Jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, well-structured answer.
Jaundice
Jaundice (icterus) is the yellowish discoloration of the skin, sclerae, and mucous membranes caused by accumulation of bilirubin in tissues. It becomes clinically detectable when serum bilirubin rises above 2.5-3 mg/dL (normal: <1 mg/dL). - Schwartz's Principles of Surgery, 11th Ed.
Bilirubin Metabolism - The Foundation
Understanding jaundice requires understanding the bilirubin pathway:
Step-by-step:
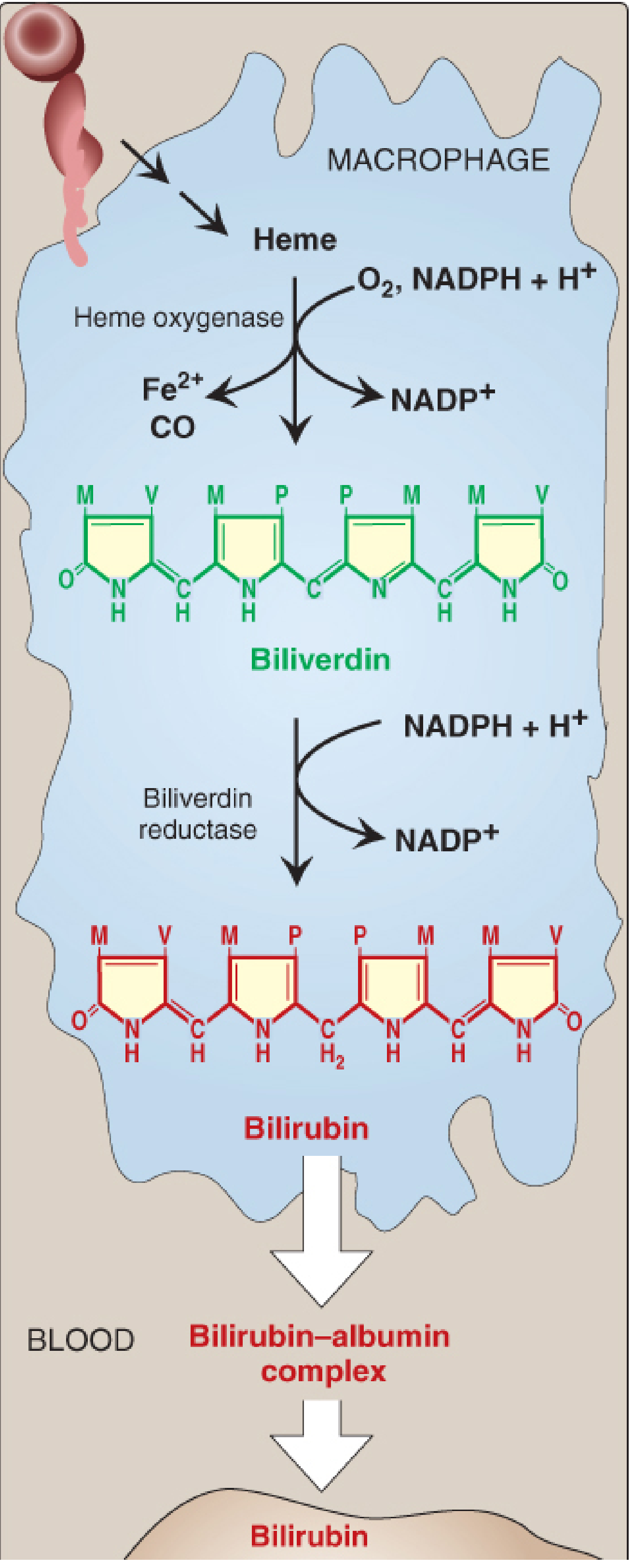
- Production: ~85% of bilirubin comes from senescent RBCs (lifespan ~120 days). Heme oxygenase in macrophages of the mononuclear phagocyte system opens the porphyrin ring, releasing Fe²+ and CO, and producing biliverdin (green). Biliverdin reductase then reduces it to bilirubin (red-orange).
- Transport: Bilirubin is insoluble in plasma - it travels to the liver bound to albumin as unconjugated bilirubin (UCB) (= indirect bilirubin).
- Hepatic uptake & conjugation: Bilirubin dissociates from albumin, enters hepatocytes via facilitated diffusion, and is conjugated with two glucuronic acid molecules by UDP-glucuronosyltransferase (UDPGT) to form bilirubin diglucuronide - now water-soluble conjugated bilirubin (CB) (= direct bilirubin).
- Excretion: CB is secreted into bile, passes through the intestine, where bacteria convert it to urobilinogen. Urobilinogen is partially reabsorbed (enterohepatic circulation) and excreted in urine; the rest is oxidized in stool to stercobilin (brown color of stool). - Lippincott's Biochemistry, 8th Ed.
Classification of Jaundice
Jaundice is classified by the site of dysfunction into three types:
| Feature | Prehepatic (Hemolytic) | Hepatic (Hepatocellular) | Posthepatic (Obstructive) |
|---|---|---|---|
| Bilirubin type elevated | UCB (indirect) only | Both UCB + CB | CB (direct) only |
| Urine color | Normal/slightly dark | Dark (urobilinogen ↑) | Dark (bilirubinuria) |
| Stool color | Normal/dark | Pale (clay-colored) | Pale (clay-colored) |
| Urine urobilinogen | ↑ | ↑↑ | Absent |
| ALT/AST | Normal | ↑↑ | Normal / mild ↑ |
| Alkaline phosphatase | Normal | Normal / mild ↑ | ↑↑ |
| Pruritus | Absent | Variable | Present (bile salts) |
1. Prehepatic (Hemolytic) Jaundice
Excessive heme degradation overwhelms the liver's conjugating capacity (normally can handle >3,000 mg/day vs. normal production of ~300 mg/day). UCB accumulates. Serum bilirubin rarely exceeds 5 mg/dL in pure hemolysis. - Harrison's Principles of Internal Medicine, 22nd Ed.
Causes:
- Inherited hemolytic anemias: Hereditary spherocytosis, sickle cell disease, thalassemia, G6PD deficiency, pyruvate kinase deficiency
- Acquired hemolytic anemias:
- Immune-mediated (positive Coombs test): autoimmune, drug-induced
- Non-immune: microangiopathic hemolytic anemia (HUS), paroxysmal nocturnal hemoglobinuria, malaria, babesiosis, mechanical (prosthetic heart valves)
- Ineffective erythropoiesis: cobalamin, folate, or iron deficiency
- Other: resorption of large hematomas, massive blood transfusion
Note: In chronic hemolysis, pigmented (calcium bilirubinate) gallstones are common and can cause coincidental choledocholithiasis. - Harrison's, 22nd Ed.
2. Hepatic (Hepatocellular) Jaundice
Damage to hepatocytes impairs uptake, conjugation, and/or excretion of bilirubin, causing both UCB and CB to accumulate.
Causes:
- Viral hepatitis (A, B, C, E; EBV, CMV)
- Alcoholic hepatitis
- Drug toxicity (paracetamol/acetaminophen overdose, isoniazid, halothane)
- Cirrhosis
- Autoimmune hepatitis
- Hereditary conditions:
- Gilbert's syndrome: Reduced UDPGT activity (10-35% of normal); benign; mild unconjugated hyperbilirubinemia triggered by fasting, illness, or stress. Affects 4-7% of the population
- Crigler-Najjar type I: Complete absence of UDPGT; severe jaundice (>20 mg/dL), kernicterus, usually fatal in infancy without liver transplantation
- Crigler-Najjar type II: Residual UDPGT activity (<10%); bilirubin 6-25 mg/dL; responds to phenobarbital
- Dubin-Johnson syndrome: Defect in secretion of CB from hepatocyte (MRP2 transporter); predominantly conjugated hyperbilirubinemia; benign; black pigment deposits in liver
- Rotor syndrome: Similar to Dubin-Johnson but no liver pigmentation - Harrison's, 22nd Ed.
3. Posthepatic (Obstructive/Cholestatic) Jaundice
Obstruction of bile flow leads to regurgitation of CB back into blood. The absence of bile in the intestine causes pale (clay-colored/acholic) stools, and CB appears in urine (urinary bilirubin = bilirubinuria). Pruritus results from bile salt deposition in skin. - Lippincott's Biochemistry, 8th Ed.
Causes:
Extrahepatic (duct obstruction):
- Malignant: cholangiocarcinoma, pancreatic cancer, gallbladder cancer, ampullary carcinoma, porta hepatis lymph nodes
- Benign: choledocholithiasis (most common), chronic pancreatitis, primary sclerosing cholangitis, postoperative biliary strictures, Mirizzi's syndrome, AIDS cholangiopathy
Intrahepatic cholestasis:
- Primary biliary cholangitis (AMA-positive)
- Drug-induced cholestasis (anabolic steroids, OCP, chlorpromazine, erythromycin estolate)
- Intrahepatic cholestasis of pregnancy
- Alcoholic hepatitis
- Vanishing bile duct syndrome (chronic liver transplant rejection, sarcoidosis)
- Progressive familial intrahepatic cholestasis
- Total parenteral nutrition
- Infections: malaria, leptospirosis, sepsis - Harrison's, 22nd Ed.
Clinical Evaluation
The initial evaluation focuses on two questions:
- Is bilirubin elevated in isolation, or are other liver tests also abnormal?
- Is the hyperbilirubinemia predominantly conjugated (direct) or unconjugated (indirect)?
Key initial labs: Bilirubin with fractionation, ALT, AST, alkaline phosphatase, GGT, prothrombin time, albumin
Pattern recognition:
- Hepatocellular pattern: ALT/AST elevated out of proportion to alkaline phosphatase
- Cholestatic pattern: Alkaline phosphatase elevated out of proportion to ALT/AST
- Isolated hyperbilirubinemia: Direct >15% suggests Dubin-Johnson/Rotor; indirect suggests Gilbert's, Crigler-Najjar, or hemolysis
The following diagnostic algorithm from Harrison's guides the workup:
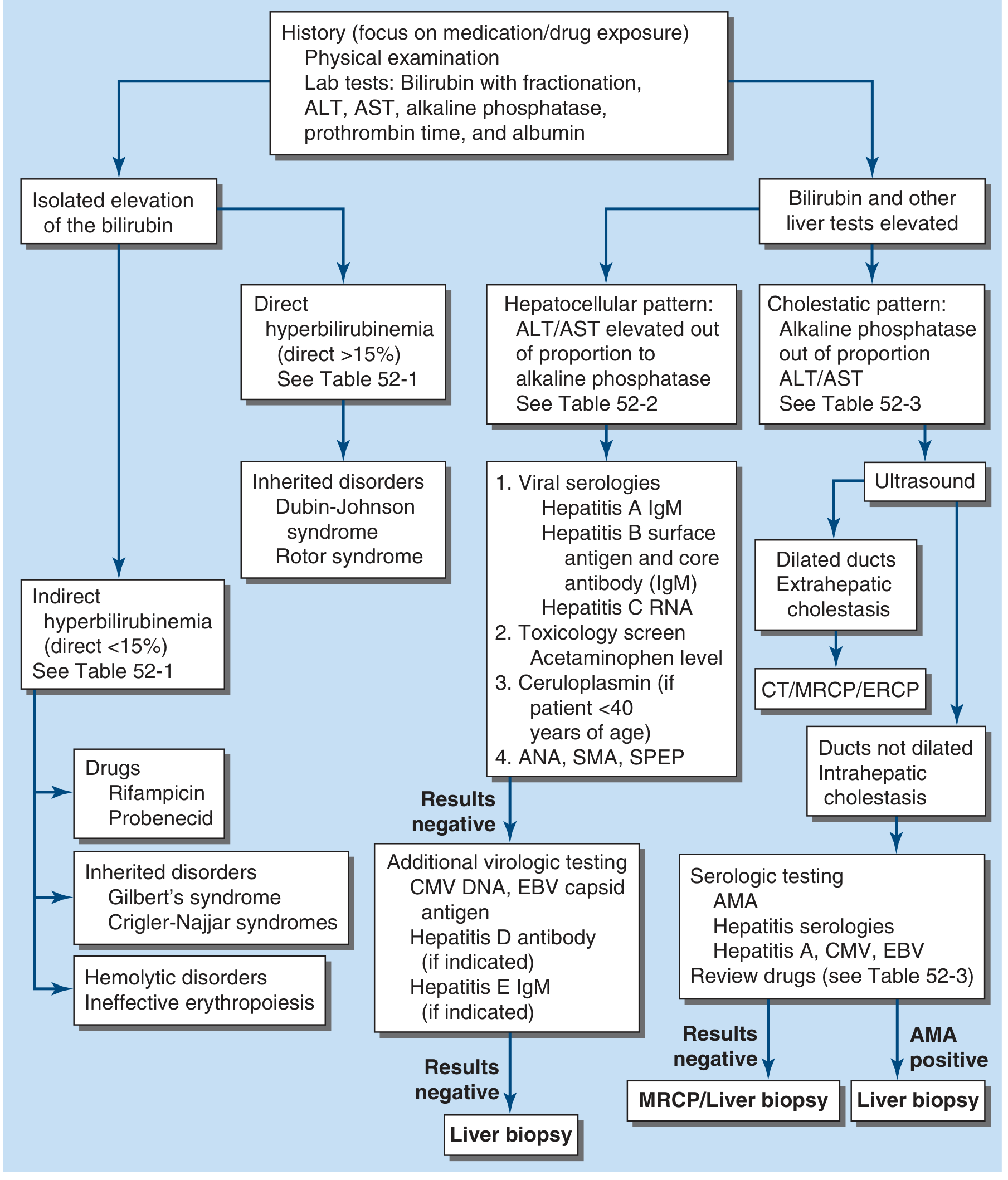
FIGURE 52-1 from Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - Evaluation of the patient with jaundice.
Investigations
| Investigation | Purpose |
|---|---|
| Serum bilirubin (total, direct, indirect) | Classify type of hyperbilirubinemia |
| LFTs (ALT, AST, ALP, GGT) | Distinguish hepatocellular vs. cholestatic |
| PT/INR, albumin | Assess hepatic synthetic function |
| CBC, reticulocyte count, peripheral smear | Screen for hemolysis |
| Direct Coombs test | Immune-mediated hemolysis |
| Viral hepatitis panel (HBsAg, anti-HCV, HAV IgM) | Viral etiology |
| ANA, ASMA, AMA | Autoimmune hepatitis, PBC |
| Ceruloplasmin (age <40) | Wilson's disease |
| Ultrasound abdomen | First-line imaging - dilated ducts? stones? |
| MRCP | Non-invasive biliary tree imaging (replaced ERCP as first-line) |
| ERCP | Therapeutic (stone extraction, stenting) |
| CT abdomen | Malignancy, pancreatic pathology |
| Liver biopsy | When serologies inconclusive |
Special Situations
Neonatal Jaundice
60% of full-term and 80% of preterm neonates develop transient physiologic jaundice in the first week of life. This is because hepatic UDPGT activity is low at birth (reaching adult levels by ~4 weeks). UCB that exceeds albumin's binding capacity (>20-25 mg/dL) can cross the blood-brain barrier and deposit in the basal ganglia, causing kernicterus (bilirubin encephalopathy).
Treatment: Phototherapy with blue fluorescent light converts bilirubin to water-soluble photoisomers that can be excreted without conjugation. Exchange transfusion is used in severe cases.
Pathologic causes include: ABO/Rh incompatibility, G6PD deficiency, biliary atresia, sepsis, hypothyroidism. - Lippincott's Biochemistry, 8th Ed.
Bilirubin Measurement - Van den Bergh Reaction
- Direct (conjugated) bilirubin: reacts rapidly with diazotized sulfanilic acid in aqueous solution (water-soluble)
- Indirect (unconjugated) bilirubin: requires methanol to dissolve before reacting
- Total bilirubin = direct + indirect
Key Distinguishing Points Summary
| Syndrome | Bilirubin type | Key feature |
|---|---|---|
| Gilbert's | Indirect ↑ | Fasting/stress triggered; benign, no treatment needed |
| Crigler-Najjar I | Indirect ↑↑ | Absent UDPGT; kernicterus; liver transplant required |
| Crigler-Najjar II | Indirect ↑ | Residual UDPGT; responds to phenobarbital |
| Dubin-Johnson | Direct ↑ | MRP2 defect; black liver on autopsy |
| Rotor syndrome | Direct ↑ | No liver pigmentation; storage defect |
| Hemolytic | Indirect ↑ | Reticulocyte ↑, LDH ↑, haptoglobin ↓ |
| Obstructive | Direct ↑ | ALP ↑↑, dark urine, pale stools, pruritus |
Sources: Harrison's Principles of Internal Medicine 22nd Ed. (2025), Lippincott's Illustrated Biochemistry 8th Ed., Schwartz's Principles of Surgery 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.