Infective endocarditis full details for md exams 15marks
Reading File
search_medical_text
infective endocarditis etiology pathogenesis classification organisms Duke criteria
search_medical_text
infective endocarditis clinical features diagnosis echocardiography management treatment complications
search_medical_image
infective endocarditis vegetation echocardiography peripheral signs
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-ready answer on Infective Endocarditis structured for a 15-mark MD examination.
INFECTIVE ENDOCARDITIS (IE)
Comprehensive MD Exam Answer — 15 Marks
DEFINITION
Infective endocarditis is a microbial infection of the endocardial surface of the heart, predominantly involving the cardiac valves (native or prosthetic), but also chordae tendineae, mural endocardium, or intracardiac devices. The hallmark lesion is the vegetation — a mass of platelets, fibrin, microorganisms, and inflammatory cells.
CLASSIFICATION
| Type | Features |
|---|---|
| Acute IE (AIE) | Virulent organisms (e.g., S. aureus), rapid destruction, high mortality if untreated |
| Subacute IE (SBE) | Less virulent (e.g., viridans streptococci), indolent course, weeks–months |
| Native Valve IE (NVE) | On structurally normal or abnormal native valves |
| Prosthetic Valve IE (PVE) | Early PVE: <60 days post-op; Late PVE: >60 days |
| IVDA-associated IE | Right-sided (tricuspid), S. aureus predominant |
| Healthcare-associated IE | Nosocomial or non-nosocomial, devices/catheters |
ETIOLOGY / CAUSATIVE ORGANISMS
Native Valve IE:
| Organism | % of Cases |
|---|---|
| Staphylococcus aureus (MSSA/MRSA) | 30–35% (most common overall) |
| Viridans streptococci (S. mutans, S. sanguinis) | 20–25% |
| Enterococcus faecalis | 10% |
| Streptococcus gallolyticus (bovis) | 5–10% (associated with colon cancer) |
| HACEK group | 5% |
| CoNS (S. epidermidis) | 5% |
| Culture-negative | 5–10% |
HACEK Group:
Haemophilus, Aggregatibacter (Actinobacillus), Cardiobacterium hominis, Eikenella corrodens, Kingella kingae — slow-growing, fastidious gram-negatives.
Culture-negative IE Organisms:
- Coxiella burnetii (Q fever), Bartonella spp., Tropheryma whipplei, Brucella spp., fungi (Candida, Aspergillus)
Prosthetic Valve IE (Early <60 days):
- CoNS, S. aureus, gram-negatives, fungi
Prosthetic Valve IE (Late >60 days):
- Viridans streptococci, enterococci (similar to NVE)
PREDISPOSING CONDITIONS (Risk Factors)
Cardiac:
- Rheumatic heart disease (most common in developing countries) — mitral valve most affected
- Congenital heart disease (VSD, PDA, bicuspid aortic valve, TOF)
- Prosthetic valves (mechanical > biological)
- MVP with regurgitation
- Prior IE
- Hypertrophic obstructive cardiomyopathy
Non-cardiac:
- IV drug abuse (IVDA) — tricuspid valve, S. aureus
- Intravascular catheters, pacemakers, ICDs
- Hemodialysis
- Immunosuppression (HIV, malignancy, DM)
- Poor dental hygiene / recent dental procedures
- Elderly patients (degenerative valve disease)
PATHOGENESIS
Endothelial damage → Platelet-fibrin thrombus (NBTE) → Bacteremia →
Microbial adherence to NBTE → Vegetation formation →
Local destruction + Systemic emboli + Immune complex disease
- Endothelial injury from turbulent flow, jet lesions, catheters exposes subendothelial matrix
- Non-bacterial thrombotic endocarditis (NBTE) forms — sterile platelet-fibrin deposits
- Transient bacteremia (dental, GI, GU procedures or spontaneous) seeds the NBTE
- Microbial adherence via surface adhesins (fibronectin-binding proteins in S. aureus; dextran in streptococci)
- Vegetation grows — organisms inside are protected from host defenses and antibiotics (metabolically quiescent, deep within biofilm)
- Consequences: valve destruction, abscess, emboli, immune complex deposition
CLINICAL FEATURES
IE can present as acute, rapidly progressive illness or subacute/chronic disease with non-specific symptoms. High suspicion is needed in febrile patients with risk factors (Management of Endocarditis, p. 18).
A. Systemic / Constitutional:
- Fever — most common symptom (>90%); may be low-grade or absent in elderly/immunosuppressed
- Chills, night sweats, malaise, anorexia, weight loss
- Arthralgia, myalgia
B. Cardiac Manifestations:
- New/changing murmur — regurgitant murmur (aortic/mitral most common)
- Heart failure — most common cause of death
- Conduction abnormalities — AV block, bundle branch block (suggests perivalvular abscess)
- Pericarditis (rare)
C. Peripheral / Embolic Manifestations:
| Sign | Description | Mechanism |
|---|---|---|
| Petechiae | Conjunctiva, palate, skin | Emboli / vasculitis |
| Osler's nodes | Painful, tender, erythematous nodules — fingertips, toes | Immune complex deposition |
| Janeway lesions | Painless erythematous hemorrhagic macules — palms, soles | Septic emboli (vasculitis) |
| Splinter hemorrhages | Linear, dark-red hemorrhages under nails | Emboli |
| Roth spots | Oval retinal hemorrhages with pale center | Immune complex / emboli |
| Clubbing | Seen in subacute/chronic cases | |
| Splenomegaly | Common in subacute IE | Immune stimulation |
Mnemonic for peripheral signs: "ONJRS + Petechiae" — Osler, Nail (splinter), Janeway, Roth spots
D. Embolic Complications:
- Stroke (cerebral emboli) — most common CNS manifestation
- Pulmonary emboli (right-sided IE)
- Splenic, renal, mesenteric infarction
- Mycotic aneurysm (cerebral, aortic) — due to seeding of arterial wall
INVESTIGATIONS
1. Blood Cultures (Cornerstone of Diagnosis)
- 3 sets from different venepuncture sites, before antibiotics
- Drawn ≥1 hour apart (or all 3 within 1 hour in acute/unstable patients)
- Both aerobic and anaerobic bottles; hold for 14 days for fastidious organisms
- Yield: ~90% of cases
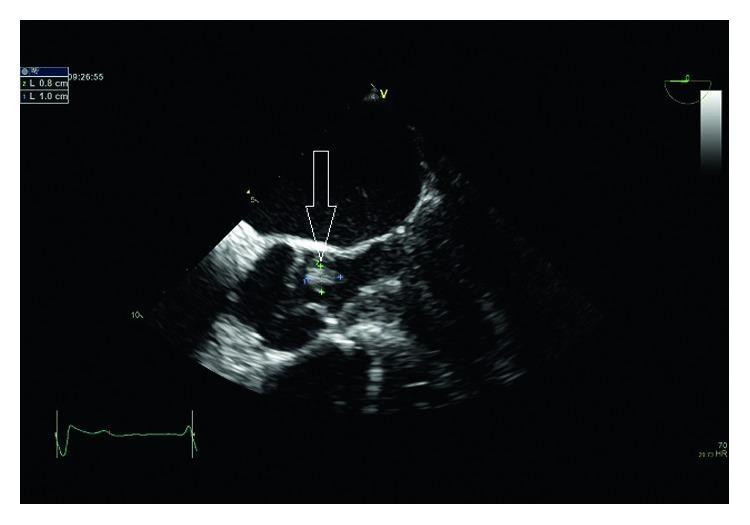
2. Echocardiography
| Modality | Sensitivity | Specificity |
|---|---|---|
| TTE (Transthoracic Echo) | 60–75% | 98% |
| TEE (Transesophageal Echo) | 90–95% | 98% |
TEE is gold standard — indicated when:
- TTE non-diagnostic
- Prosthetic valves
- Staphylococcal bacteremia
- Suspected perivalvular abscess
- Suspected PVE
Echocardiographic criteria for vegetation: Oscillating intracardiac mass on valve or supporting structures, abscess, new dehiscence of prosthetic valve, new valvular regurgitation (Harrison's, p. 3861).
3. Laboratory Tests:
| Test | Findings |
|---|---|
| CBC | Leukocytosis (acute), anemia of chronic disease |
| ESR, CRP | Elevated |
| Rheumatoid factor | Positive (~50% in SBE) |
| Urinalysis | Microscopic hematuria, proteinuria, red cell casts |
| Serum creatinine | Elevated if renal emboli/glomerulonephritis |
| Complement (C3, C4) | Low in immune complex GN |
| Blood cultures | As above |
| Serology | For culture-negative IE (Coxiella, Bartonella, Brucella) |
4. Other Imaging:
- CT scan (brain, chest, abdomen/pelvis): detect emboli, mycotic aneurysms, abscesses
- 18F-FDG PET/CT: useful for PVE, cardiac device IE, occult emboli
- Cardiac MRI: perivalvular extension
- Dental OPG / orthopantomogram: identify dental focus
DUKE CRITERIA (Modified)
Harrison's Principles, p. 3861
Major Criteria:
-
Positive blood culture for typical organisms:
- Viridans streptococci, S. gallolyticus, HACEK group, S. aureus, community-acquired enterococci in the absence of a primary focus
- Persistently positive cultures (>12 h apart, or ≥3 of ≥4 cultures)
- Single positive culture for Coxiella burnetii OR phase I IgG titer >1:800
-
Evidence of endocardial involvement:
- Positive echo: oscillating intracardiac mass, abscess, new prosthetic valve dehiscence
- New valvular regurgitation
Minor Criteria:
- Predisposing heart condition or IVDA
- Fever ≥38°C
- Vascular phenomena: arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, Janeway lesions
- Immunological phenomena: glomerulonephritis, Osler's nodes, Roth spots, rheumatoid factor
- Microbiological: positive blood culture not meeting major criteria
- Echocardiographic: consistent findings not meeting major criteria
Scoring:
| Category | Criteria |
|---|---|
| Definite IE | 2 major, OR 1 major + 3 minor, OR 5 minor |
| Possible IE | 1 major + 1 minor, OR 3 minor |
| Rejected | Firm alternate diagnosis, resolution with ≤4 days antibiotics, or no pathologic evidence at surgery/autopsy |
MANAGEMENT
Principles:
- Prolonged bactericidal antibiotics (parenteral) — 4–6 weeks
- Early surgery for high-risk patients
- Multidisciplinary "Endocarditis Team" (cardiologist, cardiac surgeon, infectious disease specialist, microbiologist)
Antibiotic Regimens:
Streptococcal IE (Penicillin-susceptible, MIC ≤0.125 μg/mL):
| Regimen | Duration |
|---|---|
| IV Penicillin G 12–18 MU/day ÷ 6 doses | 4 weeks |
| OR Ceftriaxone 2 g IV once daily | 4 weeks |
| OR Penicillin/Ceftriaxone + Gentamicin 3 mg/kg/day | 2 weeks (short course, uncomplicated) |
| Penicillin-allergic: Vancomycin 30 mg/kg/day | 4 weeks |
Staphylococcal IE (MSSA — Native Valve):
- Nafcillin/Oxacillin 12 g/day IV ÷ 6 doses × 6 weeks
- Penicillin-allergic: Cefazolin or Vancomycin
Staphylococcal IE (MRSA or Penicillin-allergic):
- Vancomycin 30–45 mg/kg/day IV ÷ 2–3 doses × 6 weeks
- Or Daptomycin 8–10 mg/kg/day (alternative, cannot use for pulmonary IE)
Enterococcal IE:
- Ampicillin 12 g/day + Gentamicin 3 mg/kg/day × 4–6 weeks
- OR Ampicillin + Ceftriaxone (for high-level aminoglycoside resistance)
- Vancomycin + Gentamicin (if penicillin-allergic)
HACEK organisms:
- Ceftriaxone 2 g/day × 4 weeks
- Or Ampicillin-sulbactam
Prosthetic Valve IE (MRSA):
- Vancomycin + Gentamicin + Rifampicin (600 mg/day, added after 3–5 days) × 6 weeks
Surgical Indications (Early Surgery):
Heart Failure (most common indication):
- Severe AR or MR with heart failure, pulmonary edema, or cardiogenic shock
- Severe AR with hemodynamic compromise
- Fistula into cardiac chamber
Uncontrolled Infection:
- Perivalvular abscess, fistula, false aneurysm
- Enlarging vegetation despite antibiotics
- Fungi or multiresistant organisms
- Persistent bacteremia/fever >7–10 days despite appropriate therapy
Prevention of Embolism:
- Vegetation >10 mm with prior embolic events
- Very large vegetation (>15 mm)
- Isolated very large vegetation >10 mm with other predictors of complicated course
Timing: Emergency (<24 hrs), urgent (<few days), elective (after 1–2 weeks)
COMPLICATIONS
| System | Complication |
|---|---|
| Cardiac | Heart failure (most common/most lethal), perivalvular abscess, fistula, pericarditis, AV block |
| Neurological | Embolic stroke (15–35%), mycotic aneurysm, hemorrhagic transformation, meningitis, brain abscess |
| Renal | Immune complex GN (diffuse/focal), renal infarction, drug nephrotoxicity |
| Splenic | Splenic abscess, splenic infarction |
| Vascular | Mycotic aneurysm (intracranial, aortic), peripheral emboli |
| Pulmonary | Septic emboli (right-sided IE) → pulmonary abscesses |
PROPHYLAXIS
Indications (High-Risk Cardiac Conditions):
- Prosthetic cardiac valve
- Previous IE
- Unrepaired cyanotic CHD
- Repaired CHD with residual defects near prosthetic material
- Cardiac transplant with valvulopathy
Procedure:
- Dental procedures involving manipulation of gingival tissue or periapical region of teeth
Regimen:
| Situation | Drug | Dose |
|---|---|---|
| Standard | Amoxicillin | 2 g PO 30–60 min before |
| Unable to take oral | Ampicillin 2 g IM/IV | |
| Penicillin-allergic | Clindamycin 600 mg PO | |
| Penicillin-allergic, IV | Clindamycin 600 mg IV |
Note: Prophylaxis is NOT recommended for GI/GU procedures by current AHA/ESC guidelines unless active IE is present.
PROGNOSIS
- In-hospital mortality: 15–30% overall
- 1-year mortality: up to 40%
- Worse prognosis with: S. aureus, prosthetic valve, perivalvular extension, heart failure, large vegetations, stroke, older age, diabetes
- Better prognosis with: streptococcal IE, early surgery when indicated
HIGH-YIELD EXAM SUMMARY TABLE
| Feature | Key Point |
|---|---|
| Most common organism (overall) | S. aureus |
| Most common in developing countries | Rheumatic heart disease → mitral valve |
| Most common organism (SBE) | Viridans streptococci |
| Most common organism (IVDA) | S. aureus → tricuspid valve |
| Most common organism (PVE early) | CoNS (S. epidermidis) |
| Most common cause of death | Heart failure |
| Most common embolic site | Brain (stroke) |
| Gold standard echo | TEE |
| Duke: Definite IE | 2 major / 1 major + 3 minor / 5 minor |
| Prophylaxis — standard | Amoxicillin 2 g PO before dental procedure |
| S. gallolyticus IE association | Colon cancer — must screen |
| MSSA NVE drug of choice | Nafcillin/Oxacillin |
| MRSA IE drug of choice | Vancomycin |
| Right-sided IE unique feature | Septic pulmonary emboli, responds to medical Rx |
| Immune phenomena | Osler's nodes, Roth spots, RF positive, GN |
| Septic emboli phenomena | Janeway lesions, splinter hemorrhages |
Sources: Harrison's Principles of Internal Medicine, 21st Edition (p. 3861) | ESC/Management of Endocarditis Guidelines (p. 18) | AHA Endocarditis Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.