Teach me topic of bladder cancer from symptoms till management in easy and understandable and memorizable way from cambell book of urology
Reading File
search_medical_text
bladder cancer symptoms diagnosis hematuria presentation
search_medical_text
bladder cancer staging TNM classification non-muscle invasive muscle invasive
search_medical_image
bladder cancer cystoscopy TNM staging diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
bladder cancer risk factors epidemiology transitional cell carcinoma urothelial
search_medical_text
bladder cancer management treatment TURBT intravesical BCG chemotherapy cystectomy
Here is a complete, Campbell's-aligned guide to Bladder Cancer — from symptoms to management — structured for easy understanding and memorization.
🫧 BLADDER CANCER — Complete Guide
Based on Campbell's Urology & Harrison's Principles of Internal Medicine
🧠 MEMORY FRAMEWORK: "STEP-UP"
Symptoms → Types → Etiology/Risk Factors → Pathology & Staging → Urology Workup (Diagnosis) → Plan (Management)
1️⃣ SYMPTOMS — "Blood in urine = Bladder Cancer until proven otherwise"
🔴 Cardinal Symptom: Painless Gross Hematuria
- Present in ~85% of cases
- PAINLESS = key distinguishing feature (painful hematuria = stones/infection)
- Intermittent in nature — patient may ignore it!
- Can be microscopic (found incidentally on urinalysis)
🟡 Other Symptoms (LUTS — Lower Urinary Tract Symptoms):
| Symptom | Clue |
|---|---|
| Frequency & Urgency | Irritative symptoms mimicking UTI |
| Dysuria | Especially in carcinoma in situ (CIS) |
| Nocturia | Bladder irritation |
| Pelvic pain | Advanced/invasive disease |
| Flank pain | Ureteral obstruction by tumor |
| Weight loss, bone pain | Metastatic disease |
💡 Memory Tip: Any adult >40 with "UTI that doesn't resolve" or "recurrent UTI in a man" → think bladder cancer!
2️⃣ TYPES — "Who causes most trouble?"
🏆 Urothelial (Transitional Cell) Carcinoma — 90–95%
- Arises from the urothelium (transitional epithelium lining bladder)
- Most common in developed countries
Other Types (less common):
| Type | Association |
|---|---|
| Squamous Cell Carcinoma | Chronic irritation, schistosomiasis (S. haematobium), stones |
| Adenocarcinoma | Urachal remnant, bladder exstrophy |
| Small Cell Carcinoma | Aggressive, rare, neuroendocrine origin |
3️⃣ ETIOLOGY / RISK FACTORS — "SMOKING SCAB"
| Letter | Risk Factor |
|---|---|
| S | Smoking — #1 risk factor (2–4× increased risk; 50% of all cases) |
| C | Chemical exposure (arylamines, benzidine — dye/rubber/leather workers) |
| A | Age >60 (peak incidence) |
| B | Bladder infections — chronic (Schistosoma haematobium → squamous type) |
| + | Male sex (3:1 male:female) |
| + | Aristolochic acid (herbal medicines) |
| + | Radiation (pelvic RT history) |
| + | Cyclophosphamide (chemotherapy — causes hemorrhagic cystitis → cancer) |
| + | White race more commonly affected |
4️⃣ PATHOLOGY & STAGING — "How deep does it go?"
This is the most important concept — it determines everything about treatment.
Bladder Wall Layers (inside → outside):
Urothelium → Lamina Propria → Muscularis Propria → Perivesical Fat → Adjacent Organs
TNM Staging:
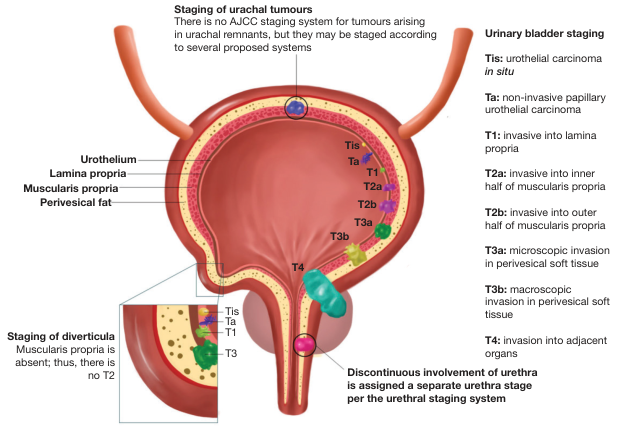
| Stage | Depth of Invasion | Category |
|---|---|---|
| Tis | Carcinoma in situ — flat, high-grade, confined to urothelium | NMIBC |
| Ta | Non-invasive papillary — confined to urothelium | NMIBC |
| T1 | Invades lamina propria (NOT muscle) | NMIBC |
| T2a | Invades inner ½ of muscularis propria | MIBC |
| T2b | Invades outer ½ of muscularis propria | MIBC |
| T3a | Microscopic perivesical fat invasion | MIBC |
| T3b | Macroscopic perivesical fat invasion | MIBC |
| T4 | Adjacent organs (prostate, vagina, rectum, pelvic wall) | MIBC |
💡 The Big Split:
- NMIBC (Non-Muscle Invasive) = Ta, T1, Tis → ~75% of cases → Treated conservatively
- MIBC (Muscle Invasive) = T2–T4 → ~18% of cases → Treated aggressively
- Metastatic = only ~3% at presentation (Harrison's, p. 2614)
Lymph Node (N) Staging:
- N0 = no nodes
- N1 = single pelvic node
- N2 = multiple pelvic nodes
- N3 = common iliac nodes
Grade (also critical!):
| Grade | Behavior |
|---|---|
| Low Grade | Slow growing, recurs but rarely invades |
| High Grade | Aggressive, invasive potential — CIS is ALWAYS high grade |
5️⃣ DIAGNOSIS / WORKUP — "See it, Sample it, Stage it"
Step 1: SEE IT — Cystoscopy
- Gold standard for diagnosis
- Directly visualizes the tumor; guides biopsy
- Describes: size, number, location, appearance (papillary vs. sessile/flat)
Step 2: TEST THE URINE
| Test | Use |
|---|---|
| Urinalysis | Detects hematuria (micro or gross) |
| Urine Cytology | Detects shed malignant cells — HIGH specificity for high-grade/CIS; low sensitivity for low-grade |
| Urine FISH/NMP22 | Newer urine tumor markers — adjunct to cytology |
Step 3: SAMPLE IT — TURBT (Transurethral Resection of Bladder Tumor)
- Diagnostic AND therapeutic procedure
- Resects visible tumor, sends for histopathology
- Must include muscularis propria in the specimen to assess depth of invasion
- Re-TURBT at 4–6 weeks for high-grade T1 or incomplete initial resection
Step 4: STAGE IT — Imaging
| Imaging | Purpose |
|---|---|
| CT Urography (CTU) | Upper tract evaluation (ureter, kidney — same urothelium!) |
| CT Chest/Abdomen/Pelvis | Lymph nodes, distant mets — for MIBC |
| MRI Pelvis (mpMRI) | Better soft tissue detail, staging of local invasion |
| Bone Scan | If bone pain or elevated ALP |
| PET-CT | Metastatic workup in select cases |
6️⃣ MANAGEMENT — "Match the treatment to the stage"
🟢 A. NON-MUSCLE INVASIVE BLADDER CANCER (NMIBC) — Ta, T1, Tis
Step 1: TURBT (always first)
Step 2: Risk-Stratify
| Risk | Features | Treatment |
|---|---|---|
| Low Risk | Low-grade, solitary Ta, <3 cm, first occurrence | Single dose intravesical chemotherapy post-TURBT (e.g., Mitomycin C) |
| Intermediate Risk | Multifocal, recurrent, or larger low-grade | Intravesical BCG × 6 weeks (induction) OR Mitomycin C |
| High Risk | T1 high-grade, CIS, or multifocal high-grade | Intravesical BCG (induction + maintenance × 1–3 years) |
🧫 Intravesical BCG (Bacillus Calmette-Guérin):
- Immunotherapy — stimulates local immune response against tumor cells
- Best treatment for CIS and high-grade NMIBC
- Protocol: 6-week induction + 3-week maintenance courses
- Side effects: cystitis symptoms, BCG sepsis (rare but life-threatening)
⚠️ BCG Failure → Radical Cystectomy (or intravesical Valrubicin/Pembrolizumab in BCG-unresponsive cases)
Step 3: Surveillance
- Cystoscopy + cytology every 3 months × 2 years, then every 6 months × 2 years, then annually
- Upper tract imaging annually
🔴 B. MUSCLE-INVASIVE BLADDER CANCER (MIBC) — T2–T4, N0–N2, M0
🏆 Gold Standard: Radical Cystectomy + Neoadjuvant Chemotherapy
Neoadjuvant Cisplatin-based Chemotherapy (MVAC or GC regimen):
- Given BEFORE surgery
- Improves overall survival by ~5–8%
- Targets micrometastatic disease
- Must have adequate renal function (GFR >50–60)
Radical Cystectomy:
- Males: Remove bladder, prostate, seminal vesicles, proximal urethra, pelvic lymph nodes
- Females: Remove bladder, uterus, ovaries, anterior vaginal wall, urethra, pelvic lymph nodes
Urinary Diversion after Cystectomy — "Where does urine go now?"
| Type | Description | Memory |
|---|---|---|
| Ileal Conduit | Ureters → loop of ileum → skin stoma (urostomy bag) | Simplest, most common |
| Orthotopic Neobladder | Ileum fashioned into pouch, connected to urethra | Patient voids normally! |
| Continent Cutaneous Reservoir | Internal pouch, catheterized via stoma | No external bag |
🔵 Bladder-Sparing Trimodality Therapy (TMT):
For patients who refuse or cannot tolerate cystectomy:
- Maximal TURBT (debulk as much as possible)
- Concurrent chemoradiation (Cisplatin + RT)
- Outcomes comparable to cystectomy in selected patients
🟣 C. METASTATIC BLADDER CANCER
| Treatment | Details |
|---|---|
| 1st Line: Cisplatin-based chemo | GC (Gemcitabine + Cisplatin) or MVAC |
| If cisplatin-ineligible: | Carboplatin + Gemcitabine, or Atezolizumab/Pembrolizumab (checkpoint inhibitors) |
| 2nd Line: | Pembrolizumab (anti-PD-1), Erdafitinib (FGFR3 inhibitor if FGFR mutation), Enfortumab vedotin (ADC) |
| Maintenance: | Avelumab (checkpoint inhibitor) after platinum-based chemo |
7️⃣ PROGNOSIS — "Stage is everything"
| Stage | 5-Year Survival |
|---|---|
| NMIBC (Ta, T1) | ~80–90% |
| MIBC (T2) | ~50–60% |
| MIBC (T3–T4) | ~30–40% |
| Metastatic (M1) | <15% |
⚠️ NMIBC has a high recurrence rate (~70%) but low mortality if properly surveilled. CIS has the highest risk of progression to invasive disease.
🗂️ MASTER SUMMARY TABLE
| Feature | NMIBC | MIBC | Metastatic |
|---|---|---|---|
| Stages | Ta, T1, Tis | T2, T3, T4 | Any T, M1 |
| % at presentation | 75% | 18% | 3% |
| 1st treatment | TURBT | Neoadj chemo + Cystectomy | Platinum chemo |
| Adjuvant | Intravesical BCG/Chemo | RT ± chemo | Immunotherapy |
| Surveillance | Cystoscopy q3mo | CT imaging | Response assessment |
| 5-yr survival | 80–90% | 30–60% | <15% |
🔑 HIGH-YIELD EXAM PEARLS
- Painless gross hematuria = bladder cancer until proven otherwise
- Smoking is the #1 risk factor (50% of cases)
- TURBT = both diagnosis AND treatment for NMIBC
- CIS = flat, high-grade, aggressive — always needs BCG
- Muscularis propria in TURBT specimen is essential — without it, staging is incomplete
- BCG failure in NMIBC = radical cystectomy (don't delay)
- Neoadjuvant cisplatin before cystectomy improves survival
- Schistosoma haematobium → squamous cell carcinoma (not transitional!)
- Upper tract surveillance mandatory — same urothelium, same risk
- Ileal conduit = simplest diversion; Neobladder = best quality of life
This covers the complete bladder cancer journey from first symptom to definitive management, organized to be both clinically logical and easy to recall during exams. Let me know if you'd like any section expanded — grading systems, surgical technique details, or specific chemotherapy regimens!
This is a shared conversation. Sign in to Orris to start your own chat.