / Plasma-Lyte) rather than normal saline
- Why? Normal saline (0.9% NaCl) contains 154 mmol/L chloride - supraphysiologic. Chloride-rich solutions cause renal vasoconstriction, worsen renal medullary hypoxia, and increase AKI risk vs. balanced solutions
- Avoid hydroxyethyl starch - associated with >2x increased AKI risk in RCTs
- Volume: 250–500 mL boluses titrated to clinical response (urine output, BP, JVP)
- No fixed daily limit in this phase - keep giving until euvolemic
Phase 2: Established AKI / Oliguric / Volume Overloaded (Restrict Fluid)
From Brenner & Rector's The Kidney (Table 29.7 - Supportive Management of AKI):
| Problem | Fluid Management |
|---|---|
| Intravascular volume overload | Restrict salt (< 1–2 g/day) and water (< 1 L/day) intake; diuretics if non-oliguric; ultrafiltration if refractory |
| Hyponatremia | Restrict oral AND IV free water |
So for an oliguric, volume-overloaded AKI patient: total fluid (IV + oral) is capped at approximately < 1 L/day beyond insensible replacement.
Practical Breakdown: IV vs. Oral
There is no separate fixed limit for IV vs. oral - they share the same daily budget. Here's how to split it practically:
In a typical oliguric AKI patient (urine output ~200–400 mL/day):
| Source | Approximate Volume |
|---|---|
| Oral intake (food + drink) | 500–600 mL |
| IV medications/infusions (antibiotics, drips) | Count every mL - flush volumes, drug diluents, TPN |
| Dedicated IV fluid (maintenance) | Only if oral route unavailable or patient is nil by mouth |
| Total (IV + oral) target | Previous UO + 400–500 mL insensible |
Key practical points:
- Count ALL sources - IV drug flushes, NG feeds, oral medications dissolved in water, ice chips all count
- If patient is on IV drips (antibiotics, vasopressors, etc.) and these already consume most of the budget - oral intake must be reduced accordingly
- If patient is dialysis-requiring AKI - fluid restriction can be somewhat relaxed as fluid removal is managed during sessions, but interdialytic weight gain should be kept to < 1–1.5 kg between sessions
Non-Oliguric AKI (Urine Output > 400 mL/day)
- Fluid management is less restrictive
- May use loop diuretics (furosemide 40–80 mg IV) to offload excess volume
- Can match input more freely to output
- Still avoid fluid overload - associated with independently increased mortality in AKI
Fluid Overload in AKI: Why Strict Restriction Matters
From Brenner & Rector's The Kidney: Fluid excess in AKI is independently associated with:
- Increased risk of new sepsis
- Intra-abdominal hypertension (IAP > 12 mmHg) → compresses renal veins → worsens AKI further
- Abdominal compartment syndrome (IAP > 20 mmHg + organ dysfunction)
- Increased short- and long-term mortality
This is why the textbook recommendation is firm: < 1 L/day total water intake in volume-overloaded AKI.
When to Start Dialysis (RRT)
If fluid restriction alone is failing and the patient develops:
- Refractory volume overload / pulmonary edema
- Hyperkalemia unresponsive to medical management
- Severe metabolic acidosis (HCO3 < 15)
- Uremic symptoms (encephalopathy, pericarditis, myoclonus)
→ Initiate RRT. At this point, fluid intake targets are co-managed with dialysis team.
Quick Reference Card
| AKI State | Daily Total Fluid (IV + Oral) |
|---|---|
| Pre-renal / hypovolemic | Resuscitate freely with balanced crystalloids until euvolemic |
| Oliguric established AKI | Previous day UO + 400–500 mL = total budget |
| Volume-overloaded AKI | < 1 L/day total; loop diuretic or RRT |
| Non-oliguric AKI | Previous day UO + 500 mL; diuretics to offload if needed |
| Dialysis-dependent AKI | < 1–1.5 kg interdialytic weight gain; co-manage with nephrology |
Salt restriction: < 1–2 g sodium/day in all established AKI with volume overload.
Sources:
- Brenner & Rector's The Kidney, 2-Volume Set — Table 29.7 (Supportive Management of AKI); Section: Fluid Management and Its Impact on AKI
- Goldman-Cecil Medicine, International Edition — Chapter 106 (AKI: Fluids and Supportive Care)
- KDIGO 2012 AKI Clinical Practice Guidelines (fluid chapters)
Open type 2 b contaminated combinated fracture of left ulna lower 4th
Reading File
Finding Sources
Finding Sources
Searching the Web
Gustilo Anderson type 2 open fracture management contaminated antibiotic debridement fixation
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.