
Read this and tell me the probably diagnosis and treatment and progress and how much time will take to cure
microcytic hypochromic anemia low MCV MCH MCHC high RDW iron deficiency thalassemia diagnosis
low platelet count thrombocytopenia high MPV causes treatment
iron deficiency anemia treatment iron supplementation duration response hemoglobin recovery
low total protein low globulin hypoproteinemia causes malnutrition liver
Abnormal Values Summary
| Parameter | Result | Reference | Status |
|---|---|---|---|
| Hemoglobin | 9.7 g/dL | 12.0–16.0 | ↓ Low |
| Hematocrit | 33.5% | 36–48 | ↓ Low |
| MCV | 64.9 fL | 83–101 | ↓ Low |
| MCH | 18.9 pg | 26.4–33.2 | ↓ Low |
| MCHC | 29.1 g/dL | 31.8–35.9 | ↓ Low |
| RDW CV | 15.40% | 11.6–14 | ↑ High |
| RBC Count | 5.16 million/cmm | 3.8–4.8 | ↑ High |
| Platelet Count | 103,000/cmm | 150,000–410,000 | ↓ Low |
| MPV | 13.30 fL | 7.5–10.3 | ↑ High |
| Total Protein | 6.28 g/dL | 6.6–8.3 | ↓ Low |
| Globulin | 2.15 g/dL | 2.3–3.5 | ↓ Low |
| A/G Ratio | 1.92 | 1.3–1.7 | ↑ High |
Probable Diagnosis
1. Iron Deficiency Anemia (Most Likely)
- Microcytic (low MCV 64.9), hypochromic (low MCH + MCHC) anemia
- Elevated RDW (15.4%) — indicates anisocytosis (variability in red cell size), a hallmark of iron deficiency
- High RBC count with low Hb — typical in iron deficiency where the bone marrow compensates
- Mentzer Index = 12.6 — a value >13 strongly favors iron deficiency (her value is borderline, leaning toward thalassemia territory, but the elevated RDW strongly points to iron deficiency)
The most likely underlying cause in a 46-year-old woman: chronic blood loss (heavy menstrual bleeding, GI bleed), poor dietary iron intake, or malabsorption.
2. Mild Thalassemia Trait (Cannot Be Excluded)
- Mentzer Index of 12.6 is borderline (just below 13), slightly leaning thalassemia
- Must be differentiated with serum ferritin, serum iron, TIBC, and Hb electrophoresis
3. Mild Thrombocytopenia with High MPV
- Platelet count 103,000 (low) + MPV 13.30 (very high) = platelets are large but few
- This pattern suggests increased platelet destruction or peripheral consumption (e.g., Immune Thrombocytopenic Purpura - ITP, viral illness, hypersplenism)
- Can also be seen alongside iron deficiency
4. Mild Hypoproteinemia (Low Total Protein + Low Globulin)
- May indicate nutritional deficiency, malabsorption, or early liver involvement
- Renal and liver function are otherwise normal (creatinine, urea, electrolytes are fine)
Recommended Investigations (Before Starting Treatment)
- Serum Ferritin (most sensitive for iron stores)
- Serum Iron + TIBC + Transferrin Saturation
- Hemoglobin Electrophoresis (to rule out thalassemia trait)
- Peripheral Blood Smear (to see red cell morphology)
- Stool for occult blood (to find source of iron loss)
- Gynecological evaluation (menorrhagia at 46 years is common)
- Anti-platelet antibodies / repeat platelet count (to assess thrombocytopenia cause)
Treatment Plan
For Iron Deficiency Anemia:
- Oral Iron: Ferrous sulfate 200mg (elemental iron ~65mg) 3 times daily OR Ferrous bisglycinate (better tolerated)
- Take on empty stomach with Vitamin C (lemon juice/orange juice) to enhance absorption
- Avoid tea, coffee, calcium supplements within 2 hours of iron tablet
- Treat the underlying cause (if menorrhagia → gynecology referral)
For Thrombocytopenia:
- Avoid NSAIDs (aspirin, ibuprofen)
- Further evaluation needed before treatment
- If ITP confirmed → may need steroids or specialist referral
For Low Protein:
- High-protein diet: eggs, lentils, legumes, paneer, fish
- Investigate for malabsorption if no dietary cause found
Expected Progress & Timeline
| Milestone | Timeframe |
|---|---|
| Reticulocyte rise (early bone marrow response) | 5–10 days after starting iron |
| Hemoglobin starts rising | 2–4 weeks |
| Hemoglobin reaches normal (12+ g/dL) | 2–3 months |
| Iron stores replenished (ferritin normalized) | 4–6 months (iron must be continued even after Hb normalizes) |
| Platelet count improvement | Depends on cause; re-check in 4–6 weeks |
Important Note
⚠️ This analysis is based solely on lab values. A physician must correlate these findings with clinical symptoms, physical examination, and additional investigations before making a final diagnosis and starting treatment. Do not self-medicate — please consult a physician or hematologist with these reports.
What about RFT test sacan in image given
RFT Results — Mrs. Hasumatiben Makwana (Female, 46Y)
| Parameter | Result | Reference Range | Status |
|---|---|---|---|
| Creatinine, Serum | 0.67 mg/dL | 0.5–1.1 | ✅ Normal |
| Urea | 20.9 mg/dL | 16.9–43.3 | ✅ Normal |
| Sodium (Na+) | 139.6 mmol/L | 136–145 | ✅ Normal |
| Potassium (K+) | 3.93 mmol/L | 3.5–5.1 | ✅ Normal |
| Uric Acid | 4.65 mg/dL | 2.3–6.1 | ✅ Normal |
| Total Protein | 6.28 g/dL | 6.6–8.3 | ⬇️ Low |
| Albumin | 4.13 g/dL | 3.5–5.3 | ✅ Normal |
| Globulin | 2.15 g/dL | 2.3–3.5 | ⬇️ Low |
| A/G Ratio | 1.92 | 1.3–1.7 | ⬆️ High |
Interpretation
✅ Kidney Function — NORMAL
- Creatinine 0.67 and Urea 20.9 confirm the kidneys are filtering well — no renal impairment
- Electrolytes (Sodium, Potassium) are balanced — no risk of fluid or acid-base disturbance
- Uric acid is normal — no gout risk currently
⚠️ Protein Panel — Mildly Abnormal
- Just slightly below the lower limit of 6.6
- Indicates the body has less circulating protein than needed
- Combined with iron deficiency anemia, this suggests overall nutritional deficiency
- Globulins include immune proteins (immunoglobulins) and transport proteins
- Low globulin can indicate:
- Poor protein intake / malnutrition
- Malabsorption (gut not absorbing nutrients properly)
- Reduced immune protein production (less common)
- Albumin is normal but globulin is low → this pushes the ratio above normal
- A high A/G ratio is less common but can be seen in hypogammaglobulinemia (low immune globulins) or simply reflects relatively low globulin against a normal albumin
What This Means Together
Nutritional deficiency — she is likely not getting enough dietary protein, which combined with iron deficiency, suggests a generalized poor nutritional state rather than any serious organ disease.
Recommendations for Low Protein
| Action | Details |
|---|---|
| Increase dietary protein | Eggs, dal, rajma, paneer, fish, chicken, soybean |
| Rule out malabsorption | If diet is adequate, investigate celiac disease or gut absorption issues |
| Repeat LFT (Liver Function Test) | To ensure the liver (which makes proteins) is functioning well |
| Repeat protein levels in 6–8 weeks | After dietary correction |
Bottom Line
⚠️ Always consult your treating physician before making any changes to diet or medications based on lab reports.
So what should be treatment given to patient
iron deficiency anemia treatment oral iron supplementation dose duration guidelines
thrombocytopenia treatment management mild low platelet count causes workup
Complete Treatment Plan for Mrs. Hasumatiben Makwana (46F)
🔴 Priority 1 — Iron Deficiency Anemia (Main Problem)
Medicines
| Medicine | Dose | When to Take | Duration |
|---|---|---|---|
| Ferrous Sulfate 200mg (or Ferrous Bisglycinate 100mg — better tolerated) | 1 tablet twice daily | Empty stomach, morning & evening | 4–6 months |
| Vitamin C 500mg | 1 tablet with each iron tablet | Same time as iron | Same duration |
| Folic Acid 5mg | 1 tablet once daily | With food | 3 months |
Why Vitamin C? It converts iron to absorbable form and doubles absorption.
Important Rules for Iron Tablets
- Take iron 1 hour before meals or 2 hours after meals
- Never take with tea, coffee, milk, antacids, or calcium supplements
- Stool may turn black — this is normal, not blood
- Common side effects: constipation, nausea — reduce dose if severe
🟡 Priority 2 — Thrombocytopenia (Low Platelets: 1,03,000)
Immediate Steps Required:
- Repeat platelet count after 2 weeks (to confirm it's not a lab error or temporary)
- Peripheral Blood Smear — to check platelet morphology
- Rule out causes:
- Dengue / viral fever (if recent fever history)
- ITP (Immune Thrombocytopenic Purpura) — most common in women
- Hypersplenism (enlarged spleen)
- Vitamin B12 / folate deficiency
Precautions Until Diagnosed:
- Avoid Aspirin, Ibuprofen, Diclofenac (all NSAIDs)
- Avoid alcohol completely
- Watch for signs of bleeding: unusual bruising, bleeding gums, heavy periods, red spots on skin (petechiae) → go to doctor immediately
- Platelets 1,03,000 is mild — not immediately dangerous (danger zone is below 20,000)
🟢 Priority 3 — Low Protein / Nutritional Deficiency
No medicine needed — Diet correction is the treatment
| Food Group | Daily Intake Recommended |
|---|---|
| Eggs | 2 eggs daily |
| Dal / Lentils | 2 bowls per day (moong, masoor, chana) |
| Paneer / Soya | 100g daily |
| Green leafy vegetables | Spinach, methi, drumstick leaves daily |
| Dry fruits | Dates, raisins, figs (also help with iron) |
| Milk / Curd | 1 glass milk + 1 bowl curd daily |
| Fish / Chicken (if non-veg) | 3–4 times per week |
🔵 Priority 4 — Investigate the Root Cause
| Investigation | Purpose |
|---|---|
| Serum Ferritin | Confirms iron store depletion |
| Serum Iron + TIBC | Confirms iron deficiency vs thalassemia |
| Hb Electrophoresis | Rules out thalassemia trait (Mentzer Index was borderline) |
| Stool Occult Blood Test | Rules out hidden GI bleeding |
| USG Abdomen | Check for spleen size (explain thrombocytopenia) |
| Gynecology consultation | Heavy periods (menorrhagia) is the #1 cause of iron deficiency in women |
| LFT (Liver Function Test) | Confirm liver is making proteins normally |
Follow-Up Schedule
| Timeframe | What to Check |
|---|---|
| 2 weeks | Repeat platelet count |
| 4 weeks | Hemoglobin level (should rise by 1–2 g/dL) |
| 3 months | Full CBC + Serum Ferritin |
| 6 months | Repeat CBC + RFT + Protein levels |
Summary in Simple Terms
Mrs. Hasumatiben primarily has iron deficiency anemia that needs iron + folic acid tablets for 4–6 months, a protein-rich diet, and investigation for why the iron is low (periods, gut bleed). Her kidneys are completely healthy. The low platelets need further investigation before any treatment is started — they are currently at a safe level but should be monitored closely.
⚠️ Disclaimer: This is for informational purposes only. All medicines must be prescribed by a qualified physician after clinical examination. Do not self-medicate.
What should be done as primary care for the person who hit tennis ball on testicle
testicular trauma blunt scrotal injury management primary care emergency
testicular rupture contusion diagnosis ultrasound scrotal trauma treatment
Immediate First Aid (First 0–30 Minutes)
Step 1 — Stop Activity Immediately
- Make the person sit or lie down in a comfortable position
- Bring knees gently toward chest — this reduces tension on the spermatic cord and eases pain
- Do NOT let them walk around — movement worsens pain and swelling
Step 2 — Support the Scrotum
- Place a folded cloth or soft towel underneath the scrotum to provide support and elevation
- This reduces blood pooling and swelling
- If athletic supporter/jockstrap is available, wear it gently
Step 3 — Apply Ice Pack
- Wrap ice cubes in a cloth (never apply ice directly to skin)
- Apply to the scrotal area for 15–20 minutes
- Repeat every hour for the first 4–6 hours
- This reduces swelling, bruising, and pain significantly
Step 4 — Pain Relief
- Give Ibuprofen 400mg or Paracetamol 500–1000mg orally
- Ibuprofen is preferred as it also reduces inflammation
- Do NOT give aspirin (increases bleeding risk)
Step 5 — Rest
- Complete bed rest for at least 24 hours
- Avoid any physical activity, sports, or lifting
🚨 Go to Emergency Immediately If ANY of These Signs Appear
| Warning Sign | What It May Mean |
|---|---|
| Severe, unbearable pain not improving | Testicular rupture or torsion |
| Rapidly increasing swelling | Internal bleeding / hematocele |
| Nausea and vomiting | Severe trauma or torsion |
| Bruising spreading rapidly | Significant vascular injury |
| Testicle feels very hard or misshapen | Possible rupture |
| No improvement after 1 hour | Needs urgent evaluation |
| Fever developing later | Risk of infection/abscess |
⚠️ Per Urological Trauma Guidelines (p. 30): Testicular rupture occurs in approximately 50% of direct blunt scrotal trauma cases. A tennis ball impact is generally below the force needed for rupture (~50 kg), but it must not be ignored.
What the Doctor Will Do
-
Scrotal Ultrasound with Colour Doppler — to check:
- Blood flow to testicle (rules out torsion)
- Internal bleeding (hematocele)
- Testicular contusion vs. rupture
- Integrity of tunica albuginea (outer covering of testicle)
-
If rupture confirmed → Emergency surgery within 72 hours (salvage rate is much higher with early surgery)
-
If only contusion/bruising → Conservative management with rest, ice, elevation, anti-inflammatories
What to Expect — Recovery Timeline
| Condition | Recovery Time |
|---|---|
| Mild contusion (bruising only) | 3–5 days with rest and ice |
| Moderate hematoma (blood collection) | 1–3 weeks |
| Testicular rupture (surgical repair) | 4–6 weeks |
| Pain and tenderness | May last up to 2 weeks even with mild injury |
DO's and DON'Ts
| ✅ DO | ❌ DON'T |
|---|---|
| Apply ice wrapped in cloth | Apply ice directly to skin |
| Elevate scrotum with soft support | Ignore worsening pain |
| Take paracetamol / ibuprofen | Take aspirin |
| Rest completely | Resume sports immediately |
| Seek medical help if pain worsens | Delay if swelling increases rapidly |
Bottom Line
⚠️ This information is for first-aid guidance only. Always consult a doctor for proper evaluation of any genital trauma.
In this cremesteric reflex help
What is the Cremasteric Reflex?
- It is a superficial reflex where stroking or lightly touching the inner thigh causes the cremaster muscle to contract, pulling the testicle upward toward the body
- It is present in normal healthy males
- Controlled by L1–L2 nerve roots (ilioinguinal and genitofemoral nerves)
Why It Matters After Testicular Trauma
✅ Cremasteric Reflex PRESENT
- Testicle rises when inner thigh is stroked
- This is a reassuring sign
- Suggests the testicle has intact blood supply and nerve function
- Makes testicular torsion very unlikely (though not 100% ruled out)
- Injury is likely just a contusion — manageable with first aid
🚨 Cremasteric Reflex ABSENT
- Testicle does NOT rise when inner thigh is stroked
- This is a red flag emergency sign
- Strongly suggests testicular torsion (twisting of spermatic cord cutting off blood supply)
- Torsion can occur after trauma due to impact causing the testicle to rotate
- Testicle can die within 4–6 hours if torsion is not treated surgically
How to Test It (Simple Bedside Check)
| Step | Action |
|---|---|
| 1 | Patient lies flat on his back |
| 2 | Use a blunt object or fingertip to lightly stroke the upper inner thigh (not the scrotum) |
| 3 | Observe whether the ipsilateral testicle rises upward |
| 4 | Repeat on the other side for comparison |
Normal response = testicle visibly lifts within 1–2 seconds
Cremasteric Reflex in Context of Tennis Ball Injury
| Scenario | Reflex Result | Action |
|---|---|---|
| Pain mild, swelling mild | Present | Ice, rest, pain relief — monitor at home |
| Pain severe, nausea present | Present | Still go to doctor for ultrasound |
| Any situation | Absent | 🚨 Rush to emergency immediately — possible torsion |
Important Limitations
- An absent reflex alone does not confirm torsion — some males normally have a weak or absent cremasteric reflex
- A present reflex does not fully rule out torsion — it is possible (rarely) to have torsion with reflex present
- Therefore cremasteric reflex is a quick screening tool, not a definitive test
- Colour Doppler Ultrasound remains the gold standard to confirm or rule out torsion
Bottom Line
After a testicular hit, check the cremasteric reflex first. If it is absent — do not wait, do not apply ice, do not give painkillers and observe — go straight to the emergency room. Time is the testicle. Surgical window for saving a torted testicle is 4–6 hours.
195 days not proper period and mild spotting
secondary amenorrhea 195 days missed period spotting perimenopause causes diagnosis
abnormal uterine bleeding spotting perimenopause 46 years workup investigations treatment
Understanding the Situation
| Fact | Detail |
|---|---|
| Age | 46 years |
| Duration without proper period | 195 days (~6.5 months) |
| Current symptom | Only mild spotting |
| Known findings | Iron deficiency anemia, low protein |
195 days of absent proper menstruation with only spotting in a 46-year-old woman is clinically significant and must be investigated urgently.
Most Likely Causes (Differential Diagnosis)
🥇 1. Perimenopause (Most Likely)
- Age 46 is the classic perimenopausal age (perimenopause occurs 2–8 years before menopause, typically ages 40–51)
- Periods become irregular, scanty, or absent with occasional spotting
- Estrogen levels fluctuate and gradually drop
- Spotting occurs due to unstable, thinning endometrium
- Per Harrison's (p. 11049): Irregular cycles for 1–2 years before the final menstrual period are normal in perimenopause
🥈 2. Pregnancy (Must Be Ruled Out First)
- Even at 46, pregnancy is possible
- Spotting can mimic periods
- Urine Pregnancy Test (UPT) must be done immediately before any other workup
🥉 3. Endometrial Hyperplasia / Polyp
- Prolonged low estrogen or hormonal imbalance → thickened irregular endometrium
- Can cause missed periods + spotting
- Risk increases with age — must be ruled out
⚠️ 4. Uterine Fibroid (Leiomyoma)
- Very common in women aged 40–50
- Can disrupt normal bleeding patterns
- Causes irregular spotting
⚠️ 5. Thyroid Dysfunction
- Hypothyroidism is a major cause of missed periods + spotting in women
- Also causes fatigue, weight gain, anemia — fits her profile
- Must be tested
🔴 6. Endometrial Carcinoma (Must Be Ruled Out)
- Any abnormal uterine bleeding in a woman >45 years must exclude endometrial cancer
- 195 days of no proper period followed by spotting is a warning sign
- Per Bailey & Love's Surgery (p. 1605): Postmenopausal or perimenopausal bleeding must be investigated structurally
Connection to Her Lab Reports
| Lab Finding | Connection to Period Problem |
|---|---|
| Hemoglobin 9.7 (low) | Could be FROM chronic blood loss due to abnormal uterine bleeding OR worsened by poor nutrition |
| Low protein + low globulin | Nutritional deficiency worsened by hormonal disruption |
| High RDW + microcytic anemia | Chronic iron loss from abnormal periods over months |
| Low platelets | May contribute to abnormal bleeding pattern |
Her iron deficiency anemia is very likely directly caused by this abnormal uterine bleeding pattern — this is the most probable root cause.
Investigations Required (Urgent)
| Investigation | Purpose | Priority |
|---|---|---|
| Urine Pregnancy Test | Rule out pregnancy | 🔴 Immediate |
| TSH (Thyroid) | Rule out hypothyroidism | 🔴 Urgent |
| FSH + LH + Estradiol | Confirm perimenopause | 🔴 Urgent |
| Transvaginal Ultrasound (TVS) | Check uterus, ovaries, endometrial thickness | 🔴 Urgent |
| Serum Ferritin + Iron studies | Confirm iron deficiency cause | 🟡 Soon |
| Prolactin level | Rule out pituitary cause of amenorrhea | 🟡 Soon |
| Endometrial biopsy | Rule out endometrial cancer if TVS shows thickened endometrium | 🟡 As directed by gynecologist |
| Pap smear | Cervical screening | 🟡 Routine |
Treatment (Depends on Diagnosis)
If Perimenopause Confirmed:
- Hormone Replacement Therapy (HRT) — low-dose estrogen + progesterone to regulate cycles and prevent osteoporosis
- Calcium + Vitamin D supplementation
- Lifestyle: regular exercise, stress reduction
If Thyroid Problem Found:
- Levothyroxine (thyroid hormone replacement) — periods often normalize within 3 months of treatment
If Fibroid/Polyp Found:
- Hormonal therapy or surgical removal depending on size
If Endometrial Hyperplasia:
- Progesterone therapy (Medroxyprogesterone) to protect the uterine lining
For Her Anemia (Already Identified):
- Continue iron + folic acid as discussed
- Anemia will not fully correct until the bleeding cause is treated
Timeline to Improvement
| Condition | Expected Improvement |
|---|---|
| Perimenopause regulated with HRT | 1–3 months |
| Thyroid treated | Periods resume in 2–3 months |
| Iron levels after treating cause | 3–4 months |
| Fibroid/polyp treated | Depends on procedure |
Most Important Next Step
🚨 Consult a Gynecologist immediately. 195 days without a proper period + spotting + iron deficiency anemia in a 46-year-old woman needs a Transvaginal Ultrasound and hormonal blood tests as the first priority. This cannot be managed with home remedies or diet alone.
⚠️ Do not ignore spotting assuming it is just "irregular periods" — at this age, all abnormal uterine bleeding must be properly investigated to rule out serious conditions including endometrial cancer.
195 days not proper period and mild spotting at age 21 year
secondary amenorrhea young woman 21 years causes diagnosis PCOS hypothalamic
secondary amenorrhea spotting workup investigations FSH LH prolactin thyroid treatment
Secondary Amenorrhea at 21 Years — Complete Analysis
What This Is Called
Most Likely Causes at Age 21
🥇 1. Pregnancy (Rule Out First — Always)
- Spotting can mimic periods
- Must be excluded before any other investigation
- Urine Pregnancy Test immediately
🥈 2. PCOS — Polycystic Ovary Syndrome (Most Common)
- #1 hormonal disorder in women aged 15–30
- Causes irregular or absent periods
- Associated with: acne, excess facial/body hair, weight gain, oily skin
- Elevated LH:FSH ratio, high androgens
- Spotting occurs due to unstable endometrium
🥉 3. Functional Hypothalamic Amenorrhea (FHA)
- Brain stops sending signals to ovaries due to stress, excessive exercise, or very low body weight/eating disorder
- Very common in young women
- Low estrogen, normal or low FSH/LH
- Ask about: dieting, weight loss, intense exercise, emotional stress, anxiety
⚠️ 4. Hyperprolactinemia
- Elevated prolactin (hormone from pituitary gland) suppresses ovulation
- Causes: pituitary adenoma (benign tumor), stress, certain medications
- Symptoms: milky discharge from nipples (galactorrhea), headache, vision changes
⚠️ 5. Thyroid Dysfunction
- Hypothyroidism (underactive thyroid) is a very common cause of missed periods in young women
- Symptoms: fatigue, weight gain, cold intolerance, dry skin, hair loss
⚠️ 6. Primary Ovarian Insufficiency (POI)
- Rare at 21 but possible — ovaries stop functioning prematurely
- High FSH, low estrogen
- Needs urgent treatment to protect bone density
⚠️ 7. Asherman's Syndrome
- Scarring inside uterus from previous D&C, abortion, or uterine procedure
- Causes absent or very scanty periods
- Ask about any previous uterine procedures
Key Questions to Ask the Patient
| Question | Why It Matters |
|---|---|
| Any recent significant weight loss? | Hypothalamic amenorrhea |
| Excessive exercise or athlete? | FHA |
| High stress / anxiety / depression? | FHA |
| Acne, facial hair, weight gain? | PCOS |
| Milky nipple discharge? | Hyperprolactinemia |
| Headaches or vision changes? | Pituitary tumor |
| Hot flashes, night sweats? | Premature ovarian insufficiency |
| Any previous uterine procedures? | Asherman's syndrome |
| Any medications (antipsychotics, antidepressants)? | Drug-induced amenorrhea |
Investigations Required
| Test | Purpose | Priority |
|---|---|---|
| Urine Pregnancy Test (UPT) | Rule out pregnancy | 🔴 First and immediate |
| FSH + LH | Distinguish PCOS vs hypothalamic vs ovarian failure | 🔴 Urgent |
| Estradiol (E2) | Assess estrogen level | 🔴 Urgent |
| Prolactin | Rule out hyperprolactinemia | 🔴 Urgent |
| TSH + Free T4 | Rule out thyroid dysfunction | 🔴 Urgent |
| Testosterone + DHEAS | Confirm PCOS / androgen excess | 🟡 Important |
| Progesterone challenge test | Checks if uterus responds — helps classify amenorrhea | 🟡 Important |
| Transvaginal / Pelvic Ultrasound | Check ovaries for cysts (PCOS), uterine lining thickness | 🟡 Important |
| AMH (Anti-Mullerian Hormone) | Assess ovarian reserve | 🟡 If POI suspected |
| MRI Brain (Pituitary) | Rule out pituitary adenoma | 🟠 If prolactin high |
Result Interpretation Guide
| FSH/LH | Estrogen | Likely Diagnosis |
|---|---|---|
| Low/Normal | Low | FHA (hypothalamic — stress/weight/exercise) |
| High LH:FSH ratio | Normal/High | PCOS |
| High FSH | Low | Premature Ovarian Insufficiency |
| Normal | Normal | Outflow tract problem / Asherman's |
| Normal | Normal + High Prolactin | Hyperprolactinemia |
Treatment (Based on Cause)
If PCOS:
- Combined Oral Contraceptive Pill (OCP) — regulates periods, reduces androgens
- Metformin — if insulin resistance present
- Lifestyle: weight management, low glycemic diet, regular moderate exercise
- Period regulation expected in 1–3 months
If FHA (Stress/Weight/Exercise):
- Address the root cause — reduce exercise, gain weight, manage stress
- Cognitive Behavioral Therapy (CBT) if eating disorder involved
- Hormonal support if estrogen very low (to protect bones)
- Periods return in 3–6 months after weight restoration or stress reduction
If Hypothyroidism:
- Levothyroxine daily
- Periods normalize in 2–3 months after thyroid correction
If Hyperprolactinemia:
- Cabergoline or Bromocriptine (dopamine agonists)
- Lowers prolactin, restores ovulation
- Periods return in 1–3 months
If Premature Ovarian Insufficiency:
- Hormone Replacement Therapy (HRT) — essential to protect bones, heart, and brain
- Fertility specialist referral
- Psychological support
Why the Spotting is Happening
- Estrogen builds up the uterine lining slightly but without ovulation
- The unstable, thin endometrium sheds a little
- This is not a real period — it is just the lining breaking down irregularly
Urgency & Timeline
| Action | Timeframe |
|---|---|
| Pregnancy test | Today |
| Blood tests (FSH, LH, prolactin, TSH, estradiol) | This week |
| Pelvic ultrasound | This week |
| Gynecologist consultation | Within 1 week |
| Treatment response | 1–3 months depending on diagnosis |
Bottom Line
A 21-year-old with 195 days of absent periods and only spotting most likely has PCOS or Functional Hypothalamic Amenorrhea — both very treatable. However, pregnancy must be ruled out today, and a full hormonal blood panel + pelvic ultrasound is essential this week. Early diagnosis and treatment protects her fertility, bone density, and long-term hormonal health.
⚠️ Please consult a gynecologist or endocrinologist urgently. Do not self-medicate with hormonal pills without proper diagnosis.
Tablet?!
⚠️ Why You Cannot Give a Tablet Without Tests
| If You Give... | Without Knowing... | Risk |
|---|---|---|
| OCP (birth control pill) | Pregnancy status | Dangerous in early pregnancy |
| Progesterone tablet | Prolactin/thyroid status | May mask serious condition |
| Any hormonal pill | FSH/LH levels | Can worsen hormonal imbalance |
The Only Safe First Step Right Now
🔴 Step 1 — Urine Pregnancy Test (UPT)
- Available at any pharmacy for ₹30–50
- Do it first morning urine for most accurate result
- Must be done before anything else
After Pregnancy is Ruled Out — Then Doctor May Prescribe:
Most Commonly Used Tablets for Amenorrhea:
| Situation | Tablet | Dose |
|---|---|---|
| To induce withdrawal bleed (diagnostic) | Medroxyprogesterone (Meprate/Provera) | 10mg daily × 10 days |
| PCOS confirmed | Combined OCP (Yasmin / Diane-35) | 1 tablet daily × 21 days |
| PCOS + insulin resistance | Metformin 500mg | Twice daily with food |
| Hypothyroidism confirmed | Levothyroxine (Thyronorm) | As per TSH level |
| High prolactin confirmed | Cabergoline 0.25mg | Twice weekly |
Most Practical Immediate Advice
- Do pregnancy test today
- If negative → visit gynecologist this week with the test result
- Doctor will likely give Medroxyprogesterone (Meprate) 10mg for 10 days as first step to induce a period and assess uterine response
- Do not take any hormonal tablet on your own
⚠️ Hormonal medications are not over-the-counter safe decisions. Wrong hormonal treatment can disrupt the cycle further, cause abnormal bleeding, or delay diagnosis of a serious condition. Please see a gynecologist before starting any tablet.
A person hit by tennis ball on cricket ground after which he has mild swelling on face and water coming from eye with the blurry vision and he also complain of the headache
blunt facial trauma orbital injury blurred vision periorbital swelling management
orbital blowout fracture epiphora watering eye headache blunt trauma diagnosis treatment
traumatic brain injury headache after head trauma concussion assessment red flags
orbital blowout fracture facial trauma CT scan periorbital swelling
🚨 Symptom Analysis
| Symptom | What It Suggests |
|---|---|
| Mild facial swelling | Soft tissue contusion / facial bone injury |
| Watering eye (Epiphora) | Nasolacrimal duct injury OR conjunctival irritation from trauma |
| Blurry vision | Orbital injury, optic nerve trauma, hyphema, or concussion |
| Headache | Concussion / traumatic brain injury (TBI) — most concerning |
Most Likely Diagnoses
🥇 1. Orbital Blowout Fracture (High Suspicion)
"The floor of the orbit is its weakest wall and in blunt trauma, such as a blow from a fist, it is often fractured without fractures of the other walls."
- Swelling and bruising around the eye ✅ (present)
- Watering eye ✅ (present)
- Blurred vision ✅ (present)
- Double vision (diplopia) — especially on looking upward (inferior rectus entrapment)
- Numbness of cheek (infraorbital nerve injury)
- Eye appearing sunken (enophthalmos)

🥈 2. Concussion / Mild Traumatic Brain Injury
"Direct orbital injury may cause short-lived blurred vision... Partial optic nerve injuries from closed trauma result in blurring of vision."
- Headache ✅ (present)
- Blurry vision ✅ (present)
- Confusion, disorientation
- Memory loss of the event
- Nausea/vomiting
- Dizziness
🥉 3. Hyphema (Blood in Front of Eye)
- Blunt trauma can rupture blood vessels inside the eye
- Blood collects in the anterior chamber (between cornea and iris)
- Causes blurry vision + pain
- Visible as a red layer at the bottom of the iris
- Needs urgent ophthalmology evaluation
⚠️ 4. Nasolacrimal Duct Injury
- The duct that drains tears gets disrupted
- Causes constant watering of the eye (epiphora) even without crying
- Requires ENT/ophthalmology repair
🚨 RED FLAG Signs — Rush to Emergency Immediately
| Sign | Emergency |
|---|---|
| Vomiting after headache | Raised intracranial pressure |
| Confusion / not recognizing people | Serious TBI / intracranial bleed |
| Unequal pupils | Brain herniation — life threatening |
| Vision completely lost | Optic nerve / retinal damage |
| Cannot move eye upward | Muscle entrapment in blowout fracture |
| Seizure | Intracranial injury |
| Worsening headache over hours | Extradural/subdural hematoma |
| Clear fluid from nose | CSF rhinorrhea — skull base fracture |
Immediate First Aid at Ground
Step 1 — Do NOT do these:
- ❌ Do NOT press or rub the eye
- ❌ Do NOT apply ice directly on the eyeball
- ❌ Do NOT give NSAIDs (ibuprofen) if eye injury suspected — increases bleeding risk
- ❌ Do NOT let the person blow their nose (can push air into orbit worsening fracture)
Step 2 — Do these:
- ✅ Make the person sit upright (reduces eye pressure)
- ✅ Cover the eye loosely with a clean cloth — do NOT patch tightly
- ✅ Give Paracetamol only for headache (not ibuprofen/aspirin)
- ✅ Apply cold compress gently on the facial swelling (not directly on eyeball)
- ✅ Keep the person calm and still
- ✅ Check for pupil equality — both pupils should be same size
Step 3 — Transport Immediately
- Do not drive himself — blurry vision is present
- Take to hospital with Ophthalmology + Emergency department
Investigations Needed at Hospital
| Investigation | Purpose |
|---|---|
| CT Face + Orbit (non-contrast) | Gold standard — detect orbital fracture, facial bone injury |
| CT Brain | Rule out intracranial bleed / concussion |
| Slit lamp examination | Check hyphema, corneal injury, lens damage |
| Visual acuity test | Quantify vision loss |
| Intraocular pressure | Rule out traumatic glaucoma |
| Colour Doppler of orbit | Assess blood supply to optic nerve |
Treatment (Hospital)
| Finding | Treatment |
|---|---|
| Concussion | Rest, observation 24–48 hrs, paracetamol, no screen time |
| Orbital blowout fracture | Surgery within 2 weeks if muscle entrapment or significant defect |
| Hyphema | Eye rest, head elevation, cycloplegic drops, avoid NSAIDs |
| Nasolacrimal injury | Surgical repair by ophthalmologist |
| Optic nerve injury | High-dose steroids, urgent ophthalmology |
| Intracranial bleed | Neurosurgery emergency |
Recovery Timeline
| Injury | Recovery |
|---|---|
| Mild concussion | 1–2 weeks with rest |
| Orbital soft tissue swelling | 5–7 days |
| Blowout fracture (non-surgical) | 4–6 weeks |
| Blowout fracture (surgical repair) | 6–8 weeks |
| Hyphema (mild) | 5–7 days |
| Vision recovery (if optic nerve involved) | Weeks to months — variable |
Bottom Line
This patient has a potentially serious eye and head injury. The combination of blurry vision + watering eye + facial swelling + headache after a direct ball impact strongly suggests an orbital blowout fracture with possible concussion. He needs emergency CT scan of face and brain + urgent ophthalmology evaluation today. Do not delay — vision loss and intracranial bleeding are time-sensitive emergencies.
⚠️ Do not manage this at home. Take to hospital immediately.
Why there is pain on occipital region when ball hit right eye
occipital pain referred pain eye trauma optic nerve visual cortex anatomy pathway
visual pathway optic nerve optic chiasm visual cortex occipital lobe anatomy diagram
Why Occipital Pain Occurs When the Eye is Hit
The Visual Pathway — The Key to Understanding This
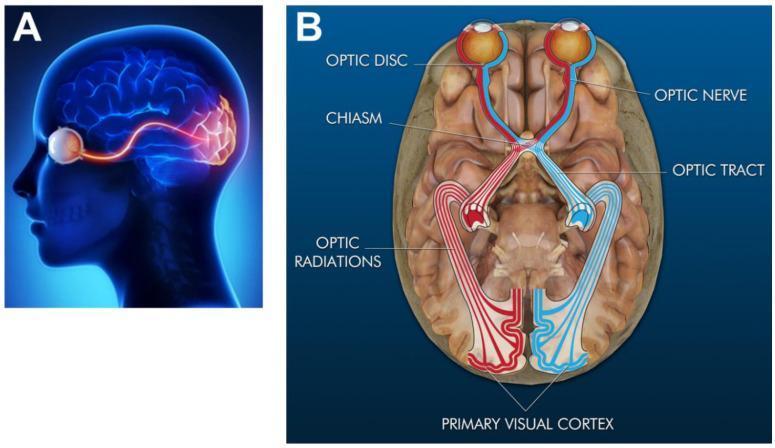
Step-by-Step Explanation
Tennis Ball Hits Right Eye
↓
Mechanical force transmitted to
Optic Nerve (Cranial Nerve II)
↓
Impulse travels along optic nerve
→ Optic Chiasm (below brain)
→ Optic Tract
→ Lateral Geniculate Nucleus (thalamus)
→ Optic Radiations
↓
PRIMARY VISUAL CORTEX
(located in OCCIPITAL LOBE
— at the BACK of the skull)
↓
Sudden abnormal electrical impulse
causes OCCIPITAL HEADACHE / PAIN
4 Reasons for Occipital Pain After Eye Trauma
1. 🧠 Visual Cortex Irritation (Main Reason)
- The primary visual cortex sits in the occipital lobe at the very back of the brain
- When the eye is hit, a sudden massive nerve impulse travels the entire visual pathway and abnormally stimulates the occipital cortex
- This causes pain felt at the back of the head (occipital region)
- Same mechanism as why pressing on your eye in the dark produces flashes of light (phosphenes) — mechanical pressure activates the visual pathway
2. 👁️ Optic Nerve Stretch / Shock
- The optic nerve runs from the eye through the optic canal in the skull to the brain
- A direct blow causes sudden traction and vibration of the optic nerve
- Pain is referred backward along the nerve pathway to the occipital area
- Similar to how hitting your elbow (ulnar nerve) causes pain shooting to the fingers
3. 🔄 Referred Pain Mechanism
- The trigeminal nerve (CN V) supplies pain sensation to the eye and surrounding structures
- Its connections within the brainstem converge with cervical nerve pathways
- This convergence creates referred pain felt at the back of the head
- Same concept as heart attack pain felt in the left arm
4. 💥 Contrecoup-Like Mechanism
- Similar to brain injury physics — force hits the front (eye/orbit)
- Pressure wave travels through cerebrospinal fluid (CSF)
- Causes contrecoup irritation at the opposite posterior brain (occipital region)
Summary Table
| Mechanism | Pathway | Result |
|---|---|---|
| Visual cortex stimulation | Eye → Optic nerve → Occipital cortex | Occipital pain + light flashes |
| Optic nerve traction | Direct nerve stretch | Referred pain posteriorly |
| Trigeminal-cervical convergence | CN V → brainstem → C2/C3 | Referred occipital headache |
| Pressure wave transmission | CSF pressure wave anteroposterior | Contrecoup-type occipital pain |
Clinical Significance — When to Worry
| Occipital Pain Type | What It May Mean |
|---|---|
| Mild, resolves in minutes | Normal visual pathway stimulation — benign |
| Persists for hours | Concussion / optic nerve injury |
| Worsening over time | 🚨 Intracranial bleed (extradural/subdural hematoma) |
| With neck stiffness | 🚨 Subarachnoid hemorrhage |
| With vision loss | 🚨 Optic nerve damage / posterior cortex injury |
| With vomiting + confusion | 🚨 Raised intracranial pressure — EMERGENCY |
Simple Analogy to Explain This
Think of the visual pathway like an electrical wire running from a socket (eye) to a bulb (occipital cortex). When you hit the socket hard, the electrical surge travels the entire wire and causes the bulb at the other end to flicker and overheat — that is exactly what causes occipital pain when the eye is struck.
⚠️ Occipital pain after eye trauma is expected and usually benign, but persistent or worsening occipital pain must be evaluated with a CT brain to rule out intracranial injury.
What is the best drug for morning sickness and vomiting in early pregnancy
Nausea & Vomiting in Early Pregnancy — Best Treatments
Important note: "Morning sickness" is a misnomer — per Yamada's Gastroenterology (p. 815): it persists throughout the day and occurs only in the morning in less than 2% of women.
Step-by-Step Treatment Ladder
🟢 STEP 1 — Non-Drug Treatment First (Mild Cases)
| Remedy | How to Use |
|---|---|
| Ginger | Ginger tea, ginger biscuits, ginger capsules 250mg 4x/day — proven effective in RCTs |
| Small, frequent meals | Eat every 2 hours — empty stomach worsens nausea |
| Avoid triggers | Strong smells, fatty/spicy food, heat |
| Cold foods | Less smell than hot food — better tolerated |
| Acupressure | P6 (wrist) pressure band — evidence-based non-drug option |
| Adequate rest | Fatigue worsens nausea significantly |
🟡 STEP 2 — First-Line Drug (Safest, Start Here)
Pyridoxine (Vitamin B6) — SAFEST FIRST CHOICE
| Detail | Info |
|---|---|
| Dose | 10–25mg 3 times daily |
| Safety | No known risk of fetal harm — safest option |
| Effectiveness | Proven better than placebo in multiple studies |
| Available as | Vitamin B6 tablets (widely available, OTC) |
Doxylamine + Pyridoxine (Combination) — GOLD STANDARD
| Detail | Info |
|---|---|
| Brand names | Diclegis, Bonjesta, Unisom + B6 |
| Dose | Doxylamine 10mg + Pyridoxine 10mg — 1–2 tablets at bedtime |
| Safety | FDA-approved for nausea/vomiting of pregnancy |
| How it works | Antihistamine (doxylamine) + B6 together reduce vomiting center stimulation |
⚠️ Women using this combination should not breastfeed (risk of infant CNS depression)
🟠 STEP 3 — If Step 2 Fails (Moderate Cases)
Metoclopramide (Perinorm/Reglan) — PREFERRED IV/ORAL AGENT
| Detail | Info |
|---|---|
| Dose | 10mg 3 times daily oral / IV |
| Safety | Study of 81,703 births showed no increased risk of congenital malformations — Yamada's (p. 815) |
| Best for | When patient cannot tolerate oral medications |
| Side effects | Drowsiness, restlessness, dystonia |
| Caution | Avoid prolonged use — FDA black box warning for tardive dyskinesia with chronic use |
Antihistamines — Dimenhydrinate / Diphenhydramine (Avomine / Benadryl)
| Detail | Info |
|---|---|
| Dose | Dimenhydrinate 50mg every 4–6 hours |
| Safety | Safe to use in pregnancy — no teratogenic risk |
| Caution | Avoid close to delivery — may cause respiratory depression in newborn |
Prochlorperazine (Stemetil)
| Detail | Info |
|---|---|
| Dose | 5–10mg 3 times daily |
| Safety | Low teratogenic risk in human studies |
| Caution | Risk of extrapyramidal symptoms in newborn if used in third trimester |
🔴 STEP 4 — Severe Cases / Hyperemesis Gravidarum
Ondansetron (Zofran) — VERY EFFECTIVE BUT USE WITH CAUTION
| Detail | Info |
|---|---|
| Dose | 4–8mg every 8 hours oral or IV |
| Effectiveness | One of the most commonly prescribed antiemetics — as effective as promethazine |
| Safety concern | Sensitivity analyses show possible risk of cardiac anomalies and cleft palate — conflicting studies |
| Recommendation | Avoid in first trimester if possible — use only when other agents fail |
| If used | Fully discuss risks/benefits with patient |
Methylprednisolone (IV Steroids) — LAST RESORT
| Detail | Info |
|---|---|
| Dose | 16mg every 8 hours IV × 3 days (hospitalized) |
| When to use | Only for severe hyperemesis gravidarum not responding to all other agents |
| Caution | Avoid before 10 weeks of gestation — ACOG guideline |
| Benefit | Proven to decrease hospital readmission |
Complete Drug Summary Table
| Drug | Safety in Pregnancy | Trimester | Use |
|---|---|---|---|
| Vitamin B6 (Pyridoxine) | ✅ Safest | All | First line |
| Doxylamine + B6 | ✅ FDA approved | All | First line |
| Ginger | ✅ Safe | All | Non-drug first |
| Metoclopramide | ✅ Safe | All | Second line |
| Dimenhydrinate | ✅ Safe | 1st/2nd | Second line |
| Prochlorperazine | ⚠️ Caution 3rd trimester | 1st/2nd | Second line |
| Ondansetron | ⚠️ Avoid 1st trimester if possible | 2nd/3rd | Third line |
| Methylprednisolone | ⚠️ Avoid before 10 weeks | After 10 wks | Last resort |
| Thalidomide | 🚫 ABSOLUTELY CONTRAINDICATED | Never | Never use |
⚠️ Drugs to NEVER Give in Pregnancy for Vomiting
| Drug | Risk |
|---|---|
| Thalidomide | Severe limb deformities (phocomelia) |
| Aspirin | Bleeding, fetal harm |
| Domperidone | Limited safety data |
When to Hospitalize (Hyperemesis Gravidarum)
- Cannot keep any food or fluid down for >24 hours
- Signs of dehydration (dry mouth, dark urine, dizziness)
- Weight loss >5% of body weight
- Electrolyte imbalance (needs IV fluids + IV antiemetics)
- Ketonuria on urine dipstick
Bottom Line
Best and safest drug: Pyridoxine (Vitamin B6) 25mg 3 times daily — start here. Best combination: Doxylamine 10mg + Pyridoxine 10mg at bedtime — FDA approved, most evidence-based. If vomiting is severe: Metoclopramide (oral or IV) is preferred with the best safety profile. Ondansetron is effective but should be avoided in the first trimester if possible.
⚠️ All medications in pregnancy must be prescribed by an obstetrician or qualified physician. Never self-medicate during pregnancy.
And wchich drug use to increase bp
Drugs Used to Increase Blood Pressure
First, it is important to know why the BP is low — because the choice of drug depends entirely on the cause of hypotension.
Before Giving Any Drug — Do This First
"Placing the patient in the recumbent position and ensuring adequate fluid volume while the primary problem is determined and treated is usually the correct course of action."
| First Step | Action |
|---|---|
| Lay patient flat | Legs elevated (Trendelenburg position) |
| IV Fluids | Normal saline or Ringer's lactate bolus first |
| Find the cause | Bleeding? Infection? Heart failure? Dehydration? |
Main Vasopressor Drugs
🥇 1. Norepinephrine (Levophed) — FIRST LINE FOR MOST CASES
| Detail | Info |
|---|---|
| Mechanism | Powerful α1 + β1 agonist → vasoconstriction + mild cardiac stimulation |
| Dose | 1–20 mcg/min IV infusion |
| Effect | Increases BP strongly, minimal heart rate change |
| Best for | Septic shock, vasodilatory shock — first-line choice |
| Why preferred | Best balance — raises BP without causing dangerous arrhythmias |
🥈 2. Epinephrine (Adrenaline)
| Detail | Info |
|---|---|
| Mechanism | α1 + β1 + β2 agonist → vasoconstriction + strong cardiac stimulation |
| Dose | 0.1–1 mcg/kg/min IV / 1mg IV bolus in cardiac arrest |
| Effect | Raises BP + increases heart rate + increases cardiac output |
| Best for | Anaphylactic shock (drug of choice), cardiac arrest, when norepinephrine fails |
| Caution | Can cause arrhythmias, increases myocardial oxygen demand |
🥉 3. Dopamine
| Detail | Info |
|---|---|
| Mechanism | Dose-dependent: low dose = renal vasodilation; high dose = α + β effects |
| Dose | 5–20 mcg/kg/min IV |
| Low dose (1–4 mcg/kg/min) | Dopaminergic — renal perfusion (controversial benefit) |
| High dose (>10 mcg/kg/min) | Vasoconstriction — raises BP |
| Caution | Higher arrhythmia risk than norepinephrine — not preferred over norepinephrine |
| Still useful for | Hypotension with bradycardia |
4. Vasopressin (ADH)
| Detail | Info |
|---|---|
| Mechanism | V1 receptor → direct vasoconstriction (non-adrenergic) |
| Dose | 0.04 units/min IV |
| Best for | Septic shock — add-on to norepinephrine to reduce norepinephrine dose |
| Advantage | Does not cause tachycardia |
| Use | Post-cardiopulmonary bypass shock |
5. Phenylephrine
| Detail | Info |
|---|---|
| Mechanism | Pure α1 agonist — only vasoconstriction, no cardiac stimulation |
| Dose | 20–200 mcg/min IV |
| Best for | Hypotension due to spinal anesthesia, supraventricular tachycardia with low BP |
| Advantage | Does not increase heart rate — safe when tachycardia is already present |
| Caution | Can decrease cardiac output — avoid in cardiogenic shock |
6. Dobutamine
| Detail | Info |
|---|---|
| Mechanism | Primarily β1 agonist — increases cardiac contractility and output |
| Dose | 2–20 mcg/kg/min IV |
| Best for | Cardiogenic shock — when heart is weak and not pumping enough |
| Note | Does NOT directly raise BP through vasoconstriction — raises BP by improving cardiac output |
| Often combined with | Norepinephrine in cardiogenic shock |
7. Midodrine (For Chronic/Oral Use)
| Detail | Info |
|---|---|
| Mechanism | Oral α1 agonist |
| Dose | 2.5–10mg 3 times daily orally |
| Best for | Chronic orthostatic hypotension (dizziness on standing) |
| Advantage | Only oral vasopressor available |
8. Fludrocortisone (For Chronic Low BP)
| Detail | Info |
|---|---|
| Mechanism | Mineralocorticoid → retains salt and water → increases blood volume |
| Dose | 0.1–0.2mg once daily oral |
| Best for | Chronic low BP, orthostatic hypotension, Addison's disease |
| Often combined with | Midodrine |
Vasopressor Comparison Table
| Drug | Vasoconstriction | Heart Rate | Cardiac Output | Best Use |
|---|---|---|---|---|
| Norepinephrine | 4+ | Mild ↑ | Maintained | Septic/vasodilatory shock — first line |
| Epinephrine | 3+ | ↑↑ | ↑↑ | Anaphylaxis, cardiac arrest |
| Dopamine | 2–3+ | ↑↑ | ↑ | Bradycardia + hypotension |
| Vasopressin | 3–4+ | No change | Maintained | Add-on in septic shock |
| Phenylephrine | 4+ | No change | ↓ slight | Spinal anesthesia hypotension |
| Dobutamine | 0 | ↑ | ↑↑ | Cardiogenic shock |
| Midodrine | 2+ | No change | No change | Chronic orthostatic hypotension (oral) |
Which Drug for Which Condition
| Condition | Drug of Choice |
|---|---|
| Septic shock | Norepinephrine (first) + Vasopressin (add-on) |
| Anaphylactic shock | Epinephrine IM 0.5mg (adrenaline — absolute first choice) |
| Cardiogenic shock | Norepinephrine + Dobutamine |
| Hypovolemic shock | IV Fluids first → then Norepinephrine if needed |
| Spinal anesthesia hypotension | Phenylephrine or Ephedrine |
| Cardiac arrest | Epinephrine 1mg IV every 3–5 min |
| Chronic orthostatic hypotension | Midodrine + Fludrocortisone (oral) |
| Bradycardia + low BP | Dopamine or Epinephrine |
Simple Summary
🔴 Emergency (hospital) low BP → Norepinephrine IV is the first choice for most shock states 🟡 Anaphylaxis → Epinephrine (Adrenaline) injection immediately 🟢 Chronic / mild low BP → Midodrine oral + fluids + salt intake + Fludrocortisone
⚠️ All vasopressor drugs are hospital/ICU-level medications administered under strict monitoring (IV lines, BP monitoring, cardiac monitoring). They must never be self-administered. Consult a physician or emergency specialist for any case of significantly low blood pressure.