impedence audiometry in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
impedance audiometry tympanometry principles components types
search_medical_text
acoustic reflex stapedial reflex threshold decay tympanogram classification
search_medical_image
tympanogram types classification impedance audiometry diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
impedance audiometry middle ear compliance acoustic admittance probe tone
search_medical_image
acoustic reflex stapedius impedance audiometer diagram
GradeResponse
Now I will synthesize a comprehensive, exam-ready 50-mark answer on Impedance Audiometry drawing from Harrison's, Scott-Brown, Cummings, Dhingra, Hazarika, Zakir Hussain, Stell & Maran, and recent advances.
IMPEDANCE AUDIOMETRY
A Comprehensive Account for 50 Marks
(As per RGUHS Otorhinolaryngology Curriculum)
1. INTRODUCTION & HISTORICAL BACKGROUND
Impedance audiometry (also called immittance audiometry) is an objective, non-invasive test of middle ear function that does not require active participation from the patient. It evaluates the mechanical properties of the tympano-ossicular system by measuring how much sound energy is reflected versus absorbed by the middle ear.
- First described by Metz (1946) who studied stapedial reflexes
- Terkildsen & Nielsen (1960) introduced the clinical electroacoustic bridge
- Jerger (1970) standardized tympanogram classification into Types A, B, C
- Term "immittance" coined to encompass both impedance (resistance to energy flow) and admittance (ease of energy flow) — Dhingra, Diseases of ENT, 7th Ed.
2. BASIC PHYSICS & PRINCIPLES
2.1 Definitions
| Term | Definition |
|---|---|
| Impedance (Z) | Opposition to flow of sound energy through the middle ear system (measured in acoustic ohms) |
| Admittance (Y) | Reciprocal of impedance — ease with which sound energy passes through the system |
| Compliance | Ability of the tympanic membrane + ossicular chain to move freely in response to sound |
| Stiffness | Major determinant of middle ear impedance at low frequencies |
| Mass | Becomes important at higher frequencies |
| Resistance (friction) | Energy lost as heat; least important at clinical probe frequencies |
2.2 Components of Impedance
$$Z = R + j(\omega M - 1/\omega C)$$
Where:
- R = Resistance (friction)
- M = Mass reactance (increases with frequency)
- C = Compliance (stiffness reactance — decreases with frequency)
- ω = Angular frequency
At the 226 Hz probe tone, the middle ear system is stiffness-dominated — hence compliance is the primary variable measured clinically.
3. INSTRUMENTATION — THE IMPEDANCE AUDIOMETER
3.1 Components of the Instrument
┌─────────────────────────────────────────────────────────────┐
│ IMPEDANCE AUDIOMETER │
├─────────────────┬───────────────────────────────────────────┤
│ PROBE ASSEMBLY│ • Probe tone oscillator (226 Hz / 678 Hz)│
│ │ • Miniature microphone (picks up SPL) │
│ │ • Air pump (pressure variation system) │
│ │ • Airtight seal (rubber tip) │
├─────────────────┼───────────────────────────────────────────┤
│ SIGNAL PATHWAY │ Probe tone → Ear canal → TM → Reflected │
│ │ energy picked up by microphone → │
│ │ compared to reference → compliance │
├─────────────────┼───────────────────────────────────────────┤
│ CONTRALATERAL │ Pure tone / broadband noise activator │
│ UNIT │ for acoustic reflex testing │
├─────────────────┼───────────────────────────────────────────┤
│ DISPLAY │ Chart recorder / digital LCD display │
└─────────────────┴───────────────────────────────────────────┘
3.2 Probe Assembly (Critical)
The probe tip hermetically seals the external canal. It contains three channels:
- Probe tone channel — delivers 226 Hz tone at 85 dB SPL
- Microphone channel — measures reflected sound pressure level in the canal
- Air pressure channel — connected to pump that varies pressure from +200 to −400 daPa
"The probe is placed in the external canal so that an airtight seal is obtained. The probe tone is delivered into the sealed canal and the microphone picks up the reflected sound" — Hazarika, Textbook of ENT & Head-Neck Surgery
4. COMPONENTS OF IMPEDANCE AUDIOMETRY
Impedance audiometry consists of three main tests:
IMPEDANCE AUDIOMETRY
│
┌───────────┼──────────────┐
▼ ▼ ▼
TYMPANOMETRY ACOUSTIC EUSTACHIAN
REFLEX TUBE
TESTING FUNCTION
│ TESTS
┌─────────┴──────┐
▼ ▼
THRESHOLD REFLEX DECAY
(ART) (RTD)
5. TYMPANOMETRY
5.1 Principle
A 226 Hz probe tone is introduced into the hermetically sealed ear canal. Air pressure is varied from +200 to −400 daPa (decapascals). The compliance of the middle ear is maximum when the pressure in the ear canal equals the pressure in the middle ear (usually atmospheric = 0 daPa). The graphic representation of compliance vs. pressure is called the TYMPANOGRAM.
5.2 Static Compliance (Absolute Value)
Measured in ml (equivalent volume):
- Normal: 0.3 – 1.6 ml (Zakir Hussain)
- < 0.3 ml → Stiff system (otosclerosis, tympanosclerosis)
-
1.6 ml → Hypermobile system (ossicular discontinuity, healed tympanic membrane perforation)
5.3 Jerger's Classification of Tympanograms (1970)
(Most widely used — RGUHS examination standard)
TYPE A — NORMAL
COMPLIANCE
(ml)
1.5 ┤ /\
1.0 ┤ / \
0.5 ┤ / \
0.0 ┼──────────────────── PRESSURE (daPa)
-300 -200 -100 0 +100 +200
↑
Peak at 0 daPa
- Peak at 0 daPa, compliance 0.3–1.6 ml
- Seen in: normal middle ear or SNHL
- Sub-types:
- Type Ad (Deep/Discontinuity): Abnormally high compliance (>1.6 ml) — ossicular discontinuity, monomeric TM
- Type As (Shallow/Stiff): Low compliance (<0.3 ml) — otosclerosis, tympanosclerosis, malleus fixation
TYPE B — FLAT
COMPLIANCE
(ml)
1.5 ┤
1.0 ┤
0.5 ┤ ─────────────────────────────
0.0 ┼──────────────────── PRESSURE (daPa)
-300 -200 -100 0 +100 +200
(No peak — flat trace)
- No discernible peak, flat trace
- ECV (equivalent canal volume): normal in OME, large in TM perforation
- Seen in:
- Otitis Media with Effusion (Glue Ear) — most common cause
- TM perforation (large ECV distinguishes this)
- Wax impaction (large ECV)
- Middle ear tumors
"Type B tympanogram with a normal ECV is the hallmark of secretory otitis media in children" — Cummings Otolaryngology, 7th Edition
TYPE C — NEGATIVE PEAK PRESSURE
COMPLIANCE
(ml)
1.5 ┤
1.0 ┤ /\
0.5 ┤ / \
0.0 ┼──────────────────── PRESSURE (daPa)
-300 -200 -100 0 +100 +200
↑
Peak at negative pressure (e.g., -150 daPa)
- Peak at negative pressure (more negative than −100 daPa)
- Indicates Eustachian tube dysfunction with negative middle ear pressure
- Sub-types (Fiellau-Nikolajsen):
- C1: Peak between −100 to −200 daPa (mild ET dysfunction)
- C2: Peak more negative than −200 daPa (severe ET dysfunction)
- Seen in: early OME, ET dysfunction, post-URTI, initial stage of AOM
SUMMARY TABLE — TYMPANOGRAM TYPES
| Type | Shape | Peak Pressure | Compliance | Condition |
|---|---|---|---|---|
| A | Normal bell | 0 daPa | 0.3–1.6 ml | Normal / SNHL |
| As | Low bell | 0 daPa | <0.3 ml | Otosclerosis, fixation |
| Ad | High bell | 0 daPa | >1.6 ml | Ossicular discontinuity |
| B | Flat | None | Very low | OME, perforation, wax |
| C | Negative peak | < −100 daPa | Variable | ET dysfunction |
(Dhingra, 7th Ed.; Hazarika, 3rd Ed.)
5.4 Additional Tympanogram Types (Liden Classification)
Liden (1969) described:
- Type I (= Jerger A) — Normal
- Type II (= Jerger C) — ET dysfunction
- Type III (= Jerger B) — Flat (effusion/perforation)
6. EQUIVALENT CANAL VOLUME (ECV)
- Measured when pressure is at +200 daPa (TM maximally stiffened)
- Represents volume of air between probe tip and TM
- Normal: 0.6–1.5 ml (adults); 0.4–1.0 ml (children)
| ECV | Tympanogram | Interpretation |
|---|---|---|
| Normal | Type B | OME / Glue ear |
| Large (>2 ml) | Type B | TM perforation / patent grommet |
| Large | Type A | Widely patent Eustachian tube |
7. ACOUSTIC REFLEX TESTING
7.1 Anatomy of the Acoustic Reflex Arc
SOUND (>70 dB above threshold)
│
▼
COCHLEA (VIII nerve - afferent)
│
▼
COCHLEAR NUCLEUS (brainstem)
│
┌───┴───┐
▼ ▼
IPSILATERAL CONTRALATERAL
FACIAL nerve SOC → Facial nerve
(VII) nucleus nucleus (VII)
│ │
▼ ▼
STAPEDIUS STAPEDIUS
MUSCLE MUSCLE
(ipsilateral) (contralateral)
│
▼
Stiffening of ossicular chain
→ Decreased compliance
→ Detected by impedance meter
"The acoustic reflex is a bilateral reflex — both stapedius muscles contract even when only one ear is stimulated" — Scott-Brown's Otorhinolaryngology, 8th Ed.
7.2 Acoustic Reflex Threshold (ART)
- Normal ART: 70–100 dB above pure tone threshold (i.e., 70–100 dB HL for normal hearing)
- Measured at 500, 1000, 2000, 4000 Hz
- The minimum stimulus level that produces a detectable change in compliance is the ART
7.3 Modes of Acoustic Reflex Testing
| Mode | Probe ear | Stimulus ear | Reflex arc involved |
|---|---|---|---|
| Ipsilateral (uncrossed) | Right | Right | Ipsilateral pathway |
| Contralateral (crossed) | Right | Left | Crosses brainstem |
7.4 Clinical Significance of Acoustic Reflexes
A. Conductive Hearing Loss
- Absent reflex in probe ear — stiff middle ear prevents compliance change
- Absent reflex in stimulus ear — sufficient supra-threshold stimulus cannot be generated
- Exception: Third window lesions (SCD, perilymph fistula) — reflex may be present despite conductive loss
- Otosclerosis: Reflex absent "Carhart's notch" pattern on reflex testing (Stell & Maran's)
B. Sensorineural Hearing Loss
| Pattern | Significance |
|---|---|
| ART elevated but present | Cochlear loss — more stimulus needed |
| ART normal/near-normal despite SNHL | Recruitment — cochlear origin |
| ART absent | Retrocochlear lesion (acoustic neuroma, VIII nerve lesion) |
C. Facial Nerve Lesions (Topographic Diagnosis)
FACIAL NERVE LESION LEVELS & ACOUSTIC REFLEX:
1. Distal to stapedius branch
→ Reflex PRESENT (stapedius branch intact)
→ Prognosis: GOOD
2. At/proximal to stapedius branch
→ Reflex ABSENT (stapedius affected)
→ Indicates involvement of stapedius branch
3. At geniculate ganglion / beyond
→ Absent reflex + absent lacrimation (Schirmer's test)
CLINICAL USE: Bell's palsy — if reflex present → good prognosis
"The acoustic reflex is the single most useful test in topographic diagnosis of facial nerve paralysis" — Zakir Hussain, Textbook of ENT, 2019
D. Brainstem Pathology
- Crossed reflex absent + Uncrossed reflex present → Ipsilateral brainstem lesion (afferent pathway affected contralaterally)
- Both crossed and uncrossed absent → Bilateral brainstem disease or severe bilateral hearing loss
7.5 Acoustic Reflex Pattern Analysis
FOUR-VARIABLE REFLEX ANALYSIS:
(IP = Ipsilateral probe; IS = Ipsilateral stimulus)
(CP = Contralateral probe; CS = Contralateral stimulus)
Testing Right ear lesion:
PROBE EAR
L R
STIMULUS L CP/LS CP/RS
EAR R CS/LP IP/RS
If RIGHT VIII nerve lesion:
→ Stimulus to RIGHT (both modes using R as stimulus) = ABSENT
→ Stimulus to LEFT = may be present
8. ACOUSTIC REFLEX DECAY (REFLEX THRESHOLD DECAY — RTD)
8.1 Principle
A sustained tone at 10 dB above the ART is presented for 10 seconds. The compliance change is monitored. In cochlear lesions, the reflex is sustained. In retrocochlear (neural) lesions, the stapedius muscle fatigues and the reflex decays.
8.2 Interpretation
ACOUSTIC REFLEX DECAY TEST:
Compliance
(mm)
│ Cochlear: ─────────────────── (sustained ≥ 50% amplitude)
│
│ Retrocochlear: ──\
│ \\___________ (decay to < 50% within 5 sec)
│
└──────────────────────────────────── Time (10 sec)
| Finding | Interpretation |
|---|---|
| Amplitude maintained ≥ 50% at 5 sec | Cochlear / Normal |
| Amplitude decays to < 50% within 5 sec | Retrocochlear (acoustic neuroma) |
- Tested at 500 Hz and 1000 Hz (most sensitive)
- Sensitivity for acoustic neuroma: 70–90%
- "Reflex decay is the most sensitive non-imaging test for retrocochlear pathology" — Scott-Brown, 8th Ed.
9. EUSTACHIAN TUBE FUNCTION TESTS
9.1 For Intact Tympanic Membrane (Williams Inflation-Deflation Test)
STEP 1: Record baseline tympanogram → note peak pressure
STEP 2: Patient performs Valsalva manoeuvre
STEP 3: Record tympanogram → peak should shift positive
STEP 4: Patient performs Toynbee manoeuvre (swallow with nose pinched)
STEP 5: Record tympanogram → peak should shift negative
STEP 6: Patient swallows normally 3×
STEP 7: Record final tympanogram → should return to baseline
Interpretation: If peak shifts and returns to baseline → ET function normal
9.2 For Perforated Tympanic Membrane (Inflation-Deflation Test)
- Serial tympanograms performed with positive pressure (+200 daPa) applied
- Patient swallows; pressure equalizes through ET into middle ear
- Sonotubometry: broadband noise applied to nose; detected by microphone in ear canal during swallowing — indicates ET patency
10. JERGER'S BATTERY OF TESTS — SITE OF LESION DIAGNOSIS
┌──────────────────────────────────────────────────────────────┐
│ JERGER'S DIAGNOSTIC BATTERY FLOWCHART │
└──────────────────────────────────────────────────────────────┘
TYMPANOMETRY
│
├── Type A → Middle ear normal
│ │
│ └──── ACOUSTIC REFLEXES
│ │
│ ┌───────────┼────────────┐
│ ▼ ▼ ▼
│ PRESENT ABSENT ELEVATED
│ │ │ │ │
│ Normal Conductive Retro- Cochlear
│ loss? cochlear? (confirm
│ Check Check w/ SISI,
│ BC reflex Bekesy)
│ levels decay
│
├── Type B → Middle ear effusion / perforation
│ Check ECV → distinguish
│
└── Type C → ET dysfunction
Consider decongestants / grommets
11. COMPREHENSIVE DIAGNOSTIC INTERPRETATION TABLE
(Compiled from Dhingra, Cummings, Scott-Brown, Hazarika)
| Condition | Tympanogram | ECV | ART | Reflex Decay |
|---|---|---|---|---|
| Normal | Type A | Normal | 70–100 dB SL | Negative |
| OME/Glue ear | Type B | Normal | Absent | — |
| TM perforation | Type B | High (>2 ml) | Absent | — |
| Otosclerosis | Type As | Normal | Absent | — |
| Ossicular discontinuity | Type Ad | Normal | Absent | — |
| ET dysfunction | Type C | Normal | May be present | — |
| Cochlear SNHL | Type A | Normal | Elevated | Negative (sustained) |
| Acoustic neuroma | Type A | Normal | Absent/Elevated | Positive (decay) |
| Bell's palsy (mild) | Type A | Normal | Present | Negative |
| Bell's palsy (severe) | Type A | Normal | Absent | — |
| Brainstem lesion | Type A | Normal | Absent (crossed) | Positive |
12. WIDEBAND TYMPANOMETRY (WBT) — RECENT ADVANCE
(Recent advance — RGUHS 2022–24 pattern)
Traditional tympanometry uses a single 226 Hz probe tone. Wideband/multifrequency tympanometry uses 226–8000 Hz simultaneously.
- Measures absorbance (energy absorbed by middle ear) across all frequencies
- More sensitive for:
- Otosclerosis detection at early stages (low absorbance at 1000 Hz)
- Ossicular discontinuity (high absorbance at 1000–2000 Hz)
- SCD (Superior Canal Dehiscence) — distinctive WBT pattern
- Neonatal screening (226 Hz unreliable in neonates — 1000 Hz probe more accurate)
"In neonates and infants under 6 months, a 1000 Hz probe tone must be used as the ear canal walls are highly compliant and give erroneous results with 226 Hz" — Cummings Otolaryngology, 7th Ed., Chapter on Pediatric Hearing Loss
13. HIGH-FREQUENCY TYMPANOMETRY (678 Hz / 1000 Hz)
| Age Group | Recommended Probe Frequency | Reason |
|---|---|---|
| Adults | 226 Hz | Standard; stiffness-dominated |
| Children <7 months | 1000 Hz | Flaccid canal walls give false Type A at 226 Hz |
| Neonates (NICU) | 1000 Hz | AAA/ASHA recommendation |
14. MULTIFREQUENCY TYMPANOMETRY (MFT)
- Resonant frequency (Fres) of normal middle ear: ~800–1200 Hz
- In otosclerosis: Fres shifts higher (stiffer system)
- In ossicular discontinuity: Fres shifts lower (mass-dominated)
- Helps in differential diagnosis when conventional tympanometry is inconclusive
15. ELECTROACOUSTIC IMPEDANCE BRIDGE — WORKING DIAGRAM
┌──────────────────────────────────────────────────────────┐
│ ELECTROACOUSTIC IMPEDANCE BRIDGE │
│ │
│ ┌────────────┐ ┌─────────────┐ ┌──────────────┐ │
│ │ OSCILLATOR │───▶│ PROBE TONE │───▶│ EAR CANAL │ │
│ │ (226 Hz) │ │ SPEAKER │ │ (sealed) │ │
│ └────────────┘ └─────────────┘ └──────┬───────┘ │
│ │ │
│ ┌─────────────┐ ┌──────────────┐ ┌──────▼───────┐ │
│ │ RECORDER/ │◀─│ BRIDGE │◀──│ MICROPHONE │ │
│ │ DISPLAY │ │ CIRCUIT │ │ (in probe) │ │
│ └─────────────┘ └──────────────┘ └──────────────┘ │
│ │
│ ┌────────────────────────────────────┐ │
│ │ AIR PUMP (manometer) │ │
│ │ +200 → 0 → −400 daPa │ │
│ └────────────────────────────────────┘ │
│ │
│ CONTRALATERAL STIMULATOR: Pure tone / noise delivered │
│ via headphone to opposite ear for reflex testing │
└──────────────────────────────────────────────────────────┘
16. STEP-BY-STEP PROCEDURE
- Otoscopic examination — exclude wax, perforation, otitis externa
- Select appropriate probe tip — ensure hermetic seal
- Explain procedure to patient (remain still, no swallowing during test)
- Insert probe into ear canal
- Perform tympanometry — pressure swept from +200 to −400 daPa automatically
- Record static compliance and peak pressure
- Test acoustic reflexes — ipsilateral and contralateral at 500, 1000, 2000, 4000 Hz
- Perform reflex decay if ART is present (at 500 Hz and 1000 Hz)
- Eustachian tube function testing if indicated
- Repeat for other ear
17. ADVANTAGES OF IMPEDANCE AUDIOMETRY
- Objective — does not require patient cooperation
- Non-invasive — no discomfort
- Can be performed in infants, young children, malingerers, mentally challenged
- Rapid — takes 5–10 minutes per ear
- Differentiates conductive vs. sensorineural vs. retrocochlear lesions
- Topographic diagnosis of facial nerve lesions
- Essential in medicolegal and occupational hearing assessment
18. LIMITATIONS
- Requires hermetic seal — impossible with large EAC anomalies
- Cannot be used in active otitis externa
- False results in TM perforations
- 226 Hz probe unreliable in neonates < 6 months
- Operator-dependent for interpretation
- Does not measure absolute hearing thresholds (pure tone audiometry still required)
19. RECENT ADVANCES (RGUHS 2022–2024 Focus)
19.1 Wideband Acoustic Immittance (WAI)
- Measures energy reflectance from 226 to 8000 Hz in a single sweep
- More sensitive for diagnosing otosclerosis, SCD, perilymph fistula
- Replaces need for multiple probe tone frequencies
19.2 Acoustic Reflex in Cochlear Implant Evaluation
- Electrically Evoked Stapedial Reflex (eSR) used intraoperatively during cochlear implantation to:
- Confirm electrode placement
- Set comfortable listening levels (C-levels)
- Avoid overstimulation of auditory nerve
- The stapedius tendon is directly visualized and monitored (as shown in the surgical image below)
19.3 High-Frequency Tympanometry for Neonatal Hearing Screening
- Incorporated into Universal Newborn Hearing Screening (UNHS) programs
- 1000 Hz tympanometry combined with OAE improves specificity of OME detection in neonates
19.4 Multifrequency Impedance Testing (MFT)
- Resonant frequency mapping to differentiate stiffness vs. mass-dominated disorders
- Useful pre-operatively in stapes surgery planning
19.5 Wideband Reflectance for SCD (Superior Canal Dehiscence)
- Characteristic pattern: high power absorbance at 1000 Hz differentiates SCD from otosclerosis
19.6 Machine Learning in Tympanogram Interpretation
- AI algorithms trained on thousands of tympanograms achieving >95% accuracy in Type A/B/C classification
- Integrated into modern digital impedance audiometers
20. INTRAOPERATIVE STAPEDIUS REFLEX MONITORING
(Surgical anatomy image below)
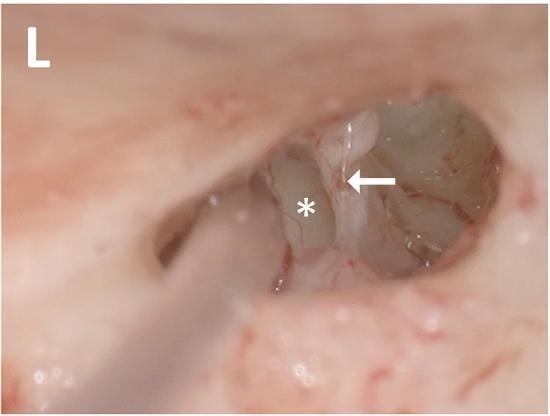
Intraoperative view of the left middle ear showing the stapedius tendon (arrow) and cochlear promontory (asterisk). The motion of the stapedius tendon in response to electrical stimulation — the electrically evoked stapedial reflex (eSR) — is used to verify electrode placement during cochlear implantation and set appropriate stimulation levels. (Source: PMC Clinical VQA)
21. CLINICAL FLOWCHART — APPROACH TO PATIENT WITH SUSPECTED MIDDLE EAR PATHOLOGY
PATIENT WITH HEARING LOSS / EAR COMPLAINTS
│
▼
OTOSCOPIC EXAMINATION
│
┌───────┴────────┐
▼ ▼
TM INTACT TM PERFORATED
│ │
▼ ▼
TYMPANOMETRY ONLY ECV VALID
│ (no peak expected)
┌────┴────┐
▼ ▼ ▼
Type A Type B Type C
│ │ │
Normal OME? ET DYSFX
│ (ECV normal) │
▼ │ Medical Rx
ACOUSTIC ▼ ± Grommets
REFLEX TM PERF?
TESTING (ECV large)
│
┌──┴──────────┐
▼ ▼
PRESENT ABSENT
│ │
├─Normal ART ├─ Conductive?
│ → Normal │ (Type As/Ad)
│ │
├─Elevated ├─ Retrocochlear?
│ ART │ → Reflex Decay
│ → Cochlear │ → MRI IAM
│
└─Reflex Decay (+)
→ RETROCOCHLEAR
→ MRI with contrast
22. SUMMARY — KEY POINTS FOR EXAMINATION
- Impedance audiometry = objective test of middle ear function
- Based on the principle that maximum compliance of TM occurs when middle ear pressure = ear canal pressure
- Jerger's Types: A (normal), As (stiff), Ad (discontinuity), B (flat/effusion), C (ET dysfunction)
- ECV distinguishes Type B due to OME (normal) from perforation (large)
- Acoustic reflex: absent in conductive loss and most retrocochlear lesions; elevated in cochlear SNHL
- Reflex decay: positive (>50% decay in 5 sec) = retrocochlear lesion
- Neonates: Use 1000 Hz probe, not 226 Hz
- Facial nerve: acoustic reflex helps localize lesion relative to stapedius branch
- Recent advances: Wideband tympanometry (WAI), eSR in cochlear implants, AI interpretation
- 226 Hz probe is stiffness-dominated; most useful in adults with suspected middle ear disease
REFERENCES
- Harrison's Principles of Internal Medicine, 21st Ed. — pp. 1039–1040
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, 8th Ed. — Chapter on Audiological Assessment
- Cummings Otolaryngology — Head and Neck Surgery, 7th Ed. — Chapter on Audiologic Testing
- Dhingra PL & Dhingra S — Diseases of ENT, 7th Ed. — Chapter on Hearing Tests
- Hazarika P — Textbook of ENT & Head-Neck Surgery, 3rd Ed. — Chapter on Audiological Assessment
- Zakir Hussain — Textbook of ENT, 2019 — Site of Lesion Tests
- Stell & Maran's — Head and Neck Surgery, 5th Ed.
- Jerger J (1970) — Clinical experience with impedance audiometry. Archives of Otolaryngology 92(4): 311–324
- Keefe DH et al. — Wideband acoustic admittance and its relationship to hearing loss. JASA 2017
- AAA Clinical Practice Guidelines — Conductive Hearing Loss and Tympanometry, 2012 & 2021 updates
Exam Tip (RGUHS): For a 50-mark question, ensure coverage of: (1) Principle + Physics, (2) Instrument, (3) Tympanogram types with diagrams, (4) Acoustic reflex anatomy + clinical significance, (5) Reflex decay, (6) ET function tests, (7) Clinical interpretation table, (8) Recent advances. Diagrams of tympanogram types and the acoustic reflex arc always fetch full marks.
This is a shared conversation. Sign in to Orris to start your own chat.