explain meningitis in detail way its pathophysiology mechanism its types its symptoms initial and sympoms criteria dianostic approach physical test to diagnose it clinically and its treatment approach and give clinical exmple to explain it
Reading File
Finding Sources
Finding Sources
Searching PubMed
"meningitis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete, detailed answer.
Meningitis: A Comprehensive Clinical Guide
1. Definition
Meningitis is an inflammatory process involving the leptomeninges (pia mater and arachnoid mater) within the subarachnoid space (SAS). When inflammation extends into the brain parenchyma, the condition is called meningoencephalitis. The term applies to both infectious causes (bacterial, viral, fungal, parasitic) and non-infectious ones (chemical meningitis from ruptured epidermoid cysts, carcinomatous meningitis from cancer cells seeding the SAS).
- Harrison's Principles of Internal Medicine 22E, p. 1162
- Robbins & Kumar Basic Pathology, p. 833
2. The Anatomy of the Problem
To understand meningitis, you must first understand the space it occupies. CSF is produced in the choroid plexus, flows through the ventricles and subarachnoid space, and is reabsorbed at the arachnoid villi. Pathogens that breach the blood-brain barrier and reach this enclosed fluid-filled compartment have effectively bypassed the body's primary immune defenses.
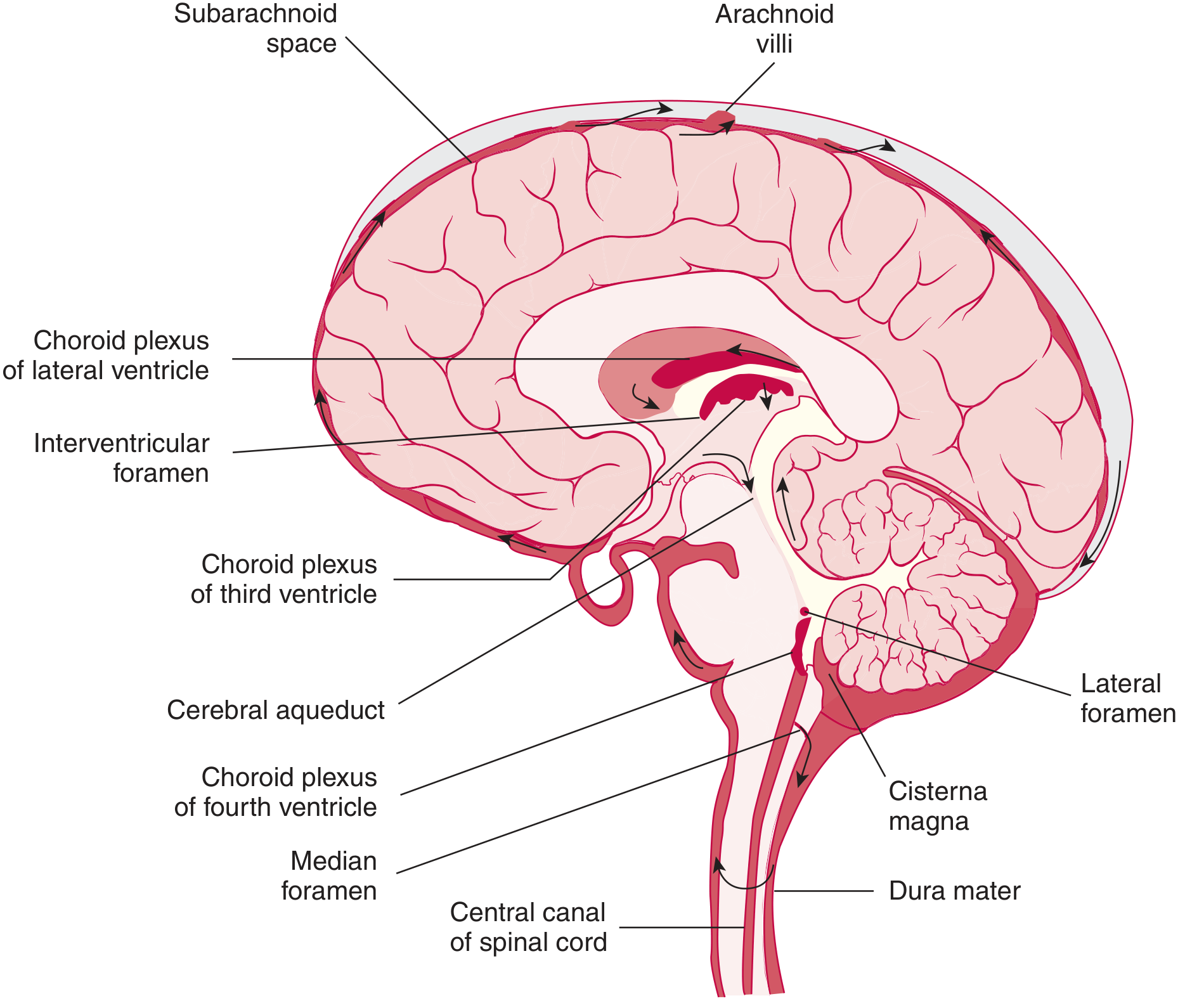
CSF flow diagram showing the subarachnoid space where meningitis occurs (Tietz Textbook of Laboratory Medicine, 7th Ed.)
3. Types of Meningitis
A. Acute Pyogenic (Bacterial) Meningitis
The most life-threatening form. Pathogens vary by age:
| Age Group | Common Organisms |
|---|---|
| Neonates (<1 month) | E. coli, Group B Streptococcus (GBS) |
| Infants/Children | Neisseria meningitidis, S. pneumoniae |
| Young adults (15-24) | Neisseria meningitidis |
| Adults >20 years | S. pneumoniae (~50%), N. meningitidis (~25%) |
| Elderly / Immunocompromised | S. pneumoniae, Listeria monocytogenes |
| Post-neurosurgery / CSF shunt | Coagulase-negative staph, S. aureus, gram-negatives |
Predisposing conditions for pneumococcal meningitis include pneumonia, sinusitis, otitis media, alcoholism, diabetes, splenectomy, hypogammaglobulinemia, complement deficiency, and head trauma with basilar skull fracture (CSF rhinorrhea). Harrison's, p. 1162
B. Aseptic (Viral) Meningitis
The most common form overall. Enteroviruses (especially Enterovirus B species) cause ~50% of all meningitis/encephalitis cases in the United States. Other causes include arboviruses (West Nile virus), herpesviruses (HSV-2), HIV seroconversion, and mumps. Symptoms are milder and usually self-limited in immunocompetent patients.
- Goldman-Cecil Medicine, Ch. 381
C. Chronic Meningitis
Onset gradual over weeks to months. Causes:
- Tuberculous - most common chronic form worldwide; subacute/chronic presentation with fever, weight loss, night sweats; may be the only manifestation of TB
- Fungal - Cryptococcus neoformans (especially in HIV), Histoplasma, Coccidioides
- Spirochetal - Treponema pallidum (neurosyphilis), Borrelia burgdorferi (Lyme)
- Rosen's Emergency Medicine, p. 4176; Tietz Textbook, p. 3157
D. Non-infectious Meningitis
- Carcinomatous meningitis (metastatic cancer in SAS)
- Chemical meningitis (ruptured dermoid/epidermoid cyst)
- Drug-induced (NSAIDs, TMP-SMX, IVIG)
- Autoimmune (SLE, sarcoidosis)
4. Pathophysiology Mechanism
The pathophysiology of bacterial meningitis - the most dangerous type - proceeds in a cascade:
Step 1: Pathogen Entry into the Subarachnoid Space
Pathogens reach the SAS by two main routes:
- Hematogenous spread (most common): bacteremia seeds the choroid plexus or meningeal vessels, crossing the blood-brain barrier (BBB)
- Direct extension: from contiguous structures - sinusitis, otitis media, mastoiditis, or a basilar skull fracture with CSF leak
N. meningitidis, for example, begins with nasopharyngeal colonization. Invasive disease follows when bacterial virulence factors overwhelm the host's ability to produce anti-meningococcal antibodies and activate complement. Individuals with complement component deficiencies (including properdin) are highly susceptible. Harrison's, p. 1162
Step 2: Bacterial Replication in a "Privileged" Space
The SAS is an immunologically privileged site with low complement levels, low immunoglobulin concentrations, and poor phagocytic activity. Bacteria replicate rapidly with little initial resistance.
Step 3: Innate Immune Recognition and Cytokine Storm
Bacterial cell-wall components (lipopolysaccharide in gram-negatives, teichoic acid/peptidoglycan in gram-positives) are recognized by pattern-recognition receptors on microglia, astrocytes, and meningeal macrophages.
This triggers massive production of:
- IL-1β and TNF-α (primary inflammatory cytokines)
- IL-6, IL-8 (CXCL8), and matrix metalloproteinases (MMPs)
These cytokines activate endothelial cells in cerebral vessels, upregulating adhesion molecules (ICAM-1, VCAM-1, E-selectin).
Step 4: BBB Disruption
Neutrophil-derived MMPs and cytokine-mediated endothelial injury disrupt tight junctions of the BBB. This leads to:
- Vasogenic edema (protein-rich fluid leaks across damaged BBB)
- Increased CSF protein (hallmark lab finding)
- Further influx of inflammatory cells and plasma proteins into CSF
Step 5: Cerebral Edema and Raised ICP
Three types of edema combine to raise intracranial pressure (ICP):
- Vasogenic - BBB disruption
- Cytotoxic - direct neuronal injury from toxins, ischemia
- Interstitial - impaired CSF absorption due to inflammation blocking arachnoid villi
Raised ICP leads to decreased cerebral perfusion pressure (CPP = MAP - ICP), causing brain ischemia.
Step 6: Vascular Complications
Inflammation causes vasculitis, vasospasm, arterial or venous thrombosis, and DIC (disseminated intravascular coagulation). The consequences include:
- Cortical infarction
- Cranial nerve palsies (due to involvement of CN III, VI, VII at the skull base)
- Cerebral venous sinus thrombosis (occurs in ~1% of meningitis cases)
Step 7: Neuronal Injury and Death
Neuronal damage results from direct cytotoxicity (apoptosis triggered by bacterial toxins), excitotoxicity (glutamate release during ischemia), and mitochondrial dysfunction. Survivors may have permanent sequelae: sensorineural hearing loss (most common), cognitive impairment, focal neurologic deficits, hydrocephalus.
Bactericidal antibiotics themselves worsen the cytokine storm initially - this is why dexamethasone given BEFORE antibiotics is a key therapeutic principle (it blocks TNF-α at the mRNA level before macrophages are activated by endotoxin). Harrison's, p. 1163-1164
5. Clinical Presentation
Classic Triad (present in only ~45% of patients):
- Fever
- Severe headache (worst of life; thunderclap in onset)
- Nuchal rigidity (neck stiffness)
The 4th symptom, altered mental status / photophobia, is also highly characteristic. Rosen's, p. 4166
Early Symptoms (prodrome, hours to 1-2 days):
- Fever, malaise, myalgia
- Non-specific headache that rapidly worsens
- Nausea and vomiting
- Photophobia and phonophobia
- In meningococcemia: non-blanching petechial rash beginning on extremities, rapidly becoming purpuric
Evolving / Advanced Symptoms:
- Altered consciousness (confusion, drowsiness, coma) - from raised ICP and cortical spread
- Seizures - from cortical irritation or infarction
- Focal neurologic deficits - CN palsies, hemiparesis
- Papilledema - sign of markedly raised ICP
- Bulging fontanelle - in infants instead of neck stiffness
- Waterhouse-Friderichsen syndrome - bilateral adrenal hemorrhage in fulminant meningococcemia with DIC and purpura fulminans
Special Populations:
- Neonates: subtle and non-specific - poor feeding, altered tone, irritability, temperature instability (may be hypothermic), bulging fontanelle. Classic signs absent in most <3 months old.
- Elderly/Immunosuppressed: altered mental status may be the ONLY finding. Classic triad may be absent.
- Tuberculous meningitis: insidious onset over weeks/months; low-grade fever, night sweats, weight loss, progressively worsening headache, cranial nerve palsies at skull base.
- Fungal meningitis: headache, low-grade fever, malaise, weight loss - subtle enough that CNS infection is often not initially suspected.
Rosen's, p. 4166-4167
6. Diagnostic Criteria and Scoring
Jolt Accentuation Test (Early Diagnostic Clue)
In patients with fever and headache, ask them to rotate their head horizontally 2-3 times per second. Worsening of headache = positive and suggests meningeal irritation (sensitivity ~97% for viral meningitis, when combined with other findings).
7. Physical Examination Tests for Clinical Diagnosis
A. Kernig's Sign
- Technique: Patient lies supine. Flex the hip to 90°. Attempt to extend the knee.
- Positive: Inability to extend the knee beyond 135° due to pain/resistance from hamstring spasm
- Mechanism: Inflammation of meninges causes pain when the sciatic nerve root (which runs through the inflamed SAS) is stretched
- Sensitivity: <12% | Specificity: high (>95%)
- Interpretation: Low sensitivity means a negative Kernig's does NOT rule out meningitis. But positive = strong clinical suspicion.
B. Brudzinski's Sign
- Technique: Patient lies supine. Passively flex the neck (bring chin to chest).
- Positive: Involuntary flexion of hips and knees occurs
- Mechanism: Passive neck flexion stretches the inflamed spinal meninges, and the patient reflexively flexes the hips and knees to reduce tension on the meninges
- Sensitivity: <12% | Specificity: high
- Clinical note: Same interpretation as Kernig's - high specificity makes it useful when positive.
Rosen's Emergency Medicine, p. 4168
C. Nuchal Rigidity
- Technique: With patient supine, attempt passive flexion of the neck.
- Positive: Resistance to flexion; patient cannot touch chin to chest
- Mechanism: Meningeal irritation and paraspinal muscle spasm protecting inflamed nerve roots
- Most sensitive of the three clinical signs for meningitis
D. Brudzinski's Contralateral Leg Sign
- Passive flexion of one leg causes contralateral leg to also flex reflexively.
E. Jolt Accentuation of Headache
- Horizontal head rotation at 2-3 Hz worsens headache. High sensitivity for meningeal inflammation.
F. Fundoscopic Examination
- Check for papilledema (blurred disc margins, loss of venous pulsations) before LP to assess for raised ICP
- Bedside ocular ultrasound (optic nerve sheath diameter >5 mm) is an alternative for ICP assessment
G. Skin Examination
- Petechiae/purpura on extremities (and trunk) = hallmark of meningococcemia
- A non-blanching rash in a febrile patient is meningococcal meningitis until proven otherwise
H. Signs of Source Infection
- Examine ears (otitis media), sinuses, skin (abscess), heart (murmur of endocarditis), spine (paraspinal tenderness)
8. Diagnostic Approach
Step 1: Clinical Assessment + Risk Stratification
Determine if the patient needs CT BEFORE lumbar puncture (LP). CT first is indicated if ANY of:
- Papilledema
- New focal neurologic deficit
- Altered level of consciousness
- New-onset seizures
- History of CNS mass lesion / immunosuppression
If none of the above are present, proceed directly to LP. Do NOT delay LP unnecessarily - diagnostic delay worsens outcomes.
Step 2: Blood Cultures
Draw before antibiotics (two sets). Positive in ~50-80% of bacterial meningitis cases. If LP is delayed for CT, draw blood cultures and start empiric antibiotics IMMEDIATELY - do not wait for LP results.
Step 3: Lumbar Puncture and CSF Analysis
This is the definitive diagnostic test.
| Parameter | Normal | Bacterial | Viral | Fungal/TB |
|---|---|---|---|---|
| Opening Pressure | 70-180 mmH₂O | Markedly elevated (>200-300) | Normal/slightly elevated | Elevated |
| Appearance | Clear | Turbid/purulent | Clear | Clear/slightly turbid |
| WBC (cells/µL) | <5 | >1000, PMN dominant | 10-500, lymphocyte dominant | 10-500, lymphocytes |
| Protein (g/L) | 0.15-0.45 | Markedly elevated (>1.0) | Normal/mildly elevated | Elevated |
| Glucose (CSF:serum ratio) | >0.6 | Low (<0.4) - bacteria consume glucose | Normal (>0.6) | Low (TB/fungal) |
| Gram stain | Negative | Positive in 60-90% | Negative | India ink (Cryptococcus) |
| Culture | Negative | Positive in 70-85% | Negative | Positive (slow) |
CSF glucose is low in bacterial meningitis because bacteria actively consume glucose in the CSF. This is a key differentiator from viral meningitis where glucose remains normal.
Step 4: Additional CSF Tests
- PCR (most sensitive for viral causes): HSV, enterovirus, CMV, EBV
- Latex agglutination / antigen testing: rapid bedside detection of S. pneumoniae, N. meningitidis, H. influenzae, GBS
- India ink preparation: identifies Cryptococcus capsule (sensitivity ~50%)
- Cryptococcal antigen (CrAg): sensitivity >90% for Cryptococcal meningitis
- AFB smear and culture + ADA (adenosine deaminase): for TB meningitis (culture takes weeks; ADA >10 U/L suggests TB)
- Metagenomics / next-generation sequencing of CSF: emerging tool for undiagnosed cases
Henry's Clinical Diagnosis and Management, p. 3807-3851; Tietz Textbook, p. 3157
Step 5: Neuroimaging
- CT head: rule out mass effect before LP; may show meningeal enhancement, hydrocephalus, abscess, empyema, infarction
- MRI brain with gadolinium: more sensitive; shows leptomeningeal enhancement, vasculitis, early ischemia, cranial nerve involvement. Superior for TB and fungal meningitis.
Step 6: Blood Tests
- CBC (leukocytosis with left shift in bacterial; lymphocytosis in viral)
- CMP, serum glucose (for CSF:serum glucose ratio)
- CRP, procalcitonin (PCT >0.5 ng/mL strongly suggests bacterial over viral)
- Blood cultures x2
- Coagulation studies / DIC screen in meningococcemia
- HIV serology (if unknown status - cryptococcal and TB meningitis are common in HIV)
9. Treatment Approach
A. Empiric Antibiotic Therapy (start within 30 min of diagnosis)
DO NOT DELAY antibiotics while waiting for CT or LP results if clinical suspicion is high.
| Patient Group | Empiric Regimen |
|---|---|
| Adults 18-50 years | Ceftriaxone 2g IV q12h |
| Adults >50 years or immunocompromised | Ceftriaxone 2g IV q12h + Ampicillin 2g IV q4h (covers Listeria) |
| Neonates | Ampicillin + Cefotaxime (or Gentamicin) |
| Post-neurosurgery/shunt/nosocomial | Vancomycin + Ceftazidime (or Meropenem) |
| Penicillin allergy | Chloramphenicol ± Vancomycin |
Harrison's, p. 1163
B. Pathogen-Directed Therapy (once cultures/sensitivities known)
| Organism | Drug of Choice | Duration |
|---|---|---|
| S. pneumoniae (penicillin-sensitive) | Penicillin G or Ceftriaxone | 10-14 days |
| S. pneumoniae (resistant) | Ceftriaxone + Vancomycin ± Rifampicin | 10-14 days |
| N. meningitidis | Penicillin G or Ceftriaxone | 5-7 days |
| Listeria monocytogenes | Ampicillin (+ Gentamicin in critically ill) | ≥21 days |
| H. influenzae | Ceftriaxone | 7-10 days |
| S. aureus (MSSA) | Nafcillin | Variable |
| MRSA | Vancomycin (± intraventricular vancomycin if no response) | Variable |
| Gram-negative bacilli | Ceftriaxone, Ceftazidime, or Meropenem | 21 days |
Harrison's, p. 1163-1164
C. Adjunctive Dexamethasone - CRITICAL
Dexamethasone 10 mg IV every 6 hours for 4 days, given 15-20 minutes BEFORE the first dose of antibiotics.
Mechanism: Dexamethasone blocks TNF-α and IL-1β synthesis at the mRNA level in macrophages and microglia - but ONLY if given BEFORE endotoxin activates them. Antibiotics lyse bacteria, releasing more endotoxin and driving cytokine production. Dexamethasone pre-treatment prevents this amplification.
Evidence: A prospective European RCT showed dexamethasone reduced unfavorable outcomes (15% vs 25%, p=.03) and death (7% vs 15%, p=.04), with most benefit in pneumococcal meningitis. It also significantly reduces the incidence of sensorineural hearing loss.
- Harrison's, p. 1164
Note: Dexamethasone reduces the penetration of vancomycin into CSF (by reducing inflammation). If MRSA or penicillin-resistant pneumococcus is suspected, consider adding rifampicin to ensure adequate CSF coverage.
D. Viral Meningitis Treatment
- Supportive care: hydration, antipyretics, analgesics (may need opioids for severe headache)
- No antiviral agents are effective for enteroviral meningitis
- Exception: HSV meningitis/encephalitis - treat with Acyclovir 10 mg/kg IV q8h
- Most patients recover fully in <1 week (children) to <3 weeks (adults)
- Hospitalization may not be needed for adults who appear well IF bacterial meningitis is confidently excluded
E. Tuberculous Meningitis
- Standard RHEZ regimen: Rifampicin + Isoniazid + Pyrazinamide + Ethambutol for 2 months, then Rifampicin + Isoniazid for 10 months (total 12 months)
- Dexamethasone is indicated as adjunctive therapy (proven mortality benefit in HIV-negative patients)
- Paradoxical reactions can occur (immune reconstitution inflammatory syndrome in HIV patients on ART)
F. Cryptococcal Meningitis
- Induction: Amphotericin B deoxycholate (0.7-1 mg/kg/day) + Flucytosine (25 mg/kg q6h) for 2 weeks
- Consolidation: Fluconazole 400 mg/day for 8 weeks
- Maintenance: Fluconazole 200 mg/day (indefinitely in HIV unless immune reconstitution on ART)
- Repeated therapeutic LPs (or lumbar drain) to manage elevated ICP - a major cause of early mortality
G. ICP Management
- Head of bed elevation 30°
- Avoid hypotonic fluids
- Mannitol for acute herniation
- Seizure prophylaxis if seizures occur (levetiracetam preferred)
- External ventricular drain (EVD) if hydrocephalus develops
10. Clinical Example
Case: Meningococcal Meningitis
Patient: Ahmed, a 19-year-old university student living in a dormitory presents to the ED at 2 AM with:
- 12 hours of rapidly worsening severe headache ("worst headache of my life")
- Fever of 39.8°C
- Neck stiffness - refuses to look down
- Photophobia - covering eyes with arm
- Nausea and vomiting x3 over past 6 hours
- His roommate had been "sick with a cold" last week
Physical Examination Findings:
- GCS: 14/15 (slightly confused)
- Temperature: 39.8°C, HR 118 bpm, BP 108/70 mmHg
- Nuchal rigidity: Positive (cannot flex neck, chin to chest impossible)
- Kernig's sign: Positive bilaterally (cannot straighten knees beyond 100°)
- Brudzinski's sign: Positive (neck flexion causes involuntary hip flexion)
- Skin: Multiple 2-5 mm non-blanching petechiae over the lower limbs and trunk, several evolving to purpuric lesions
- Fundoscopy: Venous pulsations present (no papilledema = LP is safe to proceed)
Emergency Actions (these happen simultaneously, within 15 minutes):
- Dexamethasone 10 mg IV - administered FIRST
- Blood cultures x2 drawn
- Ceftriaxone 2g IV given immediately after dexamethasone
- LP performed (no CT needed - no papilledema, no focal deficits, no altered consciousness)
CSF Results:
- Opening pressure: 320 mmH₂O (elevated)
- Appearance: Cloudy
- WBC: 4,200 cells/µL (98% neutrophils)
- Protein: 2.8 g/L (elevated; normal <0.45)
- Glucose CSF: 1.2 mmol/L; Serum glucose: 5.5 mmol/L → CSF:serum ratio = 0.22 (low; normal >0.6)
- Gram stain: Gram-negative diplococci in pairs (kidney-bean shaped) within neutrophils
- Culture: N. meningitidis serogroup B (reported 24h later)
- Blood cultures: N. meningitidis (positive)
Interpretation: Classic bacterial meningitis pattern - elevated pressure, neutrophilic pleocytosis, high protein, low glucose, positive Gram stain.
Treatment:
- Continue Ceftriaxone 2g IV q12h for 5-7 days (N. meningitidis remains penicillin-sensitive; can de-escalate to penicillin G)
- Continue Dexamethasone 10 mg IV q6h for 4 days
- Close contacts: Rifampicin 600 mg orally bd x2 days, or Ciprofloxacin single dose (chemoprophylaxis)
- Notify public health authorities
Outcome: Ahmed responded well after 48 hours on treatment - fever resolved, headache improved, CSF sterilized at 36 hours. He was discharged after 7 days with no neurologic sequelae. The petechial lesions faded. His audiogram was normal (dexamethasone benefit). His dormitory contacts received chemoprophylaxis.
Pathophysiology Teaching Point in This Case:
The petechiae are NOT simply due to "infection spreading to skin." They result from N. meningitidis causing endothelemia - bacteria enter the bloodstream and release endotoxin (LPS), activating the complement cascade and coagulation pathway, causing microvascular damage, platelet consumption (DIC), and capillary leak. The result is the characteristic non-blanching rash. In fulminant cases, this progresses to purpura fulminans, bilateral adrenal hemorrhage (Waterhouse-Friderichsen syndrome), and septic shock within hours.
11. Key Complications to Monitor
| Complication | Mechanism | Clinical Sign |
|---|---|---|
| Sensorineural hearing loss | Cochlear inflammation via perilymphatic duct from SAS | Post-illness audiogram |
| Hydrocephalus | Obstruction of arachnoid villi by exudate | Worsening headache, vomiting, papilledema |
| Cerebral infarction | Arteritis, venous thrombosis | New focal deficits, seizures |
| Subdural empyema | Pus collection over cortex | Fever, focal signs, progressive alteration |
| DIC | Endotoxin-driven coagulation activation | Petechiae, bleeding, low platelets |
| SIADH | Hypothalamic inflammation | Hyponatremia, seizures |
| Waterhouse-Friderichsen | Bilateral adrenal hemorrhage (meningococcal) | Adrenal insufficiency + DIC |
Recent Evidence Note
A 2025 systematic review and meta-analysis (PMID 39672463) examined biomarkers in paediatric bacterial meningitis and confirmed that CSF white cell count, protein, and glucose remain the cornerstones of diagnosis. A 2026 meta-analysis (PMID 41616789) raised important concern about antimicrobial resistance in S. pneumoniae, N. meningitidis, and H. influenzae (2010-2024), reinforcing that empiric therapy must cover resistant strains (especially PRSP - penicillin-resistant S. pneumoniae) with ceftriaxone + vancomycin pending sensitivities.
References:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 143 - Acute Meningitis
- Robbins & Kumar Basic Pathology, p. 833-834
- Rosen's Emergency Medicine, Ch. 95, p. 4164-4177
- Goldman-Cecil Medicine International Edition, Ch. 381
- Tietz Textbook of Laboratory Medicine, 7th Ed., p. 3157
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 3807-3851
This is a shared conversation. Sign in to Orris to start your own chat.