Give a detailed explanation about femurs in the point of view of greys anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I have comprehensive content from Gray's Anatomy for Students. Now let me compile the full, detailed response.
The Femur - Gray's Anatomy for Students
The femur is the bone of the thigh and the longest bone in the body. It extends from the hip joint above to the knee joint below, and its anatomy is best understood by dividing it into three parts: the proximal end, the shaft, and the distal end.
1. Proximal Femur
Head
The head of the femur is spherical and articulates with the acetabulum of the pelvic bone to form the hip joint - a multiaxial ball-and-socket joint designed for stability and weight-bearing at the expense of mobility. Almost the entire head is covered with hyaline cartilage, except for a small nonarticular pit on its medial surface called the fovea, which serves as the attachment point for the ligament of the head (ligamentum teres). This ligament carries a small branch of the obturator artery (the artery of the ligamentum teres), contributing to the blood supply of the femoral head.
Neck
The neck of the femur is a cylindrical strut of bone connecting the head to the shaft. It projects superomedially from the shaft at an angle of approximately 125 degrees and also projects slightly forward (anteversion). This angulation is biomechanically significant: it increases the range of movement at the hip joint by effectively lengthening the lever arm. The neck is also the site of some of the most clinically important fractures in older adults.
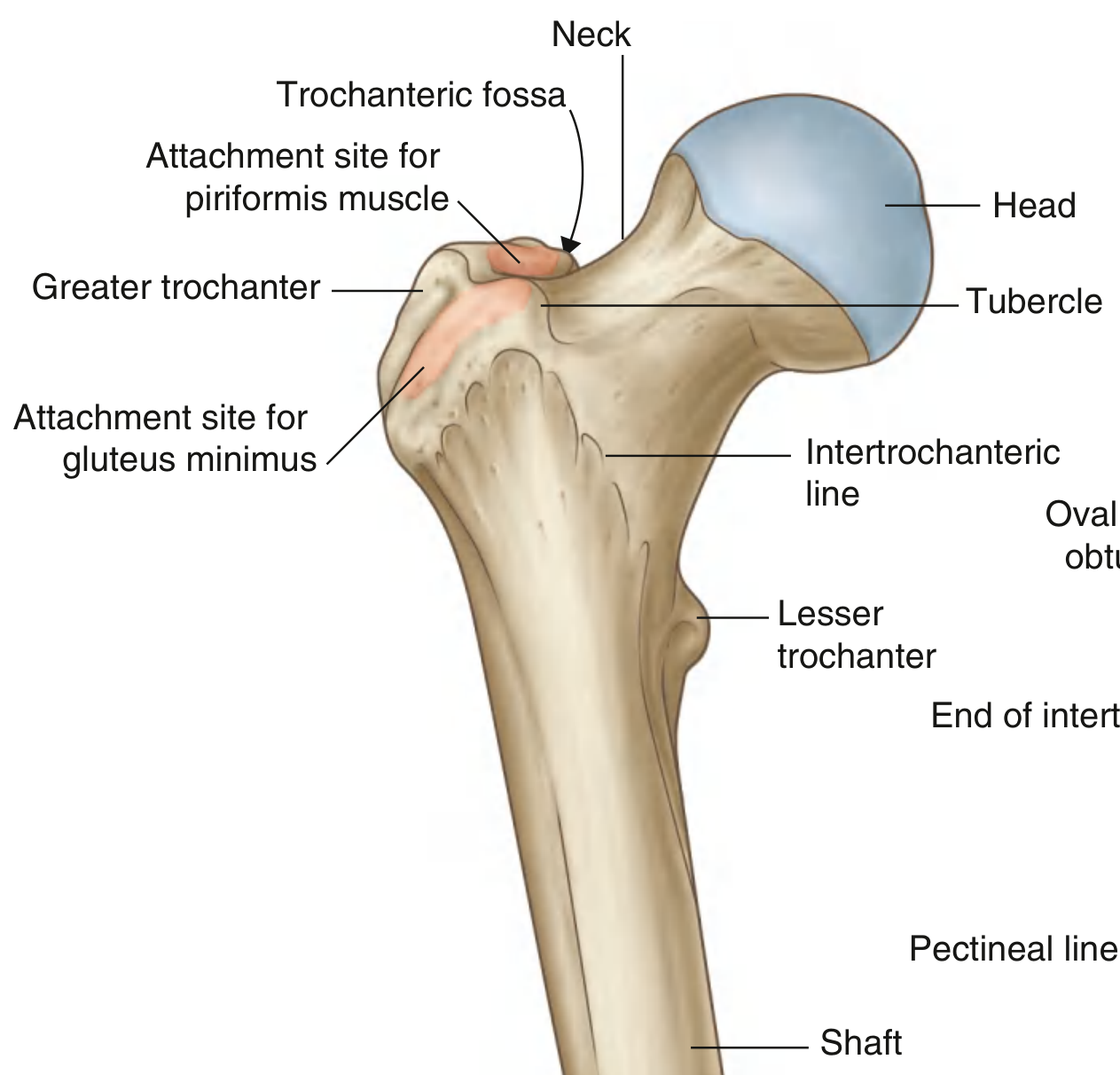
Greater Trochanter
The greater trochanter extends superiorly from the shaft just lateral to the neck-shaft junction. Posteriorly, its medial surface is deeply grooved to form the trochanteric fossa. The lateral wall of this fossa has an oval depression for the obturator externus muscle. On the anterolateral surface of the greater trochanter there is an elongate ridge for gluteus minimus, and a similar ridge posteriorly for gluteus medius. Just above the trochanteric fossa, there is an impression for obturator internus and the gemelli muscles, and slightly above and behind this, an impression for piriformis.
Lesser Trochanter
The lesser trochanter is smaller, blunt, and conical, projecting posteromedially from the shaft just inferior to the neck-shaft junction. It is the attachment site for the combined tendons of psoas major and iliacus (iliopsoas). Because psoas major's normal fulcrum is the femoral head within the acetabulum, disruption of the femoral neck (as in a fracture) causes the iliopsoas to pull the femur proximally and into external rotation - a key clinical sign.
Intertrochanteric Line and Crest
Extending between the two trochanters and separating the shaft from the neck are:
- The intertrochanteric line (anteriorly): a ridge descending medially from a tubercle at the base of the greater trochanter to just anterior to the lesser trochanter. It is continuous with the pectineal line (spiral line), which wraps around to merge with the medial margin of the linea aspera.
- The intertrochanteric crest (posteriorly): a broad smooth ridge on the posterior surface, bearing a prominent quadrate tubercle on its upper half, which is the attachment for the quadratus femoris muscle.
2. Shaft of the Femur
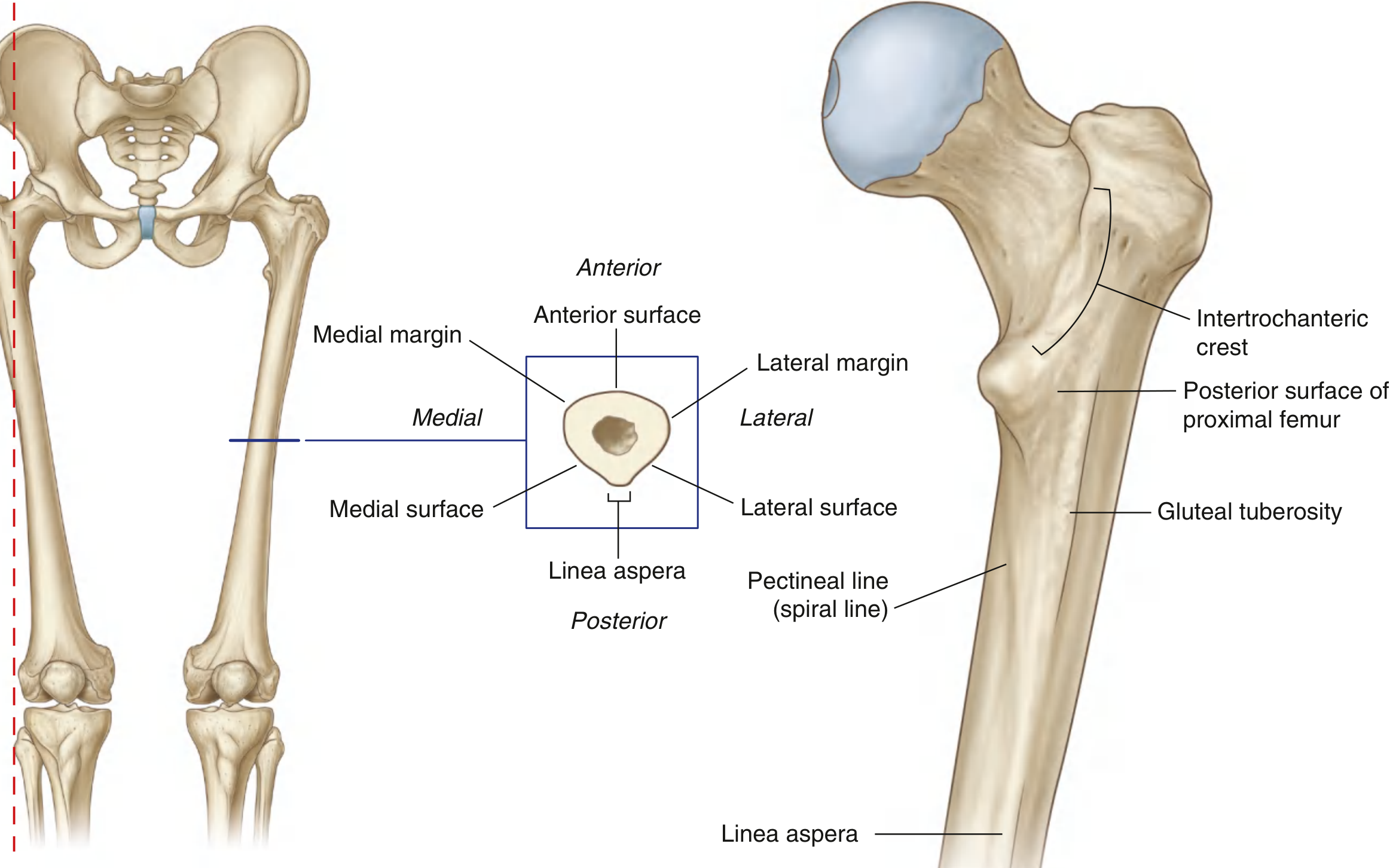
The shaft descends from lateral to medial in the coronal plane at an angle of 7 degrees from the vertical axis. Because of this oblique course, the distal femur is closer to the midline than the proximal end, placing the knee directly under the body's center of gravity. The shaft also bows slightly forward.
In cross section, the middle third is triangular, with:
- An anterior surface
- A lateral (posterolateral) surface
- A medial (posteromedial) surface
- Medial and lateral (rounded) margins
- A prominent posterior margin forming the linea aspera
Linea Aspera
The linea aspera is a broad, roughened longitudinal crest on the posterior surface of the shaft and is the major site of muscle attachment in the thigh. In the proximal third, its medial and lateral margins diverge:
- The medial margin continues as the pectineal line, curving anteriorly under the lesser trochanter.
- The lateral margin continues as the gluteal tuberosity, curving out to the base of the greater trochanter and providing attachment for gluteus maximus.
The triangular posterior surface of the proximal femur is bounded by the pectineal line, the gluteal tuberosity, and the intertrochanteric crest.
3. Distal Femur
The distal end is characterized by two large condyles (medial and lateral) that articulate with the proximal tibia. Key features include:
- Intercondylar fossa: a deep notch posteriorly separating the condyles. Its walls carry two small facets for the superior (femoral) attachments of the cruciate ligaments - the posterior cruciate ligament attaches to the medial surface of the lateral condyle, and the anterior cruciate ligament to a posterosuperior facet on the lateral surface of the medial condyle.
- Patellar surface: anteriorly, the condyles are joined and form a V-shaped trench facing anteriorly where the patella glides. The lateral surface of the trench is larger and steeper than the medial - a feature relevant to patellar tracking and dislocation.
- Epicondyles: bony elevations on the nonarticular outer surfaces of each condyle for the attachment of the collateral ligaments of the knee.
- Adductor tubercle: a prominent tubercle on the superiomedial aspect of the medial condyle, where the medial supracondylar line terminates and where the adductor magnus has its distal attachment.
- Medial epicondyle: a rounded eminence on the medial surface of the medial condyle, with the adductor tubercle just posterosuperior to it.
- The floor of the popliteal fossa is formed by the posterior surface of the distal femur, bounded by the medial and lateral supracondylar lines.
- Just lateral to the lower end of the medial supracondylar line is a roughened area for the proximal attachment of the medial head of gastrocnemius.
- On the lateral side, two facets posterior to the lateral epicondyle attach the lateral head of gastrocnemius (upper facet) and the popliteus (inferior facet), with the popliteus tendon running in the groove between them.
4. Blood Supply to the Femoral Head - Clinical Anatomy
The blood supply to the head and neck of the femur comes from three sources:
- Retinacular vessels - branches of the medial and lateral circumflex femoral arteries form an arterial ring at the base of the neck, from which vessels course along the neck, penetrate the fibrous capsule, and ascend in the retinacula to reach the femoral head. This is the most important supply.
- Medullary vessels (from the femoral shaft) - become attenuated with age as red marrow is replaced by fatty marrow.
- Artery of the ligamentum teres (a branch of the obturator artery) - small, variable, and tends to become further attenuated with atherosclerosis in the elderly.
In older adults, the first source (retinacular vessels) often becomes the sole blood supply to the femoral head, making femoral neck fractures particularly dangerous.
5. Clinical Correlates (Gray's Anatomy "In the Clinic")
Femoral Neck Fractures
Gray's classifies femoral neck fractures by location:
- Subcapital - fracture line at the head-neck junction; highest risk of avascular necrosis because the retinacular vessels are most vulnerable.
- Transcervical - fracture through the mid-neck.
- Basicervical - fracture at the base of the neck; lowest risk of avascular necrosis.
In the elderly (especially postmenopausal women with osteoporosis), these typically result from low-energy trauma (e.g., a fall from standing height) and produce transverse subcapital fractures. In the young, they result from high-energy trauma (fall from height, motor vehicle accidents with axial loading on an abducted knee) and tend to be more vertical and distal (basicervical).
Clinically, a displaced femoral neck fracture presents with the affected leg shortened and externally rotated - caused by the unopposed pull of iliopsoas (acting on the lesser trochanter) pulling the femur proximally and into external rotation, with adductor spasm exacerbating the rotation.
Treatment may involve hemiarthroplasty (replacing the femoral head with a metal prosthesis while preserving the native acetabulum) when the blood supply to the head has been disrupted.
Intertrochanteric Fractures
The break runs from the greater to the lesser trochanter, not involving the femoral neck. Because the retinacular vessels are spared, avascular necrosis of the femoral head does not occur. These are most common in the elderly after low-energy impact and are managed with internal fixation rather than arthroplasty.
An isolated lesser trochanter fracture in an adult is considered pathological until proven otherwise - it most commonly signals an underlying malignant deposit eroding the bone.
Femoral Shaft Fractures
An appreciable amount of energy is required to fracture the femoral shaft. These injuries are therefore associated with significant soft tissue damage to surrounding muscle compartments and their neurovascular contents.
Source: Gray's Anatomy for Students, Chapter 6 - Lower Limb, pp. 657-660, 687-688, 784. The femur is described in sections on the Proximal Femur, Shaft of the Femur, Shaft and Distal End of Femur, and clinical cases including Fracture of Neck of Femur.
This is a shared conversation. Sign in to Orris to start your own chat.