Here is a comprehensive structured answer to all five questions.
Clinical Case Analysis: 39-Year-Old Man with Recurrent Chest Pain
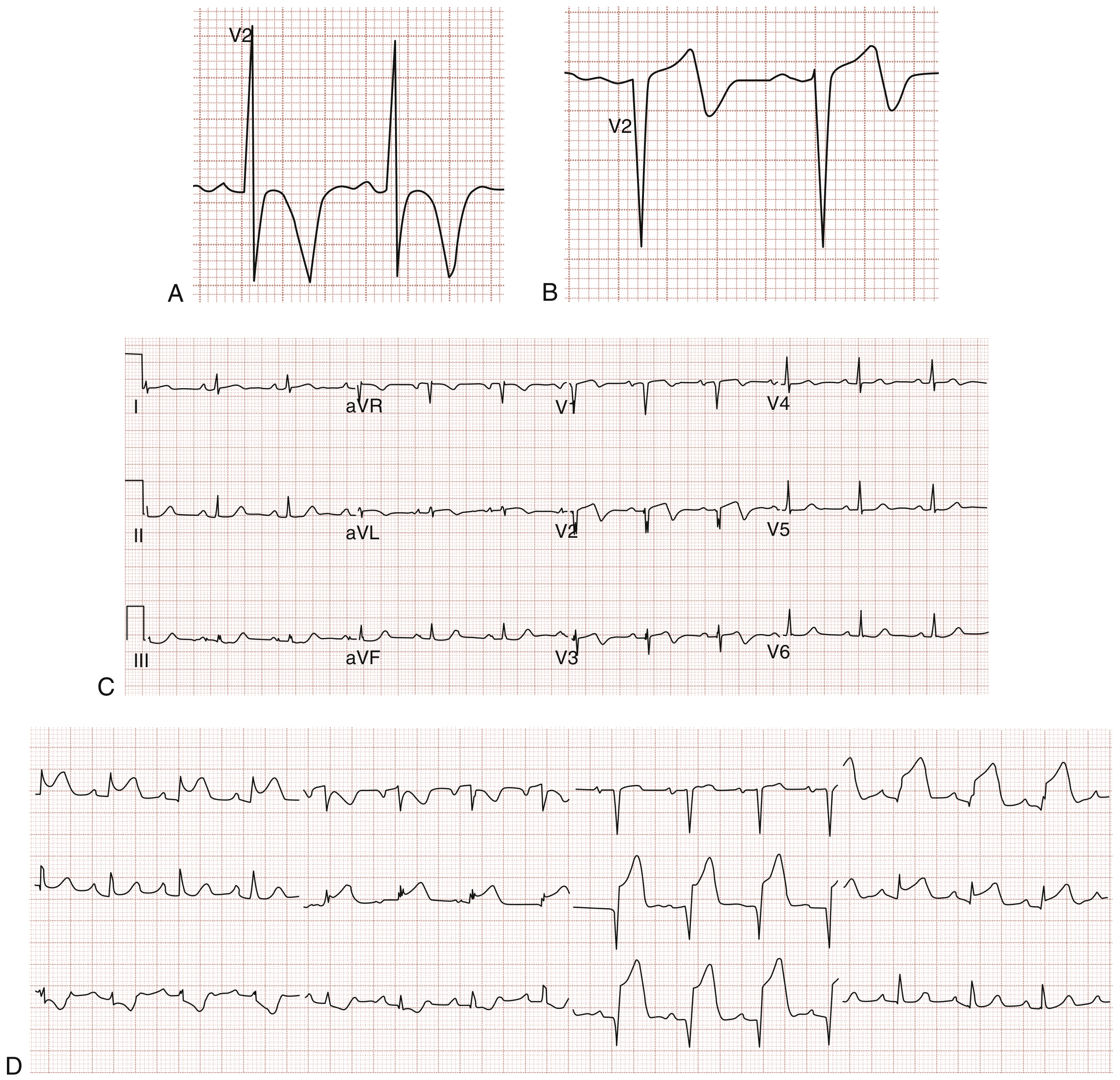
ECG Reference: Wellens Syndrome Patterns
Panels A & B show Type A (biphasic) and Type B (deeply inverted) T waves in Wellens syndrome. Panel C: pain-free patient with biphasic T waves in V2-V3. Panel D: same patient 6 hours later with extensive anterolateral STEMI requiring emergency PCI for proximal LAD occlusion. - Rosen's Emergency Medicine
Question 1: Main Diagnosis, Leading Syndrome, Concomitant Diseases, Complications, and Differential Diagnosis
Leading Syndrome
Acute Coronary Syndrome (ACS) - specifically Unstable Angina / Pre-infarction state, manifested by:
- Recurrent central chest pain at rest and with minimal exertion
- Pain not relieved by standard therapy (ranitidine ineffective)
- High-risk ECG pattern (Wellens syndrome - see Q4)
- Multiple cardiovascular risk factors
Main Diagnosis (Structured Format)
Main Diagnosis:
Unstable angina / Wellens syndrome - critical proximal LAD stenosis presenting as a pre-infarction state (ACS without ST-elevation, NSTE-ACS)
- Classification by ACS type: NSTE-ACS (unstable angina, cTnI negative x2)
- GRACE risk score: High-risk (age 39 + multiple risk factors + ECG changes + recurrent symptoms)
- Canadian Cardiovascular Society (CCS) class: Class III-IV (symptoms at minimal exertion and at rest)
- Braunwald classification of Unstable Angina: Class IIIB (rest angina, >48 hours, no precipitating cause)
Concomitant Diseases:
- Arterial hypertension (BP 145/80 mmHg, untreated)
- Active smoking (20 cigarettes/day - 20 pack-year history)
- Family history of premature CAD (father MI at age 41)
- Likely insulin resistance / pre-diabetes (South Asian ethnicity + family history of diabetes)
Complications:
- At risk for: Anterior STEMI (proximal LAD occlusion), cardiogenic shock, malignant arrhythmia, sudden cardiac death - the Wellens pattern identifies this patient as having a time-critical pre-infarction state
Differential Diagnosis: 3 Diseases
1. Gastro-oesophageal Reflux Disease (GERD) - Already diagnosed on 2nd visit
Arguments FOR: Burning, central, lower chest pain; no radiation; no exertional pattern clearly documented; age-appropriate; tried ranitidine.
Arguments AGAINST (why it is NOT the primary diagnosis):
- Ranitidine 150 mg BD gave no relief across 3 weeks
- The ECG now shows deep T-wave inversions in V2-V5 - GERD does not produce precordial T-wave changes
- High cardiovascular risk profile (South Asian, family history premature CAD, hypertension, smoking) makes cardiac ischemia statistically far more likely
- The pain is not clearly postprandial, positional, or relieved by antacids
- GERD diagnosis should never be accepted until cardiac causes are fully excluded in a high-risk patient - Fuster & Hurst's The Heart, 15th ed.
2. Pulmonary Embolism (PE)
Arguments FOR: Central chest pain, no exertional pattern clearly tied to it, normal troponin initially.
Arguments AGAINST:
- No pleuritic quality, no dyspnoea, no tachycardia (HR 75), O2 sat 98%
- No risk factors for VTE (no immobility, surgery, malignancy, long-haul travel)
- ECG does not show S1Q3T3 pattern or right heart strain; instead shows anterior precordial T-wave changes pointing to LAD territory ischemia
- Three-week history without haemodynamic deterioration is atypical for significant PE
3. Aortic Dissection
Arguments FOR: Hypertension (145/80), central chest pain, male.
Arguments AGAINST:
- Pain is NOT tearing/ripping in character, NOT sudden-onset maximal from the start
- Does NOT radiate to the back
- BP equal bilaterally (implied by single BP reading, no pulse deficit described)
- Recurrent 3-week history is incompatible with untreated aortic dissection (which is rapidly lethal if untreated)
- ECG changes are anterior ischemic, not the diffuse non-specific changes of dissection
Question 2: Description of Typical Angina
Typical (classic) angina is defined by all three of the Diamond-Forrester criteria:
- Substernal pressure-like discomfort - described as squeezing, heavy, burning, or tightness in the central chest; patients often deny "pain" and use terms like "pressure," "ache," or "tightness"
- Precipitated by exertion or emotional stress - due to increased myocardial oxygen demand exceeding supply across a fixed atherosclerotic obstruction
- Relieved by rest or sublingual nitroglycerin within 5 minutes
Additional features of stable typical angina:
- Duration typically 2-5 minutes, rarely more than 15 minutes
- May radiate to the left arm, jaw, neck, or shoulder
- Reproducible threshold - the same degree of exertion consistently triggers pain
- Worsened by cold, heavy meals, emotional upset
- Atypical presentations (nausea, diaphoresis, fatigue without chest pain) are more common in women, diabetics, and the elderly
When only two criteria are present = atypical angina. When only one criterion = non-cardiac chest pain. - Fuster & Hurst's The Heart, 15th ed.
This patient's pain is atypical: burning, central, not clearly exertional, not relieved by nitroglycerin. However, atypical presentations do NOT exclude ischemia, especially in high-risk demographics.
Question 3: ECG Findings (Fig. 4.1)
Analyzing the patient's admission ECG:
| Finding | Detail |
|---|
| Rhythm | Sinus rhythm, regular at ~75 bpm |
| Rate | ~75 bpm |
| Axis | Normal |
| P waves | Present, normal morphology |
| PR interval | Normal (~160 ms) |
| QRS | Narrow, no bundle branch block |
| ST segments | No significant ST elevation or depression |
| T waves | Deep, symmetric T-wave inversions in V2, V3, V4 (and extending into V5); upright T waves in V1 |
| Q waves | No pathological Q waves |
Key abnormality: Deep, symmetric T-wave inversions in the anterior precordial leads (V2-V5), present in a pain-free patient with a recent history of chest pain. This is the defining feature of Wellens syndrome.
Question 4: Differential Diagnosis of the ECG Findings and Most Likely Diagnosis
Differential Diagnosis for Anterior T-wave Inversions
| Cause | Features that distinguish |
|---|
| Wellens syndrome | Deep symmetric inversions V2-V5, pain-free at time of ECG, prior ischemic chest pain, no troponin rise |
| NSTEMI (resolving) | Troponin would be elevated; T-wave inversions follow ST changes |
| Post-reperfusion changes | Follows STEMI + PCI; not applicable here |
| Left ventricular hypertrophy (LVH) | Voltage criteria met, strain pattern in lateral leads; associated with hypertension |
| Right ventricular strain / PE | S1Q3T3 pattern, sinus tachycardia, T inversions in V1-V3 |
| Myocarditis / pericarditis | Diffuse changes, saddle-shaped ST elevation, pleuritic features, younger patient, viral prodrome |
| Hypertrophic cardiomyopathy | Marked LVH voltage, septal hypertrophy on echo |
| Cerebrovascular accident | Widespread deep T inversions, QT prolongation, no ischemic history |
| Benign T-wave variant (juvenile pattern) | Persistent in young patients V1-V3, no ischemic symptoms |
Most Likely Diagnosis: Wellens Syndrome (Type B)
This is the most important and most likely diagnosis in this context:
- Definition: Wellens syndrome is a specific ECG pattern of T-wave changes in leads V2-V3 (often extending to V4-V5) that represents critical stenosis of the proximal left anterior descending artery (LAD) during a pain-free interval between ischemic episodes
- Type A (25%): Biphasic T waves (initially positive then negative) in V2-V3
- Type B (75%): Deep, symmetric T-wave inversions in V2-V3 - this patient has Type B
- The T-wave changes occur during the pain-free interval - this is the hallmark and is exactly what is seen here (patient is "anxious but pain free" on examination)
- Troponin is typically negative or minimally elevated because these changes reflect reperfused ischemia, not completed infarction
- This ECG pattern predicts imminent anterior STEMI if the LAD occludes completely. Up to 75% of untreated Wellens patients progress to extensive anterior MI. - Rosen's Emergency Medicine
Why this was missed on previous visits: The ECG on previous visits was read as normal. Wellens changes may be subtle, intermittent, and require comparison across serial ECGs in the context of the clinical story.
Question 5: Most Correct Next Management Step
Immediate Actions (Emergency Management)
This patient must be admitted immediately to a cardiac care unit. Stress testing and exercise ECG are absolutely contraindicated - they risk precipitating complete LAD occlusion.
Step 1 - Immediate Stabilisation
| Intervention | Details |
|---|
| Monitoring | Continuous cardiac monitoring, 12-lead ECG every 30 min initially |
| IV access | Large-bore IV x2 |
| Oxygen | Only if SpO2 <94% (currently 98%, not indicated) |
| Bed rest | Complete bed rest; avoid exertion |
| Serial ECGs | Every 30-60 minutes and with any recurrence of pain |
| Repeat troponin | High-sensitivity troponin at 0h/1h/3h |
Step 2 - Antiplatelet Therapy (Dual)
| Drug | Dose |
|---|
| Aspirin | 300 mg oral loading dose immediately, then 75-100 mg daily |
| Ticagrelor (preferred over clopidogrel in ACS) | 180 mg loading dose, then 90 mg twice daily |
| OR Clopidogrel (if ticagrelor unavailable) | 600 mg loading dose, then 75 mg daily |
Step 3 - Anticoagulation
| Drug | Dose |
|---|
| Enoxaparin (preferred LMWH) | 1 mg/kg SC twice daily (or 0.75 mg/kg if age >75) |
| OR Unfractionated Heparin | 60-70 units/kg IV bolus (max 5000 units), then 12-15 units/kg/hour infusion, adjusted to aPTT 50-70 seconds |
Enoxaparin plus aspirin has demonstrated superiority over UFH plus aspirin in reducing death, MI, and recurrent angina in UA/NSTEMI (ESSENCE trial). - Textbook of Family Medicine, 9th ed.
Step 4 - Anti-ischemic Therapy
| Drug | Dose |
|---|
| Sublingual GTN (if chest pain recurs) | 0.4 mg SL, repeat every 5 min x3; then IV nitrate if persistent |
| IV Nitroglycerin (if ongoing pain) | 5-10 mcg/min, titrate up by 10 mcg/min every 3-5 min to pain relief |
| Beta-blocker (if no contraindication: no bronchospasm, no decompensated HF, HR >60) | Metoprolol succinate 25-50 mg oral twice daily (or 5 mg IV slowly if urgent) |
| High-intensity statin | Atorvastatin 80 mg once daily (immediately, regardless of lipid levels) |
Step 5 - Urgent Coronary Angiography + PCI
This is the definitive and most important step.
- Wellens syndrome mandates urgent invasive strategy - coronary angiography within 24-48 hours (or immediately if pain recurs or haemodynamic deterioration)
- Expected finding: critical proximal LAD stenosis (typically >90%)
- Treatment: Percutaneous Coronary Intervention (PCI) with drug-eluting stent (DES) to the proximal LAD
- If anatomy is unsuitable for PCI: Coronary Artery Bypass Grafting (CABG) referral
Step 6 - Other Medications
| Drug | Indication | Dose |
|---|
| ACE inhibitor | Hypertension (BP 145/80) | Ramipril 2.5-5 mg daily, titrate up |
| Ranitidine | Discontinue - was the wrong diagnosis; if GI protection needed, use PPI (omeprazole 20 mg daily) with dual antiplatelet | |
| Smoking cessation | Immediate | Nicotine replacement or varenicline after stabilisation |
Medications to AVOID in Wellens Syndrome
- Stress testing / exercise ECG - absolutely contraindicated, can precipitate complete LAD occlusion and massive anterior MI
- Dobutamine stress echo - also contraindicated
- Discharge on medical management alone without angiography - high mortality risk
Question 5 (Part B): Specialist Referral
| Specialist | Purpose |
|---|
| Interventional Cardiologist (urgent, same-day) | Emergency coronary angiography and PCI of the proximal LAD; this is the primary and most urgent referral |
| Cardiac Surgeon | Standby or formal referral if PCI is anatomically not feasible (left main disease, three-vessel disease) - CABG planning |
| Smoking Cessation Clinic / Respiratory Physician | Structured smoking cessation (nicotine replacement, varenicline) after cardiac stabilisation |
| Diabetologist / Endocrinologist | Formal assessment for diabetes / metabolic syndrome given South Asian ethnicity, family history of diabetes, and hypertension |
| Cardiac Rehabilitation | Post-PCI structured exercise, risk factor modification, psychological support |
Summary: Key Clinical Pearls in This Case
- Never accept a GI diagnosis in a high-risk chest pain patient without a normal ECG - this patient had anterior T-wave changes that signalled impending LAD occlusion
- Wellens syndrome is a pre-infarction state - normal troponins and pain-free state make it deceptively reassuring, but it carries a very high risk of anterior STEMI
- South Asian men have a 3-4x higher risk of premature CAD than the white European population - the age of 39 is not reassuring in this ethnicity
- Family history of MI at 41 pushes the pre-test probability of significant CAD very high
- Stress testing is contraindicated - the correct next step is urgent angiography, not more non-invasive testing
Sources: Rosen's Emergency Medicine; Fuster & Hurst's The Heart, 15th ed.; Lippincott Illustrated Reviews Pharmacology; Textbook of Family Medicine 9th ed.; Robbins & Cotran Pathologic Basis of Disease