Do Research on The Topic ' Variations in The Shape of The Stomach '
Reading File
search_medical_text
variations in shape of the stomach anatomical types
search_medical_image
stomach shape variations anatomy types
GradeResponse
GradeResponse
search_medical_text
gastric shape J-shaped steer-horn orthotonic hypertonic hypotonic stomach radiology
search_medical_text
stomach position body habitus sthenic asthenic radiographic appearance
GradeResponse
Based on the retrieved content and comprehensive anatomical knowledge, here is a thorough research summary on variations in the shape of the stomach.
Variations in the Shape of the Stomach
Overview
The stomach is the most dilated part of the gastrointestinal tract, situated between the esophagus and the duodenum. Its shape is remarkably variable — influenced by body type (habitus), posture, degree of filling, muscle tone, age, and pathological conditions. No two stomachs look identical in life.
Anatomical Regions (Constant Landmarks)
Before discussing variations, the consistent anatomical divisions serve as reference points:
| Region | Description |
|---|---|
| Cardia | Junction with the esophagus |
| Fundus | Dome-shaped superior portion (left of cardia) |
| Body (Corpus) | Largest central part |
| Pyloric antrum | Funnel-shaped distal region |
| Pylorus | Junction with duodenum |
| Incisura angularis | Angular notch on lesser curvature |
| Greater curvature | Longer left lateral border |
| Lesser curvature | Shorter right medial border |
Morphological (Shape) Variations
The stomach assumes four classically described shapes, largely correlating with body habitus:
1. J-Shaped Stomach (Orthotonic / Most Common)
- Seen in individuals of average build
- The stomach hangs vertically downward and curves to the right like the letter "J"
- The pylorus lies near the midline at approximately the level of L1–L2
- The incisura angularis is well-defined
- The greater curvature may reach the level of the iliac crest
- This is considered the standard anatomical form
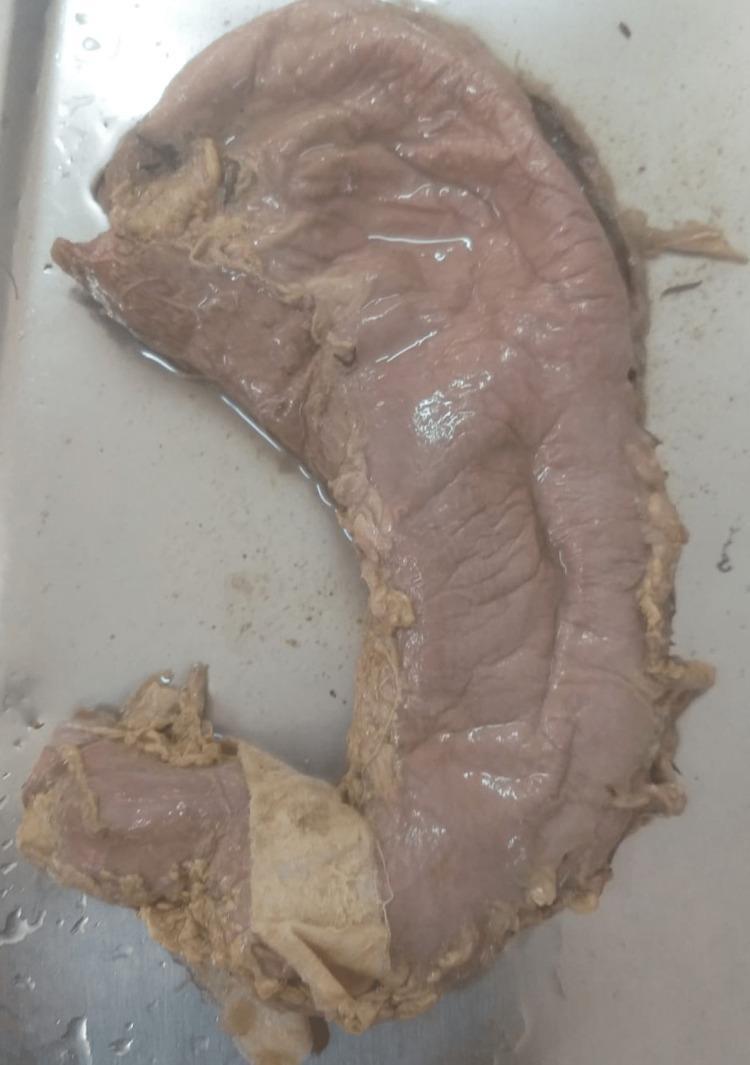
Cadaveric specimen showing a J-shaped stomach (Type III morphological variation), with pronounced vertical elongation, a sharp incisura angularis, and the classic J configuration:
2. Steer-Horn Stomach (Hypertonic)
- Seen in hypersthenic (broad, muscular) individuals
- High transverse position, almost horizontal
- The pylorus lies high and to the right
- Short, wide, and almost transverse in orientation
- The fundus and pylorus are at nearly the same level
- The stomach resembles the horns of a steer
- Associated with a high pylorus and can be mistaken for pathology on imaging
3. Cascade Stomach
- A specific variation where the fundus folds posteriorly over the body
- Barium or contrast "cascades" from the fundus downward into the body
- Can be normal or associated with a large hiatus hernia or aerophagia
- More common in the elderly and in individuals lying supine
- Has clinical significance as it may trap air/fluid and cause bloating
4. Fish-Hook Stomach (Hypotonic / Elongated)
- Seen in asthenic (thin, tall) individuals
- Greatly elongated, hanging low into the pelvis
- The pylorus may be located as low as the true pelvis
- Associated with gastroptosis (downward displacement)
- Greater curvature may drop to the level of the pelvic brim or below
- Greater risk of gastric volvulus
5. Leather-Bottle Stomach (Linitis Plastica)
- Pathological variation — not a normal anatomical type
- The stomach is shrunken, rigid, and non-distensible
- Caused by diffuse infiltrating adenocarcinoma involving all gastric layers
- Loss of normal peristalsis and rugal folds
- Clinically important differential when a small, non-distending stomach is seen on imaging or endoscopy
Classification by Muscle Tone
| Type | Tone | Shape | Habitus | Position |
|---|---|---|---|---|
| Orthotonic | Normal | J-shaped | Average | Intermediate |
| Hypertonic | High | Steer-horn | Hypersthenic | High/transverse |
| Hypotonic | Low | Fish-hook/elongated | Asthenic | Low/pelvic |
| Atonic | Absent | Greatly elongated, bag-like | Cachectic/elderly | Very low |
Factors Influencing Gastric Shape
1. Body Habitus
- The single most important determinant in radiological practice
- Hypersthenic → high, horizontal stomach
- Asthenic → low, elongated stomach
2. Posture
- Erect: stomach elongates and descends
- Supine: stomach becomes more horizontal and transverse
- Left lateral decubitus: fundal air moves to the body
3. Degree of Filling
- Empty stomach: comma-shaped or tubular, with prominent rugal folds
- Full stomach: fully expanded, globular or J-shaped, rugae flattened
4. Age and Sex
- Infants: stomach is more horizontal and the cardia is more medial
- Neonates: the stomach is spherical/round with a prominent fundus
- Elderly females: more prone to gastroptosis and fish-hook shape
5. Respiratory Phase
- Deep inspiration → stomach descends by 3–5 cm
- Relevant for interpretation of barium studies and ultrasound
6. Pregnancy
- Growing uterus displaces the stomach superiorly and to the left
- Can alter acid reflux mechanics and gastric emptying
Developmental (Congenital) Variations
| Condition | Description |
|---|---|
| Congenital hypertrophic pyloric stenosis | Hypertrophied pyloric muscle → "olive" mass, string sign on barium, "shoulder sign" on ultrasound |
| Microgastria | Rare; stomach fails to develop normally; tubular, midline, non-rotating |
| Gastric duplication cysts | Cystic structures within the gastric wall; spherical or tubular |
| Heterotopic pancreas | Ectopic pancreatic tissue in gastric wall, usually antrum |
Radiological Assessment
As noted by Bailey & Love's Short Practice of Surgery (28th Ed., p. 1174), upper GI radiology has largely been replaced by CT (with oral contrast) and endoscopy for evaluating gastric anatomy. However, barium meal studies remain useful conceptually for understanding shape variations:
- Barium meal (double-contrast): best delineates rugal pattern, shape, and peristalsis
- CT scan: gold standard for assessing wall thickness, position, and pathological change
- Ultrasound: useful in neonates (pyloric stenosis), limited in adults
- MRI: increasingly used for gastric motility studies
Clinical Significance of Shape Variations
| Variation | Clinical Relevance |
|---|---|
| J-shaped (orthotonic) | Normal; baseline reference |
| Steer-horn (hypertonic) | May mimic high gastric outlet obstruction on imaging |
| Fish-hook / gastroptosis | Risk of gastric volvulus; associated with chronic dyspepsia |
| Cascade stomach | Can trap gas and fluid; associated with hiatus hernia |
| Linitis plastica | Malignant; urgent workup required |
| Congenital microgastria | Requires surgical reconstruction in neonates |
Summary
The shape of the stomach is one of the most variable structures in human anatomy. The four principal radiological types — steer-horn, orthotonic (J-shaped), fish-hook, and atonic — reflect a spectrum of muscle tone and body build. Understanding these normal variations is critical for radiologists, surgeons, and gastroenterologists to avoid misinterpreting normal anatomy as pathology, and vice versa. Pathological alterations (linitis plastica, pyloric stenosis, volvulus) superimposed on these baseline variants add additional layers of clinical complexity.
This is a shared conversation. Sign in to Orris to start your own chat.