Renal function test and biomarkers
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the content needed to compile a thorough, well-structured answer. Here is the complete guide to Renal Function Tests and Biomarkers:
Renal Function Tests (RFT) and Biomarkers
Overview
Laboratory tests for renal function are among the most commonly performed in clinical chemistry. They span traditional filtration markers (creatinine, BUN), estimation equations for GFR, urinalysis, and a growing panel of novel biomarkers for early detection of acute kidney injury (AKI) and chronic kidney disease (CKD). The key challenge is that conventional markers like serum creatinine detect injury only after substantial nephron loss has already occurred.
1. Traditional / Conventional RFT
A. Serum Creatinine
Creatinine is an end-product of muscle creatine metabolism (MW ~113 Da), freely filtered at the glomerulus, and secreted (to a minor degree) in the tubule. It is the most widely used clinical proxy for GFR.
Reference ranges:
- Males: ~0.7-1.2 mg/dL
- Females: ~0.5-1.0 mg/dL
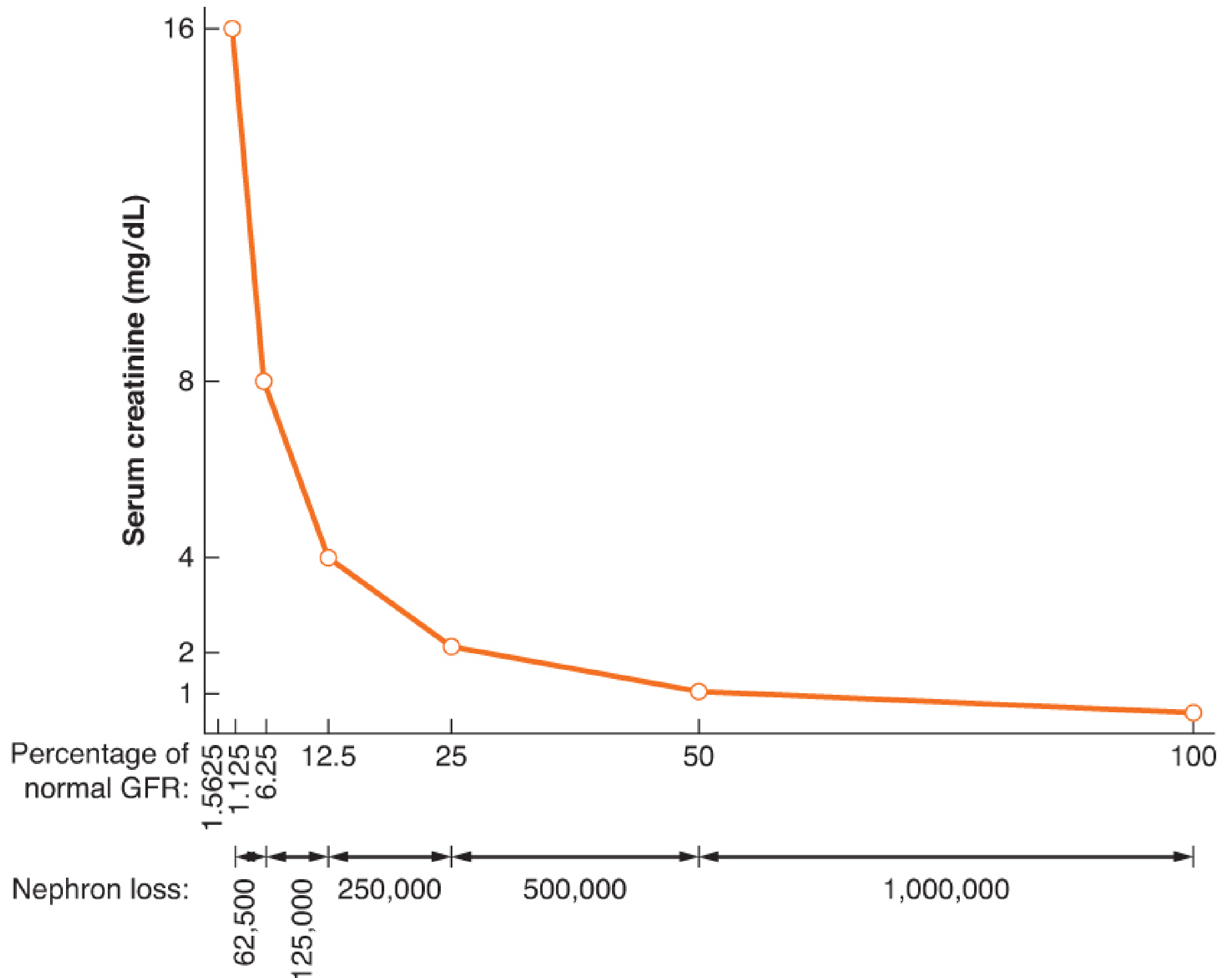
Critical limitation - the "creatinine blind spot": The relationship between GFR and serum creatinine is nonlinear and logarithmic. A 50% loss of nephron mass (GFR drop from 120 to ~60 mL/min) produces only a modest rise in serum creatinine from ~1.0 to ~2.0 mg/dL. Conversely, renal function must decline by ~50% before a measurable change in creatinine is seen. This is the so-called "creatinine blind spot."
Specific limitations of creatinine (Brenner and Rector's The Kidney):
- Muscle mass effect - Production varies greatly with age, sex, and muscle mass (24-hr creatinine excretion falls from 23.8 mg/kg in men aged 20-29 to 9.8 mg/kg in men aged 90-99)
- Non-specificity for tubular injury - Does not distinguish prerenal, intrinsic, or postrenal causes; cannot localize glomerular vs. tubular vs. proximal vs. distal injury
- Lag time - Static measurements do not reflect real-time GFR changes; creatinine accumulates over hours to days
- Drug interference - Cimetidine and trimethoprim inhibit tubular secretion, raising creatinine without affecting true GFR
- Assay interference - The Jaffé (alkaline picrate) method overestimates creatinine by ~25% due to noncreatinine chromogens (proteins, glucose, acetoacetate)
- CKD misclassification - Small changes in serum creatinine in patients with pre-existing CKD may falsely classify them as having AKI
Measurement methods:
- Jaffé (alkaline picrate) reaction - standard but subject to chromogen interference
- Enzymatic assays (creatininase method) - more specific, preferred in diabetic patients
B. Blood Urea Nitrogen (BUN)
Urea is the primary end-product of protein/amino acid catabolism, synthesized in the liver and excreted by kidneys. BUN (normal range: ~7-20 mg/dL) has significant limitations as a kidney function marker:
- Highly non-specific - BUN rises with high protein intake, catabolic states (fever, burns, trauma, corticosteroids, sepsis), GI bleeding, and decreased tubular flow (dehydration, obstruction)
- Tubular reabsorption - Urea is passively reabsorbed in tubules; anything that slows tubular flow (volume depletion) raises BUN disproportionately
- BUN:Creatinine ratio - >20:1 suggests prerenal azotemia; <10:1 may suggest liver disease or malnutrition
- Advanced CKD - Averaging urea clearance and creatinine clearance can be more accurate at low GFR, since creatinine clearance overestimates and urea clearance underestimates true GFR
(Barash's Clinical Anesthesia; Brenner and Rector's The Kidney)
C. Creatinine Clearance and eGFR
Measured Creatinine Clearance (CrCl):
- Formula: CrCl = (Urine Creatinine × Urine Volume) / Serum Creatinine
- Requires 24-hour urine collection; prone to collection errors (skipped voids = underestimation)
- Overestimates true GFR because of tubular secretion of creatinine
Estimated GFR (eGFR) equations:
- Cockcroft-Gault: uses age, sex, weight, and serum creatinine
- MDRD (4-variable): uses age, sex, race, and serum creatinine
- CKD-EPI: more accurate across the range of GFR; preferred current standard
- CKD-EPI Cystatin C equation: combines creatinine + cystatin C for improved accuracy
GFR-based CKD staging (KDIGO):
| Stage | GFR (mL/min/1.73m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal/high |
| G2 | 60-89 | Mildly decreased |
| G3a | 45-59 | Mild-moderate decrease |
| G3b | 30-44 | Moderate-severe decrease |
| G4 | 15-29 | Severely decreased |
| G5 | <15 | Kidney failure |
D. Urinalysis
A core component of every renal evaluation (Barash's Clinical Anesthesia):
Dipstick tests:
- Protein - Semiquantitative; positive result prompts 24-hr protein quantification (proteinuria >3.5 g/day = nephrotic range). Types: glomerular, tubular, overflow, tissue
- Blood/hematuria - >2 RBCs/HPF is abnormal; may indicate glomerulonephritis, stones, or infection
- Glucose - Indicates either hyperglycemia or proximal tubular dysfunction (Fanconi syndrome)
- Nitrites/leukocyte esterase - Screens for UTI
- pH, specific gravity - Reflects concentrating ability (normal SG 1.001-1.035; >1.018 indicates preserved concentrating function)
Urine Microscopy:
- Granular/muddy brown casts - Diagnostic of acute tubular necrosis (ATN)
- Red cell casts - Pathognomonic of glomerulonephritis
- White cell casts - Acute pyelonephritis or interstitial nephritis
- Fatty casts (oval fat bodies) - Nephrotic syndrome
Urine Electrolytes:
- Urine sodium <20 mEq/L - Prerenal (kidney retaining sodium)
- Urine sodium >40 mEq/L - Intrinsic renal injury (tubular inability to retain sodium)
- Fractional Excretion of Sodium (FENa) <1% - Prerenal; >2% - ATN
2. Novel Filtration Markers
Cystatin C
Cystatin C is a 13-kDa cysteine protease inhibitor produced at a constant rate by all nucleated cells. It is:
- Freely filtered at the glomerulus
- Neither secreted nor reabsorbed, but fully catabolized by proximal tubular cells (making urinary cystatin C a tubular injury marker)
- Less influenced by muscle mass than creatinine
- Short half-life (~2 hours) - responds more rapidly to acute changes in GFR
Advantages over creatinine:
- Better predictor of risk for death and ESRD across diverse populations
- Elevated in >50% of persons aged >80 (reflecting true GFR decline in elderly)
- CKD-EPI Cystatin C equation improves CKD classification and risk stratification vs. creatinine-based equations alone
- Serum cystatin C also associated with cardiovascular risk
Limitations: Elevated in males, taller/heavier patients, and those with higher lean body mass - similar confounders to creatinine
(Brenner and Rector's The Kidney; Miller's Anesthesia)
Proenkephalin A 119-159 (penKid)
A peptide derived from enkephalins, correlated with GFR, and emerging as a promising acute filtration marker in ICU settings. (Miller's Anesthesia)
3. Novel Tubular Injury Biomarkers (AKI Biomarkers)
These markers detect injury at the cellular level, filling the "opportunity gap" between normal renal function and cell death, where changes in GFR and serum creatinine are not yet apparent. (Current Surgical Therapy 14e)
RIFLE and KDIGO AKI Staging (for context)
RIFLE Criteria:
| Category | Serum Creatinine/GFR Change | Urine Output |
|---|---|---|
| Risk (R) | SCr >1.5× or GFR decrease >25% | <0.5 mL/kg/h for >6 h |
| Injury (I) | SCr >2× or GFR decrease >50% | <0.5 mL/kg/h for >12 h |
| Failure (F) | SCr >3× or GFR decrease >75% | <0.3 mL/kg/h for >24 h |
| Loss (L) | SCr >4 mg/dL; complete loss >4 weeks | Anuria >12 h |
| ESRD (E) | End-stage >3 months | - |
KDIGO AKI Stages:
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | >0.3 mg/dL rise OR >150-200% | <0.5 mL/kg for >6 h |
| 2 | >200-300% | <0.5 mL/kg for >12 h |
| 3 | >300% or ≥4 mg/dL (acute rise >0.5 mg/dL) | <0.3 mL/kg for >24 h or anuria >12 h |
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
A. Kidney Injury Molecule-1 (KIM-1)
- Type I cell membrane glycoprotein with an immunoglobulin-like domain and mucin domain
- KIM-1 mRNA increases more than any other known gene after kidney injury
- Its ectodomain is shed into urine after proximal tubular injury
- Earlier diagnostic indicator of AKI than plasma creatinine or BUN in preclinical and clinical studies
- High specificity - no systemic source detected; expression limited to the kidney
- Induced by many nephrotoxins: cisplatin, cyclosporin, cadmium, gentamicin, mercury, chromium
- NGAL is more sensitive at earliest time points; KIM-1 adds specificity at later time points
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
B. Neutrophil Gelatinase-Associated Lipocalin (NGAL)
- 25-kDa protein initially identified bound to gelatinase in neutrophil granules
- Also known as lipocalin-2 (LCN2) or human neutrophil lipocalin (HNL)
- Synthesized during granulocyte maturation; induced in epithelial cells during inflammation
- Detectable in urine as early as 3 hours after cisplatin administration in animal models
- Most sensitive marker at earliest time points after AKI
- Validated in pediatric and adult patients undergoing cardiopulmonary bypass (CPB) for cardiac surgery
- Available as both serum and urine measurements
- Limitations: also elevated in inflammatory conditions (sepsis, malignancy), reducing specificity
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
C. Interleukin-18 (IL-18)
- 18-kDa proinflammatory cytokine activated by caspase-1
- Produced by renal tubule cells and macrophages; mediates neutrophil and monocyte infiltration in tubular injury
- In humans, IL-18 is induced and cleaved mainly in proximal tubules and released into urine
- Participates in: ischemia-reperfusion injury, allograft rejection, infection, autoimmune disease, and malignancy
- Measured by commercially available ELISA and microbead assays
- TRIBE-AKI Study (1,219 adults undergoing cardiac surgery): IL-18 significantly predicted AKI before creatinine rise
- Higher IL-18 in acute tubular necrosis vs. prerenal azotemia or UTI (original validation study by Parikh et al., 72 patients)
(Brenner and Rector's The Kidney)
D. Fatty Acid-Binding Protein (FABP)
- Liver-type (L-FABP) and heart-type (H-FABP) variants both studied as AKI biomarkers
- H-FABP is a promising biomarker particularly in cardiac surgery and ICU-associated AKI
E. α1-Microglobulin
- Low-molecular-weight glycoprotein (~27-30 kDa); member of the lipocalin superfamily
- Primarily synthesized by liver; freely filtered at glomerulus and completely reabsorbed/catabolized by normal proximal tubule (via megalin-mediated uptake)
- Urinary α1-microglobulin elevation = proximal tubular injury or dysfunction
- Reference ranges: <13 mg/g creatinine (age <50); <20 mg/g creatinine (age ≥50)
- More stable than β2-microglobulin across a range of urine pH, making it a more reliable biomarker
- Associated with increased risk of CKD and all-cause mortality
(Brenner and Rector's The Kidney)
F. N-acetyl-β-D-glucosaminidase (NAG)
- Lysosomal enzyme from proximal tubular cells; too large to be filtered, so any urinary NAG = tubular cell damage
- Sensitive marker of tubular injury in diabetic nephropathy and nephrotoxin exposure
G. TIMP-2 × IGFBP-7 (Cell Cycle Arrest Markers)
- Urinary TIMP-2 (tissue inhibitor of metalloproteinase-2) × IGFBP-7 (insulin-like growth factor binding protein-7) product
- Both are G1 cell cycle arrest markers expressed in stressed tubular cells before injury manifests
- FDA-cleared NephroCheck® test
- Clinical utility: Urinary TIMP-2 × IGFBP-7 is associated with increased risk of KDIGO stage 2 or 3 AKI within the next 12 hours in ICU patients at high risk for AKI
- AUC ~0.80 in validation studies
(Brenner and Rector's The Kidney - Key Points)
H. Hepcidin-25
- An iron-regulatory peptide showing promise in cardiac surgery AKI
- Lower urinary hepcidin-25 on postoperative day 1 is associated with AKI development
- AUC ~0.80 in preliminary studies
- Combining hepcidin-25 with postoperative NGAL improves AUC to ~0.84
(Brenner and Rector's The Kidney)
I. Other Novel Biomarkers (Emerging)
| Biomarker | Origin/Mechanism | Key Feature |
|---|---|---|
| N-acetyl-β-D-glucosaminidase (NAG) | Proximal tubule lysosomal enzyme | Sensitive nephrotoxin marker |
| Uromodulin (Tamm-Horsfall protein) | Thick ascending limb | CKD progression marker |
| MicroRNA | Cellular stress/injury | Promising early detection |
| Monocyte chemoattractant protein-1 (MCP-1) | Inflammatory | Cardiac surgery AKI |
| TGFR1, TGFR2, EGF, plasma KIM-1 | Growth factor signaling | Markers for incident/progressive CKD |
4. CKD-Specific Biomarkers
Beyond GFR and proteinuria (the two pillars of CKD classification):
- Plasma TGFR1, TGFR2 - TGF-β pathway markers increasingly recognized as markers of CKD progression
- Plasma EGF - Epidermal growth factor; associated with CKD progression
- Urinary α1-microglobulin - Associated with CKD development and all-cause mortality
- Serum cystatin C - Predicts cardiovascular morbidity and mortality even beyond its GFR-estimating role
- Albuminuria - 30-300 mg/day = microalbuminuria (early diabetic nephropathy); >300 mg/day = macroalbuminuria
(Brenner and Rector's The Kidney)
5. Summary Comparison Table
| Biomarker | Source | Detects | Timing of Rise | Advantages | Limitations |
|---|---|---|---|---|---|
| Serum Creatinine | Muscle | GFR | 24-48 h after injury | Cheap, ubiquitous | Muscle mass dependent; nonspecific; late marker |
| BUN | Protein catabolism | GFR (indirect) | Concurrent with SCr | Cheap | Highly non-specific; diet/catabolism dependent |
| Cystatin C | All nucleated cells | GFR | Earlier than SCr | Muscle mass independent; short T½ | Influenced by body composition; expensive |
| NGAL | Proximal tubule (and neutrophils) | Tubular injury | 2-4 hours | Earliest marker; sensitive | Less specific in infection/inflammation |
| KIM-1 | Proximal tubule | Tubular injury | 6-12 hours | Kidney-specific; nephrotoxin sensitive | Moderate sensitivity vs. NGAL early |
| IL-18 | Proximal tubule | Ischemic tubular injury | 6-12 hours | Distinguishes ATN from prerenal | Less studied in sepsis AKI |
| α1-Microglobulin | Proximal tubule | Proximal tubular dysfunction | Early | Stable across pH range | Age-dependent normal range |
| TIMP-2 × IGFBP-7 | Tubular stress | Cell cycle arrest/stress | Before injury | Predictive (12 h ahead); FDA-cleared | Requires specialized assay |
| NAG | Proximal tubule lysosomes | Tubular cell damage | Early | Not filtered; purely tubular origin | Non-specific across tubular insults |
| Uromodulin | Thick ascending limb | CKD/tubular integrity | CKD progression | CKD-specific | Less validated in AKI |
Clinical Takeaways
- Serum creatinine and BUN detect injury only after at least 50% nephron loss - they are "lagging indicators."
- Novel biomarkers (NGAL, KIM-1, IL-18, TIMP-2 × IGFBP-7) detect subclinical tubular injury in the window before creatinine rises.
- Cystatin C is the best validated replacement for creatinine as a GFR marker, especially in the elderly, low muscle mass, or obesity.
- NGAL is the most sensitive early marker; KIM-1 adds kidney-specificity at later time points.
- TIMP-2 × IGFBP-7 is the only FDA-cleared test for AKI risk stratification in ICU patients.
- Urinalysis + microscopy remains an essential and cost-free component of every renal evaluation - muddy brown casts are pathognomonic of ATN.
Sources:
- Henry's Clinical Diagnosis and Management by Laboratory Methods (AKI biomarkers, RIFLE/KDIGO staging)
- Brenner and Rector's The Kidney, 2-Volume Set (cystatin C, α1-microglobulin, creatinine limitations, CKD biomarkers)
- Barash, Cullen, and Stoelting's Clinical Anesthesia (urinalysis, GFR-creatinine relationship, BUN)
- Miller's Anesthesia, 10e (novel biomarkers, cystatin C, penKid)
- Current Surgical Therapy, 14e (AKI biomarker candidate overview)
This is a shared conversation. Sign in to Orris to start your own chat.