Bullous leison on skin
Reading File
search_medical_text
bullous lesion skin blistering diseases classification etiology diagnosis
search_medical_text
bullous pemphigoid pemphigus vulgaris autoimmune blistering skin treatment
search_medical_image
bullous skin lesion blister dermis epidermis
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive overview of bullous lesions of the skin:
Bullous Lesions of the Skin
A bulla (plural: bullae) is a fluid-filled blister >5 mm in diameter. Lesions <5 mm are termed vesicles. Bullae arise from cleavage either within the epidermis (intraepidermal) or beneath it (subepidermal), and this distinction is the cornerstone of classification.
Classification
Based on Harrison's Principles of Internal Medicine (p. 1582):
I. Primary Mucocutaneous Diseases
A. Primary Blistering Diseases (Autoimmune)
| Disease | Cleavage Level | Key Feature |
|---|---|---|
| Pemphigus vulgaris | Intraepidermal (suprabasal) | Flaccid bullae, oral lesions, anti-Dsg3 Ab |
| Pemphigus foliaceus | Intraepidermal (subcorneal) | Superficial, no mucosal involvement |
| Bullous pemphigoid (BP) | Subepidermal | Tense bullae, elderly, anti-BP180/BP230 Ab |
| Gestational pemphigoid | Subepidermal | Pregnancy-associated |
| Cicatricial pemphigoid | Subepidermal | Mucosal scarring, conjunctival involvement |
| Dermatitis herpetiformis | Subepidermal | Grouped vesicles, gluten-sensitive |
| Linear IgA bullous dermatosis | Subepidermal | Linear IgA at BMZ, drug-triggered |
| Epidermolysis bullosa acquisita | Subepidermal | Trauma-induced, anti-type VII collagen |
B. Secondary (Reactive) Blistering
- Contact dermatitis — chemical/allergic trigger
- Erythema multiforme — target lesions, HSV/Mycoplasma
- Stevens-Johnson Syndrome (SJS) — mucosal involvement, <10% BSA detachment
- Toxic Epidermal Necrolysis (TEN) — >30% BSA, high mortality
- Bullous fixed drug eruption
- Pseudoporphyria
C. Infections
- Herpes zoster / Varicella — dermatomal or generalized vesicles
- Herpes simplex virus (HSV)
- Staphylococcal scalded-skin syndrome (SSSS) — exfoliatin toxin, neonates/children
- Bullous impetigo — S. aureus, honey-colored crust
- Bullous tinea
- Enteroviruses (hand-foot-mouth disease)
II. Systemic Diseases
- Paraneoplastic pemphigus — associated with lymphoma/thymoma
- Porphyria cutanea tarda — sun-exposed areas, fragile skin
- Diabetic bullae (bullosis diabeticorum)
- Bullous lupus erythematosus
Key Differentiating Features
| Feature | Pemphigus Vulgaris | Bullous Pemphigoid |
|---|---|---|
| Age | 40–60 yrs | >70 yrs (mean ~80 yrs in Europe) |
| Bulla type | Flaccid, easily rupture | Tense, intact |
| Mucosa | Frequently involved | Rarely involved |
| Nikolsky sign | Positive | Negative |
| Autoantibody | Anti-Dsg1, Anti-Dsg3 | Anti-BP180, Anti-BP230 |
| Cleavage | Suprabasal (intraepidermal) | Subepidermal (BMZ) |
| Prognosis | More severe | Morbid; 2–3× higher mortality vs age-matched population |
Diagnosis
Clinical
- Nikolsky sign: lateral pressure causes skin slippage → positive in pemphigus vulgaris, TEN
- Asboe-Hansen sign: pressure on bulla causes lateral extension
Investigations
| Test | Purpose |
|---|---|
| Skin biopsy (H&E) | Level of cleavage (intra- vs subepidermal) |
| Direct immunofluorescence (DIF) | Autoantibody deposits at specific sites |
| Indirect immunofluorescence (IIF) | Circulating autoantibodies in serum |
| Salt-split skin IIF | Differentiates BP (roof) from EBA (floor) |
| ELISA | Quantify anti-BP180, anti-Dsg1/3 titers |
| Tzanck smear | Acantholytic cells (pemphigus) or multinucleate giant cells (HSV/VZV) |
| Bacterial/viral cultures | Infectious causes |
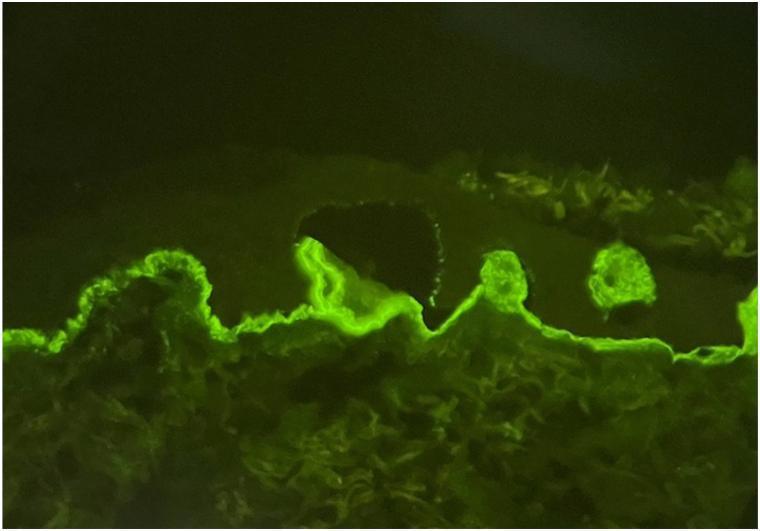
Below is a salt-split skin immunofluorescence study — the epidermis is separated from dermis by 1M NaCl, and IgM deposits (bright green) localize to the floor (dermal side) of the blister, a pattern characteristic of epidermolysis bullosa acquisita or bullous pemphigoid:
Management
Bullous Pemphigoid (most common autoimmune bullous disease)
Per Management of Bullous Pemphigoid guidelines (p. 3):
- First-line: High-potency topical corticosteroids (clobetasol propionate) — preferred over systemic steroids due to lower mortality in extensive disease
- Systemic corticosteroids (prednisone 0.5 mg/kg/day) for widespread involvement
- Adjuvant immunosuppressants: Doxycycline + niacinamide (mild disease); azathioprine, methotrexate, mycophenolate mofetil
- Biologic: Omalizumab (anti-IgE), dupilumab — emerging evidence
- Monitor for steroid complications; the disease carries 2–3× higher mortality vs age-matched population
Pemphigus Vulgaris
- Systemic corticosteroids (mainstay): Prednisone 1 mg/kg/day
- Rituximab (anti-CD20): now first-line in moderate-to-severe disease per many guidelines
- Steroid-sparing agents: Azathioprine, mycophenolate mofetil, cyclophosphamide
- IVIG and plasmapheresis for refractory cases
Infectious Bullae
- Bullous impetigo/SSSS: Antistaphylococcal antibiotics (cloxacillin, dicloxacillin; IV oxacillin for SSSS)
- HSV/VZV: Acyclovir or valacyclovir
SJS/TEN (Dermatologic Emergency)
- Immediate hospitalization, burn unit care
- Discontinue offending drug
- Supportive care: fluid/electrolyte management, wound care
- Cyclosporine, IVIG, TNF-inhibitors considered in select cases
Complications
- Secondary infection / sepsis
- Fluid and electrolyte loss (large bullae/TEN)
- Scarring and contracture (cicatricial pemphigoid, TEN)
- Blindness (ocular involvement in cicatricial pemphigoid)
- Malnutrition (oral pemphigus)
- Drug toxicity from long-term immunosuppression
Clinical Pearl: Always biopsy the edge of a fresh blister (<24h old) for H&E, and perilesional normal skin for DIF, to maximize diagnostic yield. Ruptured/old bullae give non-specific results.
This is a shared conversation. Sign in to Orris to start your own chat.