Thrombosis & embolus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I have a comprehensive set of information. Now let me compile a thorough answer from all the Robbins Cotran content I've gathered.
Thrombosis & Embolism
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease
THROMBOSIS
A thrombus is a solid mass of blood constituents (platelets, fibrin, RBCs, WBCs) formed within the vascular system during life. It is pathological clot formation - distinct from normal hemostasis.
Virchow's Triad
The three primary abnormalities leading to thrombosis form Virchow's triad:
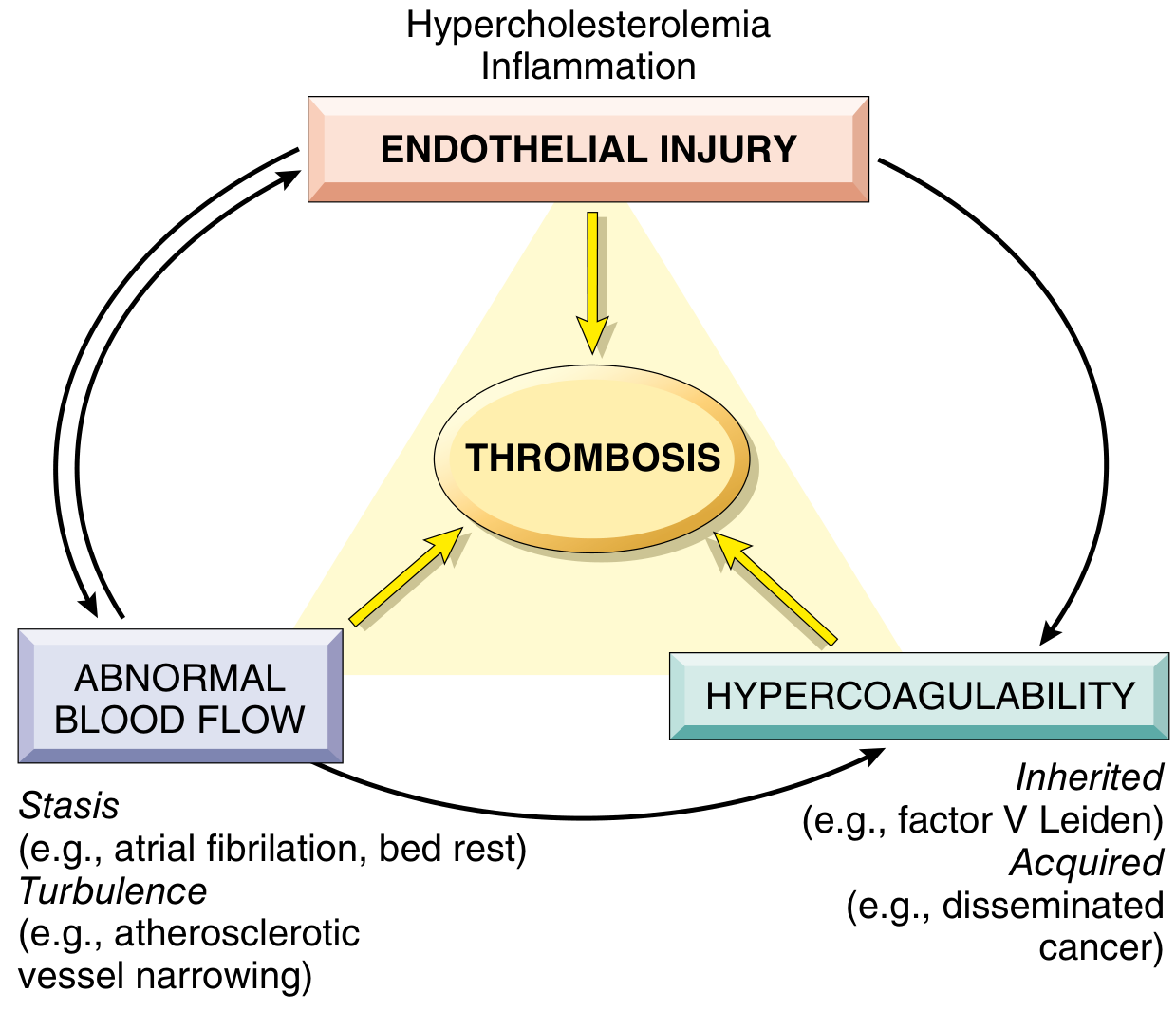
1. Endothelial Injury
The most important factor, especially for arterial and cardiac thrombosis where high flow rates impede clot formation. Platelet adherence and activation is a necessary prerequisite under high shear stress.
Mechanisms of injury:
- Physical injury, infectious agents, abnormal blood flow
- Inflammatory mediators and cytokines
- Metabolic abnormalities (hypercholesterolemia, homocystinemia)
- Toxins from cigarette smoke
Prothrombotic endothelial changes:
- Procoagulant changes: Downregulation of thrombomodulin, protein C, and tissue factor pathway inhibitor (TFPI) - shifts balance toward coagulation
- Antifibrinolytic effects: Secretion of plasminogen activator inhibitors (PAIs), reduced tissue plasminogen activator (t-PA) expression
- Platelet-activating effects: Increased expression of vWF and tissue factor
2. Abnormal Blood Flow (Stasis or Turbulence)
- Turbulence promotes arterial and cardiac thrombosis by causing endothelial injury/dysfunction
- Stasis is the dominant factor in venous thrombosis
Turbulence and stasis promote thrombosis by:
- Disrupting laminar flow, bringing platelets into contact with endothelium
- Preventing dilution of activated clotting factors by fresh blood
- Retarding influx of clotting factor inhibitors
- Promoting endothelial cell activation
Clinical examples:
- Atrial fibrillation - blood stasis in the atrial appendage
- Aneurysms - turbulence and stasis in the sac
- Atherosclerotic plaques - turbulence around stenoses
- Prolonged bed rest / immobility - venous stasis in lower limbs
- Hyperviscosity states (polycythemia, sickle cell disease)
3. Hypercoagulability
Defined as any alteration in the coagulation pathways that predisposes to thrombosis.
| Type | Examples |
|---|---|
| Primary (Inherited) | Factor V Leiden mutation (most common hereditary thrombophilia), Prothrombin gene mutation (G20210A), Antithrombin III deficiency, Protein C or S deficiency |
| Secondary (Acquired) | Prolonged bed rest/immobility, MI, atrial fibrillation, tissue damage (surgery, fracture), cancer (Trousseau syndrome), antiphospholipid antibody syndrome, HIT (heparin-induced thrombocytopenia), pregnancy, OCP use, nephrotic syndrome |
Morphology of Thrombi
Arterial thrombi (white thrombi):
- Rich in platelets and fibrin
- Typically at sites of endothelial injury (atherosclerotic plaques)
- Grow in a retrograde direction from point of attachment
- Show lines of Zahn - pale platelet/fibrin layers alternating with darker RBC-rich layers (pathognomonic of antemortem thrombus)
Venous thrombi (red/stasis thrombi):
- Rich in RBCs (hence "red")
- Occur in slower-flow venous circulation
- Most commonly in deep veins of lower extremity (DVT)
- Lines of Zahn are less distinct
Mural thrombi:
- In heart chambers or aortic lumen
- Post-MI (endocardial injury), atrial fibrillation (stasis), aortic aneurysm
Fate of a Thrombus
Thrombi have four possible fates:
| Fate | Description |
|---|---|
| Propagation | Accumulates more platelets and fibrin, enlarges |
| Embolization | Dislodges and travels to distant sites |
| Dissolution (lysis) | Fibrinolytic activity dissolves the clot (most desirable) |
| Organization and recanalization | Older thrombi become organized by ingrowth of endothelial cells, smooth muscle, fibroblasts; may eventually recanalize to restore flow |
Consequences of Thrombosis
- Local vascular occlusion - ischemia/infarction distal to the clot
- Distal embolization - thrombus fragment travels and blocks a distant vessel
- Venous congestion - in venous thrombosis, backup of blood causing edema, pain, and ulceration
EMBOLISM
An embolus is a detached intravascular solid, liquid, or gaseous mass that is carried by blood from its point of origin to a distant site, where it causes partial or complete vascular occlusion.
Most emboli are dislodged thrombi - hence the collective term thromboembolism.
Types of Emboli
1. Pulmonary Embolism (PE)
- Origin: 70-80% arise from deep vein thrombosis (DVT) of the legs
- Incidence: ~60-120 cases/100,000 per year (US); 60,000-100,000 deaths/year
- ~20% die before or shortly after diagnosis
Pathophysiology by size:
| Embolus Size | Effect |
|---|---|
| Large/massive | Occludes main pulmonary artery or saddle embolus at bifurcation → sudden death, acute cor pulmonale |
| Medium | Occludes a medium pulmonary artery → pulmonary hemorrhage (rarely infarction due to dual lung supply) |
| Small/multiple | Multiple small emboli over time → pulmonary hypertension, right heart failure |
| Paradoxical | Crosses patent foramen ovale → systemic embolization |
Pulmonary infarction occurs in <10% because the lung has a dual blood supply (pulmonary + bronchial arteries). It occurs when bronchial flow is also compromised (left heart failure, pneumonia).
Clinical features:
- Pleuritic chest pain, dyspnea, tachycardia, hemoptysis
- Large emboli: sudden-onset shock, right heart failure
- Multiple small emboli: progressive dyspnea, pulmonary HTN
2. Systemic Thromboembolism
- Most arise from intracardiac mural thrombi (2/3 associated with left ventricular MI; 25% with dilated left atrium in atrial fibrillation)
- Also from aortic aneurysms, ulcerated atherosclerotic plaques, valvular vegetations
- Travel to: legs (most common ~75%), brain, intestines, kidneys, spleen
3. Fat Embolism
- Source: Fat globules from bone marrow after fracture of long bones (femur, tibia) or severe burns
- Enters pulmonary circulation via torn marrow vessels
- Fat embolism syndrome: Occurs 1-3 days after injury
- Pulmonary insufficiency (dyspnea, tachypnea)
- Neurological symptoms (irritability, restlessness, coma)
- Petechial rash (thrombocytopenia + anemia)
- Mortality: ~10%
4. Air Embolism
- Gas bubbles in the circulation obstruct flow
- Can occur from entry of air during surgery (neurosurgical, cardiac), obstetric procedures, IV catheter placement, chest trauma
- Decompression sickness (Caisson disease): Rapid decompression from high-pressure environments causes nitrogen gas bubbles to form in tissues and blood
- Acute: bends (joint pain), chokes (pulmonary symptoms)
- Chronic: aseptic necrosis of bone (especially femoral head)
5. Amniotic Fluid Embolism
- Rare but catastrophic obstetric complication
- Amniotic fluid (with fetal cells, hair, vernix) enters maternal circulation through uterine tears or ruptured cervical veins
- Triggers: pulmonary vascular obstruction, anaphylactoid reaction, DIC
- Mortality: up to 80%
6. Cholesterol (Atheroembolism)
- Showers of cholesterol crystals from ulcerated atherosclerotic plaques
- Affects small arteries of kidneys, brain, extremities
- Often triggered by arterial catheterization
Comparison: Thrombosis vs. Embolus
| Feature | Thrombus | Embolus |
|---|---|---|
| Definition | Clot formed in situ | Detached mass traveling in blood |
| Composition | Platelets, fibrin, RBCs | Usually dislodged thrombus; can be fat, air, tumor |
| Formation | Virchow's triad (injury, stasis, hypercoag) | Usually from thrombosis elsewhere |
| Attachment | Attached to vessel wall | Not attached - free-floating |
| Lines of Zahn | Present (arterial) | Absent |
| Location | Where formed | Distal, at branch points or narrowings |
| Consequence | Local occlusion, embolism | Distal infarction/obstruction |
Key points to remember:
- Virchow's triad (endothelial injury, stasis/turbulence, hypercoagulability) underlies all thrombosis
- Arterial thrombi = platelet-rich, white; venous thrombi = RBC-rich, red
- Lines of Zahn distinguish antemortem thrombus from postmortem clot
- PE is the most common and clinically significant form of embolism
- Fat embolism presents 1-3 days post-fracture with the triad of respiratory failure, neurologic symptoms, and petechiae
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 126-137
This is a shared conversation. Sign in to Orris to start your own chat.