Temperature regulation in physiology uc exam 1 st year answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have enough comprehensive content now. Let me compile the full exam answer.
Temperature Regulation in Physiology - 1st Year UC Exam Answer
1. Introduction - Homeothermy
Humans are homeothermic (warm-blooded) animals who maintain a relatively constant internal body temperature despite wide fluctuations in environmental temperature. This stability is essential because enzyme systems of the body have narrow temperature ranges for optimal function. The regulation is primarily integrated in the hypothalamus.
- Guyton & Hall, Medical Physiology
2. Normal Body Temperature
| Site | Normal Value |
|---|---|
| Oral (standard) | 37°C (98.6°F) |
| Rectal (core) | ~37.5°C (0.5°C above oral) |
| Axillary | ~36.5°C (0.5°C below oral) |
| Skin | Varies with environment |
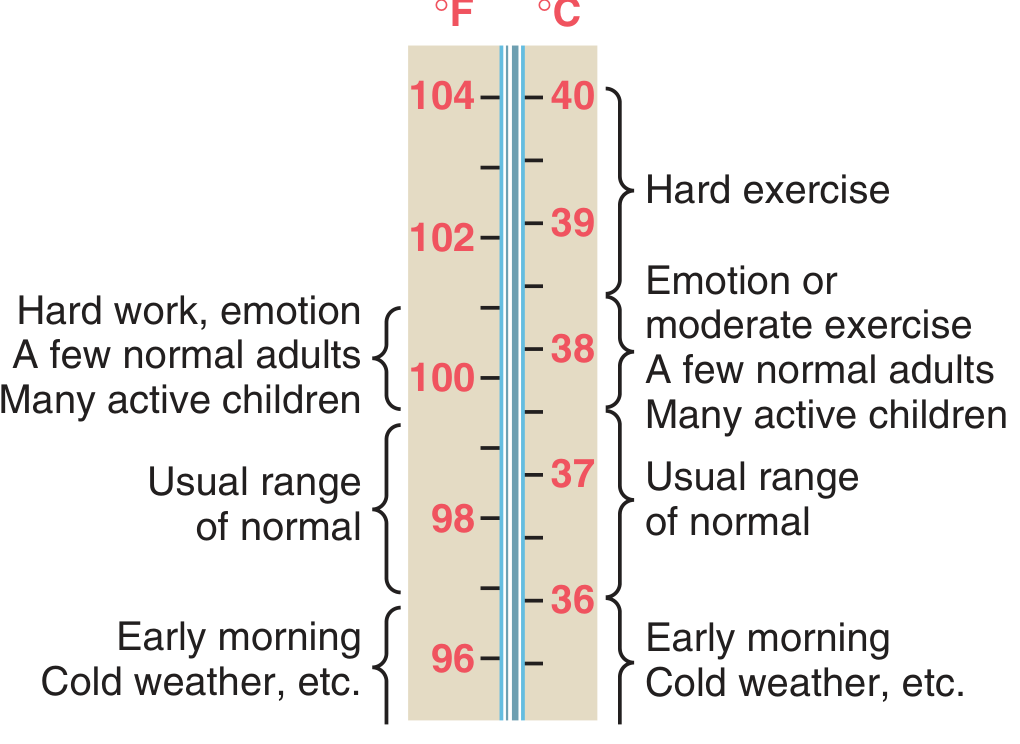
Core temperature is the temperature of deep tissues (thorax, abdomen, brain). It remains constant within ±0.6°C. Skin temperature fluctuates with environment and is what matters for heat loss to surroundings.
Circadian variation: Core temperature is lowest around 6 AM and highest in the evenings, showing a daily fluctuation of 0.5-0.7°C.
In women: An additional monthly cycle exists - basal temperature rises ~0.5°C at the time of ovulation (useful for detecting ovulation).
- Ganong's Review of Medical Physiology, 26th Ed.
3. Heat Balance: Production vs. Loss
Body temperature = Balance between heat production and heat loss.
If Heat Production > Heat Loss → Body temperature rises
If Heat Loss > Heat Production → Body temperature falls
4. Heat Production
Sources of heat in the body:
- Basal metabolic rate (BMR) - all cells continuously produce heat
- Muscular activity - exercise is the greatest source; shivering is the most potent cold-response mechanism
- Thyroid hormones (thyroxine T3/T4) - stimulate Na⁺-K⁺ ATPase, increase O₂ consumption, increase metabolic rate → thermogenic
- Sympathetic nervous system / catecholamines (epinephrine, norepinephrine) - stimulate β receptors in brown adipose tissue → non-shivering thermogenesis
- Specific dynamic action (SDA) of food / thermogenic effect - digestion, absorption and storage of food produces heat
- Chemical reactions - cell temperature increase accelerates reactions (Q₁₀ effect)
- Guyton & Hall, Medical Physiology
5. Heat Loss Mechanisms
Heat is lost from the body surface by four physical methods:
A. Radiation (~60% at rest, room temperature)
- Transfer of heat as infrared electromagnetic waves from body to surroundings (and vice versa)
- Does not require a medium
- Most important mechanism at normal room temperature
- Depends on temperature gradient between body surface and surroundings
B. Conduction (~15%)
- Direct transfer of heat by physical contact with cooler objects
- Water conducts heat ~20 times better than air (explains rapid heat loss in cold water)
- Convection is a special form: air/water currents carry away conducted heat
C. Evaporation (~25%)
Two types:
- Insensible perspiration (~600 ml/day, 12-16 kcal/hour): continuous water evaporation from skin and respiratory tract, cannot be controlled
- Sensible (active) sweating: controlled by the hypothalamus via sympathetic cholinergic fibers to sweat glands; major heat loss mechanism during exercise or high environmental temperature
- Each gram of water evaporated removes ~0.58 kcal (580 cal) of heat
When environmental temperature > skin temperature, evaporation becomes the ONLY effective heat loss mechanism.
D. Radiation from Expired Air (minor)
- Warming of inspired air + humidification accounts for ~10% of heat loss at rest
Summary table:
| Method | % at Rest | Key Feature |
|---|---|---|
| Radiation | ~60% | Infrared waves, no contact needed |
| Conduction + Convection | ~15% | Direct contact; wind enhances |
| Evaporation | ~25% | Only method when temp ≥ skin temp |
- Guyton & Hall, Medical Physiology; Costanzo Physiology, 7th Ed.
6. Role of the Hypothalamus (The Thermostat)
The hypothalamus is the central integrator of temperature regulation.
Anterior Hypothalamus (Pre-optic area) - "Heat Loss Center"
- Contains heat-sensitive neurons that respond to rising blood temperature
- Coordinates heat dissipation: vasodilation of skin vessels, sweating
- Lesion → inability to lose heat → hyperthermia
Posterior Hypothalamus - "Heat Conservation/Production Center"
- Activated by cold
- Coordinates heat conservation: vasoconstriction, shivering, sympathetic activation
- Lesion → inability to generate/conserve heat → hypothermia
Set-point concept:
- The hypothalamus acts like a thermostat set at ~37°C
- Temperature sensors (peripheral in skin + central in hypothalamus) feed information to hypothalamus
- If actual temperature deviates from set point, corrective responses activate
7. Responses to Cold (Mechanisms for Generating/Conserving Heat)
| Mechanism | Mediator | Effect |
|---|---|---|
| Cutaneous vasoconstriction | Sympathetic α₁ activation | Reduces skin blood flow → reduces heat loss |
| Shivering | Posterior hypothalamus → α & γ motor neurons | Rhythmic skeletal muscle contraction → most potent heat producer |
| Non-shivering thermogenesis | Sympathetic β activation in brown fat | Uncoupled oxidative phosphorylation → heat without work |
| Thyroid hormone release | TRH → TSH → T3/T4 | Increased Na⁺-K⁺ ATPase, O₂ consumption, metabolic rate |
| Behavioral responses | Conscious cortex | Curling up, adding clothing, seeking warmth |
| Piloerection (goosebumps) | Sympathetic → arrector pili | Traps air layer - minor in humans |
- Costanzo Physiology, 7th Ed.
8. Responses to Heat (Mechanisms for Dissipating Heat)
| Mechanism | Mediator | Effect |
|---|---|---|
| Cutaneous vasodilation | Decreased sympathetic tone | Up to 30% of cardiac output to skin; conducts heat to surface |
| Sweating | Sympathetic cholinergic fibers | Evaporation cools skin; up to 2-3 L/hour when acclimatized |
| Behavioral responses | Cortex | Seeking shade, removing clothing, drinking cold water |
| Decreased muscle tone | CNS inhibition | Reduces heat production |
Sweat glands:
-
Secretion controlled by sympathetic cholinergic fibers (exception to usual adrenergic sympathetic rule)
-
Blocked by atropine (anticholinergic) → dangerous hyperthermia
-
Guyton & Hall, Medical Physiology
9. Heat Acclimatization
With repeated heat exposure over 1-6 weeks:
- Sweat production increases: up to 2-3 L/hour (vs. 1 L/hour unacclimatized)
- Sweat sodium concentration decreases (aldosterone-mediated salt conservation)
- Earlier onset of sweating
- Salt loss decreases from 15-30 g/day to 3-5 g/day
- Acclimatization disappears within weeks if not maintained
10. Fever
Definition: Body temperature above the normal range due to upward resetting of the hypothalamic set point.
Pathophysiology:
- Infection/injury → macrophages/leukocytes phagocytize pathogens
- Release of cytokines (especially IL-1/Interleukin-1, also IL-6, TNF-α) - "endogenous pyrogens"
- IL-1 acts on OVLT (organum vasculosum of the lamina terminalis) of hypothalamus
- Triggers prostaglandin E₂ (PGE₂) synthesis via cyclooxygenase (COX)
- PGE₂ raises the hypothalamic set point
- Body now perceives normal temperature as "too cold" → activates heat conservation mechanisms (shivering, vasoconstriction) = chills/rigor (fever rising phase)
- When infection resolves → set point drops → body sweats profusely to lose heat = defervescence
Exogenous pyrogens: LPS (lipopolysaccharide) from gram-negative bacteria, bacterial toxins
Antipyretics (e.g., aspirin, paracetamol): Inhibit COX → block PGE₂ synthesis → lower set point → sweating → fever reduction
Beneficial effects of fever:
- Impairs bacterial/viral replication
- Enhances immune cell activity
- Increases antibody production
11. Abnormalities of Temperature Regulation
Hyperthermia (Heat Illnesses)
| Condition | Description |
|---|---|
| Heat cramps | Painful muscle spasms; NaCl depletion from heavy sweating |
| Heat exhaustion | Volume depletion + electrolyte loss; weakness, dizziness, tachycardia; temp < 40°C |
| Heat stroke | Core temp > 40°C + CNS dysfunction (confusion, loss of consciousness); failure of thermoregulation; medical emergency |
| Malignant hyperthermia | Genetic defect in RYR1/CACNA1A; triggered by volatile anesthetics; uncontrolled Ca²⁺ release from SR → massive muscle contraction → extreme heat; treat with dantrolene |
| Neuroleptic malignant syndrome | Dopamine D2 blockade (antipsychotics); hyperthermia + rigidity + autonomic instability |
Hypothermia
- Core temp < 35°C
- At ~28°C: loss of ability to auto-rewarm; loss of consciousness
- Metabolic/physiologic processes slow down
- Humans can tolerate 21-24°C with careful management
- Useful clinically (cardiac surgery, brain protection)
12. Peripheral Temperature Receptors
- Warm receptors: Free nerve endings; respond to 30-43°C; C-fibers
- Cold receptors: Free nerve endings; respond to 10-40°C (peak 25°C); Aδ fibers (fast); C-fibers (slow)
- Paradoxical cold sensation: Extreme heat (>45°C) can stimulate cold receptors → "burning cold"
- Signals travel via spinothalamic tract → thalamus → somatosensory cortex
13. Key Points Summary (Exam Mnemonics)
Heat loss = RCES (Radiation, Conduction/Convection, Evaporation, Sweating)
Hypothalamus roles:
- Anterior = Loss of heat (A for Anterior = cAring about cooling)
- Posterior = Production/conservation of heat
Fever sequence: Pathogen → Macrophage → IL-1 → Hypothalamus → PGE₂ → ↑Set point → Shiver → Fever → Sweat → Defervescence
Sweat glands = Sympathetic but CHOLINERGIC (remember this exception!)
Sources: Guyton & Hall Textbook of Medical Physiology; Costanzo Physiology, 7th Ed.; Ganong's Review of Medical Physiology, 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.