About Preeclampsia
Reading File
Finding Sources
Searching PubMed
"preeclampsia"[MeSH Terms] AND management
Searching the Web
preeclampsia 2024 2025 guidelines diagnosis management
Reading File
Reading File
Finding Sources
Searching PubMed
"preeclampsia"[MeSH Terms] AND "pathogenesis"
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
preeclampsia pathophysiology placental ischemia angiogenic factors diagram
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Preeclampsia
Definition & Epidemiology
Preeclampsia is a pregnancy-specific disorder defined as new-onset hypertension (BP ≥140/90 mmHg on two occasions ≥4 hours apart) after 20 weeks of gestation, accompanied by proteinuria (≥300 mg protein/24-hour urine, or protein:creatinine ratio ≥0.3) or signs of end-organ damage in the absence of proteinuria.
- Affects 5–7% of all pregnancies globally
- A leading cause of maternal and perinatal morbidity/mortality worldwide
- In the absence of treatment, ~1 in 100 cases progresses to eclampsia (generalized tonic-clonic seizures)
Harrison's Principles of Internal Medicine 22E, p. 3942; Creasy & Resnik's Maternal-Fetal Medicine, pp. 1055–1140
Diagnostic Criteria
Hypertension
- Systolic BP ≥140 mmHg OR diastolic BP ≥90 mmHg on two readings ≥4 hours apart
- An incremental rise of 30 mmHg systolic / 15 mmHg diastolic is no longer part of the diagnostic criteria (no increased adverse outcome risk in this group)
Proteinuria (any one of):
- ≥300 mg protein in 24-hour urine collection
- Protein:creatinine ratio ≥0.3
- Dipstick 2+ (only if quantitative methods unavailable — false positives/negatives common)
Without proteinuria, preeclampsia is diagnosed if hypertension co-exists with:
| Finding | Threshold |
|---|---|
| Thrombocytopenia | Platelets <100,000/μL |
| Elevated transaminases | >2× upper limit of normal |
| Renal insufficiency | Creatinine >1.1 mg/dL (no other renal disease) |
| Pulmonary edema | Clinical/radiological |
| New-onset cerebral or visual disturbances | — |
Creasy & Resnik's Maternal-Fetal Medicine, p. 1055
Severe Features
The diagnosis of preeclampsia with severe features requires any of the following:
- BP ≥160/110 mmHg on two occasions ≥4 hours apart (unless antihypertensives already initiated)
- New-onset cerebral or visual disturbances
- Pulmonary edema
- Persistent epigastric or RUQ pain unresponsive to medication
- Liver enzymes >2× normal
- Thrombocytopenia (platelets <100,000/μL)
- Progressive renal insufficiency (creatinine >1.1 mg/dL)
⚠️ ACOG recommends abandoning the term "mild" preeclampsia — even without severe features, significant morbidity and mortality risk remain.
Pathophysiology
The precise mechanism remains incompletely understood but involves several converging pathways:
1. Abnormal Placentation & Uteroplacental Ischemia
- Defective trophoblastic invasion of spiral arteries → failure of normal vascular remodeling → high-resistance, low-flow uteroplacental circulation
- Placental ischemia is the primary driver
2. Angiogenic Imbalance
- Excess production of sFlt-1 (soluble fms-like tyrosine kinase 1) — an anti-angiogenic factor
- Decreased PlGF (placental growth factor) — a pro-angiogenic factor
- sFlt-1/PlGF ratio ≥40 is associated with increased risk of developing severe features within 2 weeks
- sFlt-1 acts by binding and neutralizing VEGF and PlGF → endothelial dysfunction
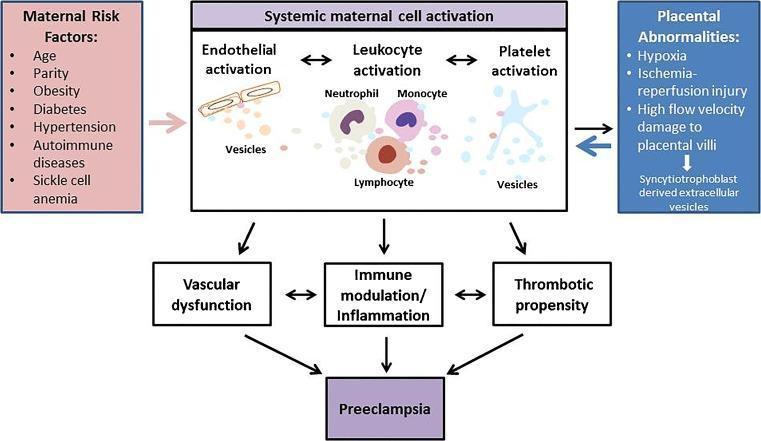
3. Endothelial Dysfunction & Systemic Inflammation
- Endothelial activation → increased vascular permeability, vasospasm
- Leukocyte activation (neutrophils, monocytes) and platelet activation
- Exaggerated maternal inflammatory response with pro-inflammatory cytokines
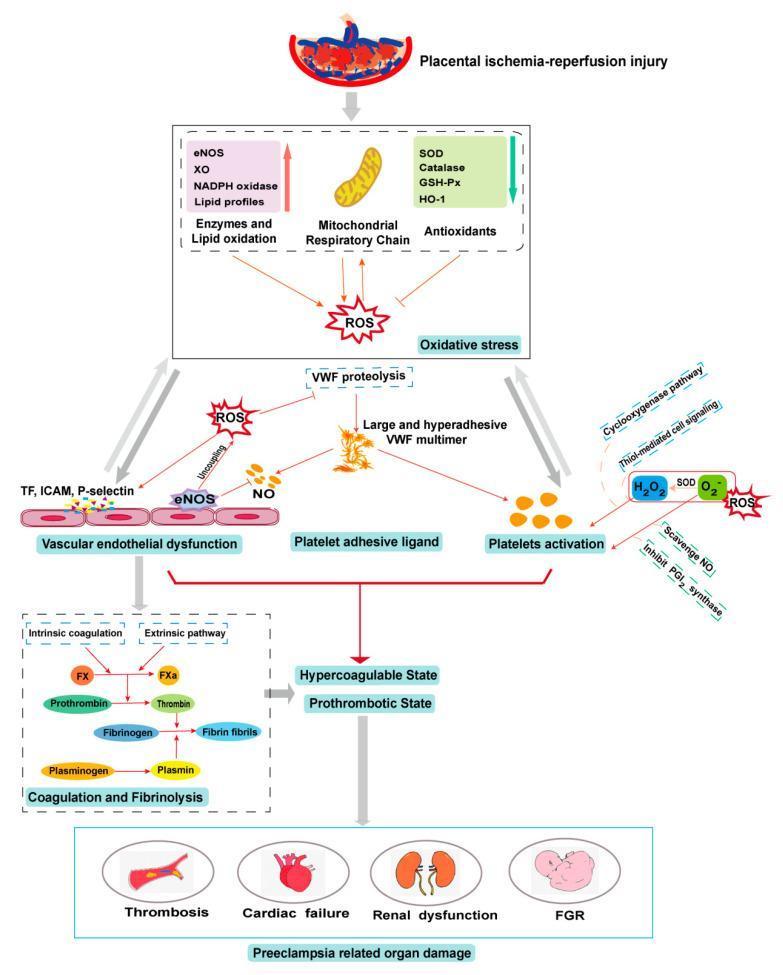
4. Oxidative Stress
- Reactive oxygen species (ROS) from NADPH oxidase, eNOS uncoupling, mitochondrial dysfunction
- Lipid peroxidation and large VWF multimer formation → prothrombotic state
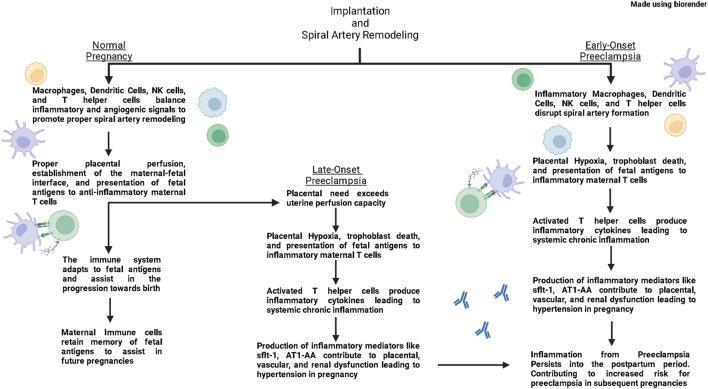
5. Immunological Mechanisms
- Impaired HLA-G/HLA-C interactions between extravillous trophoblasts and maternal NK cells/macrophages → deficient spiral artery remodeling
- Early-onset preeclampsia (before 34 weeks): dominated by defective placentation
- Late-onset preeclampsia (≥34 weeks): normal initial remodeling, but placental demands exceed uterine perfusion capacity over time
Barash, Cullen & Stoelting's Clinical Anesthesia 9e, p. 3508; Creasy & Resnik's Maternal-Fetal Medicine, p. 1060; Harrison's 22E, p. 3942
Organ-System Pathology
Neurological
- Loss of cerebral vascular autoregulation → focal hypoperfusion despite elevated MAP
- Posterior Reversible Encephalopathy Syndrome (PRES): vasogenic, parietooccipital edema — typically reversible
- Petechial hemorrhage after convulsions
- White matter lesions and cognitive dysfunction in long-term follow-up
- Symptoms: headache, blurred vision, scotomata, diplopia, hyperreflexia, cortical blindness, convulsions
- Cerebral hemorrhage is a leading cause of death
Liver
- Gross lesions visible in 60% of eclamptic women
- Periportal hemorrhage (early) → hepatic infarction (late, from intense vasospasm)
- HELLP syndrome: Hemolysis, Elevated Liver enzymes, Low Platelets — a severe subtype with high morbidity
Kidney
- Glomerular endotheliosis (pathognomonic lesion): enlarged endothelial cells occlude capillary lumens, reduced GFR
- Glomerular changes include decreased size, reduced capillary diameter, increased cytoplasmic endothelial-mesangial volume
- Results in proteinuria, oliguria, anuria, and rising creatinine
Cardiovascular
- Hypovolemia paradoxically (fluid shifts from intravascular to extravascular space)
- Mean plasma volume up to 30–40% below normal in severe disease
- Pulmonary edema in ~2% of severe cases (from fluid overload, cardiac failure, aspiration, or magnesium sulfate)
- Airway edema — important for anesthetic management (risk of difficult intubation)
Hematologic
- Thrombocytopenia (platelets 100–150 × 10⁹/L typically)
- Elevated fibrin degradation products; fibrinogen usually normal (unless abruption)
- PT/PTT prolongation indicates consumption of procoagulant factors
Metabolic
- Exaggerated insulin resistance → elevated triglycerides, LDL, fatty acids; reduced HDL
- These changes may predate clinical disease and resolve postpartum
Fetal
- Reduced placental intervillous blood flow → chronic fetal hypoxia
- IUGR, preterm birth, increased perinatal mortality — risks correlate with severity
Risk Factors
| Category | Risk Factors |
|---|---|
| Prior history | Previous preeclampsia (strongest risk factor) |
| Medical conditions | Chronic hypertension, renal disease, DM (especially with vascular disease), SLE, antiphospholipid syndrome |
| Obstetric | Nulliparity, multiple gestation (twin 6.7%, triplet 12.7%, quadruplet 20%), molar pregnancy |
| Body habitus | Obesity (3× risk — linear relationship with BMI) |
| Other | Advanced maternal age, donor oocyte pregnancies, new paternity |
Creasy & Resnik's Maternal-Fetal Medicine, pp. 1056–1058
HELLP Syndrome
A severe subtype of preeclampsia with:
- Hemolysis (microangiopathic hemolytic anemia)
- Elevated liver enzymes (transaminases >2× normal)
- Low platelets (<100,000/μL)
Complications: coagulopathy, CVAs, hepatic capsule rupture, placental abruption, DIC.
Eclampsia
- Preeclampsia + new-onset generalized tonic-clonic seizures with no other identified cause
- Occurs in ~1% of untreated preeclampsia cases
- Risk of seizures correlates poorly with BP level
- Managed with magnesium sulfate (first-line anticonvulsant and seizure prophylaxis)
Management
Definitive Treatment
Delivery of the fetus and placenta — the only cure.
Delivery Timing by Severity
| Scenario | Recommendation |
|---|---|
| Without severe features | Delivery at 37 weeks (expectant management until then) |
| With severe features ≥34 weeks | Delivery indicated |
| With severe features <34 weeks | Expectant management in tertiary center if no indications for earlier delivery |
| Indications for delivery before 34 weeks | Unrelenting symptoms, lab deterioration, refractory severe BP, severe IUGR, abruption |
Antihypertensive Therapy
- Goal: prevent cerebral hemorrhage, myocardial ischemia, renal injury while maintaining uteroplacental flow
- ACOG: treat BP ≥160/110 mmHg within 30–60 minutes
| Drug | Route | Notes |
|---|---|---|
| Labetalol | IV | First-line for acute management |
| Hydralazine | IV | First-line for acute management |
| Nifedipine (extended-release) | Oral | Acute or maintenance |
- ACE inhibitors / ARBs are contraindicated (stillbirth, fetal anomalies)
Seizure Prophylaxis & Treatment
- Magnesium sulfate (MgSO₄) — standard of care for seizure prevention in severe preeclampsia and treatment of eclampsia
- Loading dose 4–6 g IV, then maintenance 1–2 g/hr
Expectant Management Components
- Frequent BP monitoring and lab surveillance
- Serial fetal surveillance (biophysical profile, umbilical artery Doppler)
- Limited physical activity
- Corticosteroids (betamethasone 12 mg IM × 2 doses) if delivery anticipated before 34 weeks
Aspirin Prophylaxis
- Low-dose aspirin 81 mg/day initiated between 12–16 weeks (by 28 weeks at the latest)
- Recommended for high-risk women
- Reduces preeclampsia incidence by ~50% in diabetic women; reduces IUGR by ~20%
- Endorsed by ACOG, SMFM, and ADA
Long-Term Consequences
Women with prior preeclampsia have significantly elevated long-term risks:
- Chronic hypertension
- Cardiovascular disease (2–4× increased risk)
- Chronic kidney disease
- Diabetes mellitus
- White matter lesions and cognitive dysfunction
Cardiovascular risk-reduction interventions should be initiated at postpartum health encounters.
Harrison's 22E, p. 3942; Barash, Cullen & Stoelting's Clinical Anesthesia 9e, pp. 3508–3512
Summary Table: Preeclampsia vs Severe Features
| Feature | Without Severe Features | With Severe Features |
|---|---|---|
| BP | 140–159 / 90–109 mmHg | ≥160/110 mmHg |
| Proteinuria | ≥300 mg/24h | Any amount |
| Platelets | Normal | <100,000/μL |
| Creatinine | Normal or mildly elevated | >1.1 mg/dL |
| Liver enzymes | Normal or mildly elevated | >2× ULN |
| CNS symptoms | None | Headache, visual changes |
| Pulmonary edema | Absent | Present |
| Delivery timing | 37 weeks | Immediate or ≥34 weeks |
Sources: Creasy & Resnik's Maternal-Fetal Medicine, 8e; Harrison's Principles of Internal Medicine 22E; Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Goldman-Cecil Medicine, International Ed.
This is a shared conversation. Sign in to Orris to start your own chat.