Traplixam causing hypotension which other alternative drug combination for hyper tension control
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypertension combination antihypertensive treatment alternatives
Reading File
Finding Sources
Searching the Web
Traplixam amlodipine perindopril indapamide hypotension alternative antihypertensive combination
Finding Sources
Reading File
Here is a thorough answer based on textbook evidence and official product information:
Traplixam (Triplixam) Causing Hypotension - Alternative Antihypertensive Combinations
Traplixam / Triplixam = Perindopril (ACE inhibitor) + Indapamide (thiazide-like diuretic) + Amlodipine (dihydropyridine CCB)
Hypotension occurs because all three agents lower BP through complementary mechanisms simultaneously - ACE inhibition reduces angiotensin II-mediated vasoconstriction, indapamide causes volume depletion, and amlodipine causes direct arterial vasodilation. The combination is especially prone to causing hypotension if:
- Patient is volume-depleted or dehydrated
- Dose is too high for the patient's baseline BP
- Used in elderly or frail patients
Step 1 - Before Switching: Optimize First
Before switching entirely, consider:
- Reduce to a lower-strength Triplixam (e.g., from 10/2.5/10 down to 5/1.25/5)
- Remove indapamide temporarily if volume depletion is suspected
- Check posture/timing - take in the morning, ensure adequate hydration
Step 2 - Alternative Two-Drug Combinations (Preferred)
Based on the ACCOMPLISH trial and guidelines (Textbook of Family Medicine 9e), the strongest evidence-based two-drug alternatives are:
| Combination | Example Products | Mechanism | Notes |
|---|---|---|---|
| ACE inhibitor + CCB | Perindopril + Amlodipine (Coveram, Prestalia) | Vasodilation x2 pathways | ACCOMPLISH trial: superior CV outcomes; less hypotension than triple combo |
| ARB + CCB | Valsartan + Amlodipine (Exforge), Telmisartan + Amlodipine (Twynsta) | Similar to above; use if ACE cough | Good for diabetics/proteinuria |
| ACE inhibitor + Thiazide | Perindopril + Indapamide (Coversyl Plus, BiPreterax) | RAAS + volume reduction | Acceptable alternative per guidelines; lower dose = less hypotension risk |
| ARB + Thiazide | Losartan + HCTZ (Hyzaar), Olmesartan + HCTZ | RAAS + volume reduction | Well tolerated; widely used |
| ARB + CCB + low-dose diuretic | Olmesartan + Amlodipine + HCTZ (Tribenzor) | Triple but with ARB | If triple needed, can titrate each component separately |
Key point: The ACE inhibitor + CCB (without diuretic) combination from ACCOMPLISH study is the preferred first choice and carries less hypotension risk than the triple combination in Traplixam.
Step 3 - Beta-Blocker Based Combinations (Second-Line)
Beta-blockers are generally second-line unless there is a compelling indication (heart failure, post-MI, angina):
- Beta-blocker + CCB (e.g., Bisoprolol + Amlodipine) - for patients with angina or high heart rate
- Beta-blocker + Thiazide - effective but metabolically unfavorable
- ACE inhibitor/ARB + Beta-blocker - for heart failure with hypertension
Step 4 - If Three Drugs Still Needed (Resistant Hypertension)
Use components separately so each can be individually titrated:
- ACE-I/ARB + CCB + low-dose thiazide at minimum effective doses
- Add spironolactone 25 mg as 4th agent for true resistant hypertension (strong evidence)
Causes of Hypotension with Traplixam to Address
| Cause | Management |
|---|---|
| Excessive diuresis (indapamide) | Stop or reduce indapamide; ensure fluid intake |
| Over-correction of BP | Target SBP ≥ 120 mmHg (avoid aggressive targets in elderly) |
| Drug-drug interaction | Check NSAIDs, nitrates, sildenafil |
| First-dose effect | Take in morning; check 2-hour post-dose BP |
| Volume depletion (vomiting, diarrhea) | Temporarily hold diuretic component |
Practical Recommendation
If Traplixam is causing symptomatic hypotension, the most evidence-based switch is to:
Perindopril + Amlodipine (dual combination, no diuretic) - e.g., Coveram 5/5 or 10/5 mg once daily
This preserves the ACE inhibitor and CCB components (which showed the best outcomes in ACCOMPLISH), removes the diuretic-driven volume depletion, and allows gentler BP titration. If BP control is still insufficient, indapamide can be added back at the lowest dose (1.25 mg).
- Textbook of Family Medicine 9e, Combination Therapy section: "the most compelling evidence suggests that if two agents are required, a combination of an ACE inhibitor plus a calcium channel blocker (amlodipine) should be used first line based on the ACCOMPLISH study."
Patient lvh with aortic valve calcification
Reading File
Finding Sources
Finding Sources
Searching the Web
LVH aortic valve calcification hypertension management antihypertensive 2024
Finding Sources
Finding Sources
Searching PubMed
left ventricular hypertrophy aortic valve calcification treatment
Reading File
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC6024830
Reading File
Finding Sources
Loading Image
Loading Image
Here is a comprehensive clinical overview of LVH with aortic valve calcification:
LVH with Aortic Valve Calcification - Clinical Overview
Pathophysiology - How They Are Linked
Aortic valve calcification causes calcific aortic stenosis (CAS), which is the most common valvular heart disease in adults over 65. The two conditions are directly connected in a progressive cascade:
Aortic valve calcification → Narrowing of valve orifice → Increased LV afterload → Compensatory concentric LVH
From Robbins Pathologic Basis of Disease:
"The obstruction to left ventricular outflow leads to gradual narrowing of the valve orifice (valve area ~0.5-1 cm² in severe AS; normal ~4 cm²) and an increasing pressure gradient across the calcified valve. Left ventricular pressures rise to 200 mmHg or more, producing concentric left ventricular (pressure overload) hypertrophy."
From Rosen's Emergency Medicine:
"As the valve narrows, increased left ventricular afterload leads to compensatory LVH to maintain cardiac output. LVH and increased wall tension predispose the patient to cardiac ischemia even in the absence of significant coronary artery disease."
Gross Pathology of Calcific Aortic Stenosis
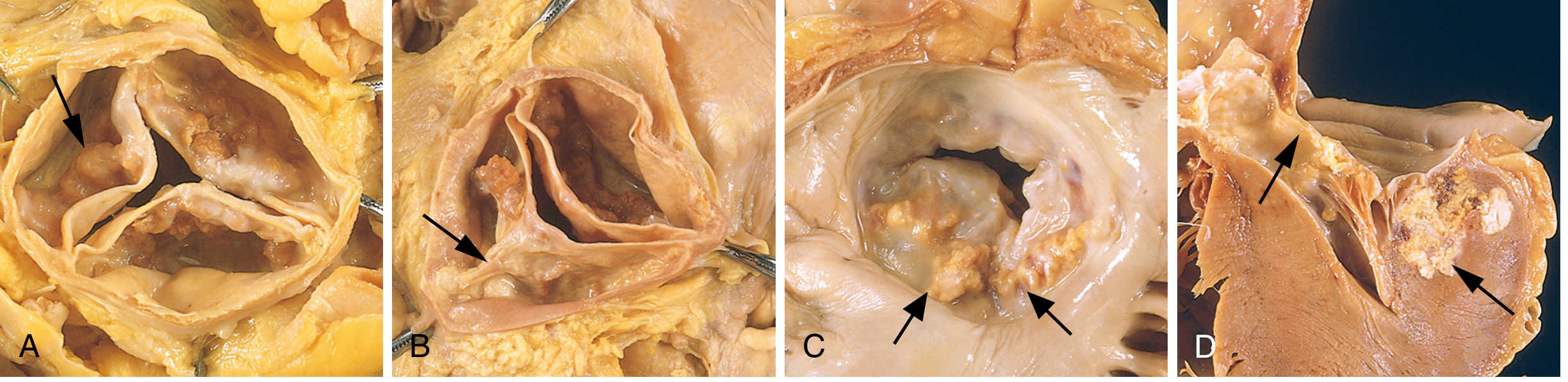
Panel A: Calcific stenosis of a previously normal tricuspid valve - nodular calcium heaped in sinuses of Valsalva (arrow). Commissures are NOT fused (unlike rheumatic disease). Panel B-D: Bicuspid valve variants with accelerated calcification.
Echocardiography - Diagnostic Standard
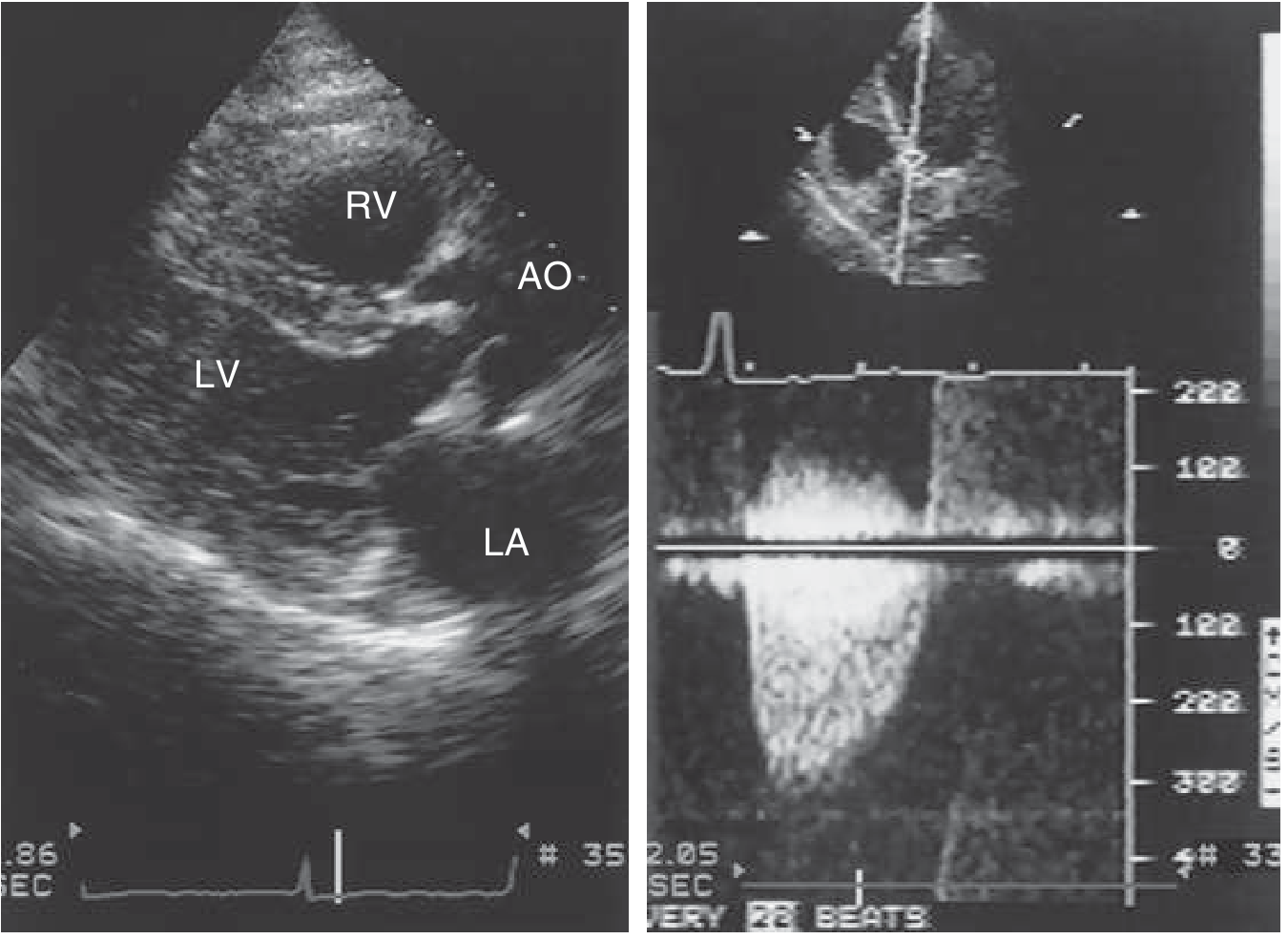
Doppler echo showing restricted aortic valve opening (left panel) and CW Doppler velocity ~3 m/s, peak gradient ~36 mmHg (right panel). ECG shows LVH pattern.
Etiology and Risk Factors
Aortic valve calcification shares risk factors with atherosclerosis but is a distinct active osteogenic process:
| Risk Factor | Comment |
|---|---|
| Age (>65 years) | Most common cause of AS in adults |
| Hypertension | Accelerates calcification progression (PROGRESSA study) |
| Hyperlipidemia | Chronic injury to valve endothelium |
| Bicuspid aortic valve | Stenosis occurs 1-2 decades earlier |
| Male sex | More common in males |
| Chronic kidney disease | Abnormal calcium-phosphate metabolism |
| Diabetes | Metabolic inflammation |
Important: Despite similarities to atherosclerosis, statins do NOT prevent progression of valve calcification. The valve contains osteoblast-like cells that synthesize bone matrix proteins - this distinguishes it from atherosclerosis. (Robbins Pathology)
Severity Classification by Echocardiography
| Severity | Peak Velocity | Mean Gradient | Valve Area |
|---|---|---|---|
| Mild | 2.0-2.9 m/s | <20 mmHg | >1.5 cm² |
| Moderate | 3.0-3.9 m/s | 20-39 mmHg | 1.0-1.5 cm² |
| Severe | ≥4.0 m/s | ≥40 mmHg | <1.0 cm² |
- Peak velocity ≥4 m/s: symptoms usually develop within 2 years
- Peak velocity ≥5 m/s: symptoms likely within 1 year
- Calcium score by CT correlates with severity and can resolve discordant echo findings
Classic Symptom Triad (Severe AS - SAD)
- Syncope - exertional, due to inability to increase cardiac output
- Angina - subendocardial ischemia from hypertrophied LV; also coronary atherosclerosis (coronary angiography recommended pre-op)
- Dyspnea - diastolic dysfunction from stiff hypertrophied LV → heart failure
Prognosis without valve replacement:
- After angina onset: ~5 years survival
- After syncope onset: ~3 years survival
- After heart failure onset: ~2 years survival
LVH in AS - Key Features
- Concentric (pressure overload) hypertrophy - wall thickness increases, cavity size maintained initially
- Diastolic dysfunction develops early - reduced LV compliance → impaired filling
- The hypertrophied LV is preload-dependent - any volume depletion, diuresis, or dehydration can cause acute decompensation
- Atrial fibrillation is poorly tolerated - loss of atrial kick worsens diastolic filling
Management
Medical Management
| Drug Class | Use | Cautions |
|---|---|---|
| ACE inhibitors / ARBs | Preferred for LVH regression + AS; may slow valve calcification (RAS upregulated in AS); benefit in LV remodeling | Start at LOW dose; titrate slowly; avoid in severe AS if symptomatic |
| CCBs (amlodipine) | For hypertension control when ACE/ARB inadequate | Relatively safe |
| Beta-blockers | Useful for rate control (AF), angina; use cautiously | Avoid if significant AR coexists |
| Diuretics | For congestion/heart failure symptoms | Use with caution - LV is preload-dependent; avoid overdiuresis |
| Statins | Do NOT slow progression of valve calcification | Can still be used for concomitant atherosclerosis/dyslipidemia |
From the PROGRESSA study: "Hypertension was shown to accelerate the progression of aortic valve calcification." - treat hypertension aggressively but carefully.
Key principle: Antihypertensive therapy in AS must be started at low doses with careful titration to avoid the hazard of peripheral vasodilation causing hypotension against a fixed obstruction. Vasodilators (nitrates, alpha-blockers, hydralazine) should generally be avoided.
Definitive Treatment - Valve Replacement
| Indication | Action |
|---|---|
| Symptomatic severe AS (any of the SAD triad) | Valve replacement (SAVR or TAVR) |
| Asymptomatic severe AS + EF <50% | Valve replacement |
| Asymptomatic severe AS + exercise-induced hypotension or symptoms | Valve replacement |
| Asymptomatic severe AS with rapid progression | Consider valve replacement |
SAVR vs TAVR choice:
- Low/intermediate surgical risk: either option depending on anatomy and patient preference
- High surgical risk / elderly / frail: TAVR preferred
- Transcatheter approach is now standard in most elderly patients with calcific AS
Emergency Management (Decompensated AS)
- Judicious fluid resuscitation - maintain preload
- Restore sinus rhythm if in AF (atrial kick critical)
- Avoid: vasodilators, aggressive diuresis, inotropes (if possible)
- Vasopressor of choice if needed: phenylephrine or norepinephrine
- IABP as bridge to surgery if no response to medical therapy
- Urgent TAVR/SAVR referral
ECG Findings in LVH + AS
- LVH voltage criteria (Sokolow-Lyon: SV1 + RV5 ≥35 mm)
- Strain pattern (ST depression + T-wave inversion in lateral leads V4-V6, I, aVL)
- Left axis deviation
- Left atrial enlargement (P-wave abnormalities)
- LBBB (late stage)
- Atrial fibrillation (late stage)
Summary - Key Clinical Points
- Aortic valve calcification → progressive stenosis → chronic LV pressure overload → concentric LVH
- LVH makes the heart stiff and ischemia-prone, even without CAD
- Treat hypertension (ACE-I/ARB preferred) but start low and go slow - the fixed obstruction is unforgiving with vasodilators
- Statins do NOT slow valve calcification despite atherosclerosis-like risk factors
- Once symptomatic, only valve replacement (SAVR or TAVR) improves prognosis
- The LVH may partly regress after successful valve replacement
Sources: Robbins Pathologic Basis of Disease; Rosen's Emergency Medicine; Goldman-Cecil Medicine; PROGRESSA study (PMC6024830); 2024 ESC Hypertension Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.