Gordon syndrome
Reading File
search_medical_text
Gordon syndrome pseudohypoaldosteronism type 2 clinical features genetics
search_medical_text
Gordon syndrome hyperkalemia hypertension WNK kinase diagnosis treatment
GradeResponse
GradeResponse
search_medical_text
pseudohypoaldosteronism type 2 hyperkalemia hypertension thiazide diuretics pathophysiology
Based on what was retrieved and my medical knowledge, here is a comprehensive overview of Gordon syndrome.
Gordon Syndrome (Pseudohypoaldosteronism Type II / PHA II)
Gordon syndrome, also called Pseudohypoaldosteronism Type II (PHA II) or familial hyperkalemic hypertension (FHH), is a rare inherited disorder of renal tubular electrolyte handling characterized by the triad of hyperkalemia, hypertension, and normal or reduced GFR, despite otherwise normal or elevated aldosterone levels. (Harrison's Principles of Internal Medicine, 21st Ed., p. 353, 2080)
Etiology & Genetics
Gordon syndrome is caused by gain-of-function mutations that enhance sodium chloride reabsorption in the distal nephron, particularly the distal convoluted tubule (DCT). The key molecular players are the WNK (With No lysine K) serine-threonine kinases:
| Gene | Locus | Inheritance | Notes |
|---|---|---|---|
| WNK1 | 12p13 | Autosomal dominant | Intronic deletion → overexpression |
| WNK4 | 17q21 | Autosomal dominant | Missense mutations → loss of inhibition of NCC |
| KLHL3 | 5q31 | AD or AR | Adaptor protein targeting WNKs for degradation |
| CUL3 | 2q36 | Autosomal dominant | E3 ubiquitin ligase; often de novo, more severe |
- CUL3 mutations tend to be de novo and cause the most severe phenotype, with earlier onset and more pronounced hyperkalemia and hypertension.
- The final common pathway is increased activity of the NCC (Na-Cl cotransporter, SLC12A3) in the DCT, leading to excess sodium reabsorption and impaired potassium/H⁺ secretion.
Pathophysiology
- ↑ NCC activity → increased Na⁺/Cl⁻ reabsorption in DCT
- ↓ Na⁺ delivery to the collecting duct → reduced driving force for potassium secretion via ROMK channels → hyperkalemia
- Volume expansion from Na⁺ retention → hypertension (aldosterone-independent)
- Reduced H⁺ secretion in collecting duct → metabolic acidosis (hyperchloremic)
- Aldosterone levels are normal or elevated but functionally "opposed" by downstream NCC activity — hence the "pseudohypoaldosteronism" misnomer
Clinical Features (Harrison's, p. 353, 2080)
- Hypertension — often severe, can present in childhood or early adulthood
- Hyperkalemia — chronic, often asymptomatic unless severe (muscle weakness, arrhythmia risk)
- Hyperchloremic metabolic acidosis (normal anion gap)
- Normal or reduced GFR (no intrinsic renal disease)
- Short stature — in some cases
- Muscle weakness — secondary to hyperkalemia
- Aldosterone levels normal or elevated but urinary K⁺ excretion paradoxically low
Diagnosis
Suspected when:
- Hypertension + hyperkalemia in the absence of renal insufficiency
- No medications (e.g., ACE inhibitors, potassium-sparing diuretics) causing hyperkalemia
- Family history of hypertension and/or hyperkalemia
Key laboratory findings:
| Finding | Value |
|---|---|
| Serum K⁺ | ↑ (often 5.5–7 mEq/L) |
| Serum Cl⁻ | ↑ (hyperchloremia) |
| Bicarbonate | ↓ (metabolic acidosis) |
| Plasma renin | Low–normal (suppressed by volume expansion) |
| Aldosterone | Normal or elevated |
| Urinary K⁺ excretion | Low relative to serum K⁺ |
| GFR | Normal or mildly reduced |
Differentiation from other causes of hyperkalemia + hypertension:
- Primary hyperaldosteronism: hyperkalemia is absent (hypokalemia instead)
- Chronic kidney disease: GFR is reduced and explains hyperkalemia
- PHA type I: presents in neonates, salt-wasting, hypotension — not hypertension
- Liddle syndrome: hypokalemia + low aldosterone (gain-of-function ENaC)
Genetic testing for WNK1, WNK4, KLHL3, CUL3 mutations confirms the diagnosis.
Treatment (Harrison's, p. 353)
The treatment of Gordon syndrome is remarkably effective and pharmacologically elegant — the molecular defect (excess NCC activity) is directly targeted:
First-Line: Thiazide Diuretics
- Hydrochlorothiazide or chlorthalidone — block NCC directly
- Often produce dramatic normalization of both blood pressure and serum potassium
- This therapeutic response is itself near-diagnostic
- Low doses are typically sufficient
Dietary
- Low-sodium diet — reduces substrate for excess NCC-mediated reabsorption
- Complements pharmacologic therapy
Additional Measures
- Correction of metabolic acidosis if severe (sodium bicarbonate supplementation)
- Avoid medications that worsen hyperkalemia (NSAIDs, ACE inhibitors/ARBs — use with caution, though paradoxically RAS blockade can help BP)
Prognosis
- Excellent with treatment — patients on thiazides have normalized electrolytes and blood pressure
- Untreated, chronic hypertension leads to cardiovascular and end-organ complications
- CUL3 mutations may require higher doses or combination therapy due to phenotypic severity
Summary
Gordon syndrome (PHA II) is a rare but clinically important monogenic cause of hypertension that should be suspected in any patient with hypertension + hyperkalemia + normal renal function. Its molecular basis in WNK-SPAK-NCC signaling makes it a model for understanding distal tubular physiology, and its exquisite response to thiazide diuretics makes it one of the most satisfying diagnoses in nephrology.
Perilunate dislocation x ray with explanation about how to diagnose it
Reading File
search_medical_image
perilunate dislocation wrist X-ray radiograph
search_medical_text
perilunate dislocation X-ray radiographic diagnosis findings Gilula arcs
GradeResponse
GradeResponse
Here is a comprehensive breakdown of how to diagnose perilunate dislocation on X-ray.
Perilunate Dislocation — X-Ray Diagnosis
The X-Ray
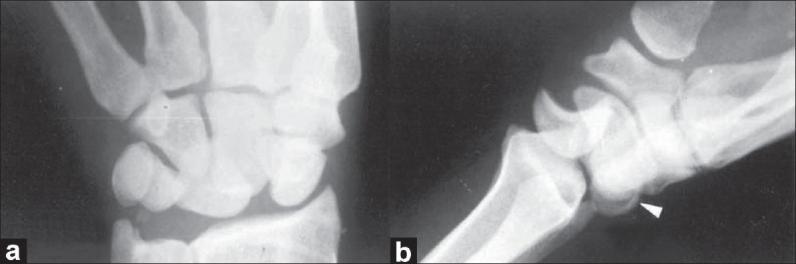
AP (left) and lateral (right) wrist radiographs demonstrating a dorsal perilunate dislocation. Note the disrupted carpal arcs on AP view, and the dorsally displaced capitate relative to a lunate that remains seated against the radius on the lateral view. An avulsion fracture of the dorsal horn of the lunate (white arrowhead) and ulnar styloid tip fracture are also visible.
What Is Perilunate Dislocation?
In a perilunate dislocation, the lunate stays in its normal fossa against the distal radius, but the entire rest of the carpus (led by the capitate) dislocates — most commonly dorsally — around it. This follows high-energy hyperextension injury (e.g., fall on outstretched hand, motor vehicle accident).
It sits in a progressive injury spectrum (Mayfield stages I–IV):
| Stage | Injury |
|---|---|
| I | Scapholunate dissociation |
| II | Capitolunate dislocation (perilunate) |
| III | Lunotriquetral disruption |
| IV | Lunate dislocation (lunate flips volar) |
How to Read the X-Ray: Step-by-Step
View 1: PA/AP Radiograph
Step 1 — Check Gilula's Lines (Three Carpal Arcs)
Gilula's lines are three smooth, parallel arcs drawn across the proximal carpal row in a normal wrist:
| Arc | Traces along |
|---|---|
| Arc I | Proximal articular surfaces of scaphoid, lunate, triquetrum |
| Arc II | Distal articular surfaces of scaphoid, lunate, triquetrum |
| Arc III | Proximal articular surfaces of capitate and hamate |
In perilunate dislocation: all three arcs are disrupted. The carpal bones overlap abnormally. The proximal and distal rows are no longer parallel.
Step 2 — Look at the Lunate Shape
- Normally the lunate appears quadrilateral on AP view
- In perilunate dislocation, it may appear triangular ("pie-shaped") due to rotational tilt — this is even more pronounced in a full lunate dislocation
Step 3 — Look for Carpal Crowding / Overlap
- The capitate appears superimposed over or proximally displaced relative to its normal position
- There is loss of joint space between the carpal rows
- The scapholunate interval may be widened >3 mm (Terry Thomas sign) if there is associated scapholunate ligament injury
Step 4 — Look for Associated Fractures
- Trans-scaphoid perilunate dislocation is the most common variant — the scaphoid fractures through its waist instead of the ligament tearing
- Also check for: radial styloid fracture, ulnar styloid avulsion fracture, lunate dorsal horn avulsion
View 2: Lateral Radiograph — The Key View
The lateral view is diagnostic and is where perilunate dislocation is most clearly identified.
The Normal Lateral Alignment Rule
On a true lateral wrist X-ray, three bones should form a straight line:
Radius → Lunate (cup) → Capitate (sits in lunate cup) → 3rd metacarpal
The capitate sits inside the concave distal surface of the lunate, and the lunate sits in the lunate fossa of the radius.
What You See in Perilunate Dislocation
| Structure | Position |
|---|---|
| Radius | Normal |
| Lunate | ✅ Remains seated in radial fossa — in normal position |
| Capitate | ❌ Displaced dorsally (posteriorly) — no longer sitting in the lunate cup |
| Rest of carpus | Rides dorsally with the capitate |
Memory aid: "The lunate stays, everything else runs away — dorsally."
In contrast, in lunate dislocation (Stage IV):
- The capitate returns to alignment with the radius
- But the lunate is spilled volar (anteriorly), often compressing the median nerve → carpal tunnel syndrome
Summary: AP vs Lateral Findings
| Feature | AP View | Lateral View |
|---|---|---|
| Gilula's arcs | Disrupted | N/A |
| Lunate shape | May appear triangular | Seated normally on radius |
| Capitate position | Overlapping/proximally displaced | Dorsally displaced off lunate |
| Scapholunate gap | May be >3 mm | — |
| Associated fractures | Scaphoid waist, radial/ulnar styloid | Lunate dorsal horn avulsion |
Common Pitfall
Perilunate dislocation is missed in up to 25% of cases on initial presentation because:
- The AP view can look deceptively subtle
- Swelling distracts from careful X-ray analysis
- The lateral view is not obtained or is a poor true lateral
Always get a true lateral view and trace the radius–lunate–capitate alignment in any wrist trauma with significant swelling or mechanism.
Next Steps After X-Ray Diagnosis
- CT scan — better delineates associated fractures (especially scaphoid)
- MRI — assesses ligamentous injury if CT is inconclusive
- Urgent orthopedic/hand surgery referral — closed reduction under anesthesia, followed by surgical fixation in most cases
- Monitor for median nerve injury (acute carpal tunnel syndrome) — present in ~25% of cases (Bailey & Love's Surgery, 28th Ed., p. 455)
This is a shared conversation. Sign in to Orris to start your own chat.