Now I have comprehensive information from multiple authoritative textbooks and excellent diagrams. Let me compile a thorough set of notes.
Development of the Tongue - Complete Notes
Overview
The tongue develops from the floor of the primitive pharynx (stomodeum) during the 4th week of intrauterine life (IUL), arising from contributions of the 1st, 2nd, 3rd, and 4th pharyngeal arches. Its development involves a series of swellings that proliferate, overgrow, and fuse in a precise sequence.
Developmental Swellings - Step by Step
Step 1: Tuberculum Impar (Median Lingual Swelling)
- Appears at the end of the 4th week of IUL
- A small, median, triangular elevation in the floor of the primitive pharynx
- Located just cranial (rostral) to the foramen cecum
- Derived from 1st pharyngeal arch mesenchyme
- Also called the median tongue bud - it is the first indication of tongue development
- Fate: It is ultimately overgrown by the lateral lingual swellings and does not form a recognizable part of the adult tongue
Step 2: Lateral Lingual Swellings (Distal Tongue Buds)
- Appear soon after the tuberculum impar
- Two oval swellings, one on each side of the tuberculum impar
- Placed slightly distal to the tuberculum impar - hence called distal tongue buds
- Derived from proliferation of mesenchyme in the ventromedial parts of the 1st pharyngeal arch
- They rapidly increase in size, merge with each other, and overgrow the tuberculum impar
Fate of lateral lingual swellings:
- They merge and form the anterior 2/3 (oral part / body) of the tongue
- The midline groove on the tongue surface + the internal fibrous lingual septum mark the fusion site of the two lateral swellings
Step 3: Hypobranchial Eminence / Copula of His
- Develops caudal to the tuberculum impar
- A large, second median swelling in the floor of the primitive pharynx
- Derived from mesoderm of the 2nd, 3rd, and part of the 4th pharyngeal arches
- It soon subdivides into two parts:
- Large cranial part = the true hypobranchial eminence (from 3rd and 4th arch mesenchyme)
- Small caudal part = the copula (from 2nd arch fusion) - this is eventually overgrown and disappears
Note on terminology: Some texts use "hypobranchial eminence" and "copula" interchangeably for the whole structure (copula of His), while others distinguish the 2nd arch copula from the 3rd/4th arch hypobranchial eminence. The key point: the 2nd arch component (copula) is overgrown by the 3rd arch tissue - explaining why sensory supply to the posterior tongue is from CN IX (glossopharyngeal - 3rd arch nerve) rather than CN VII.
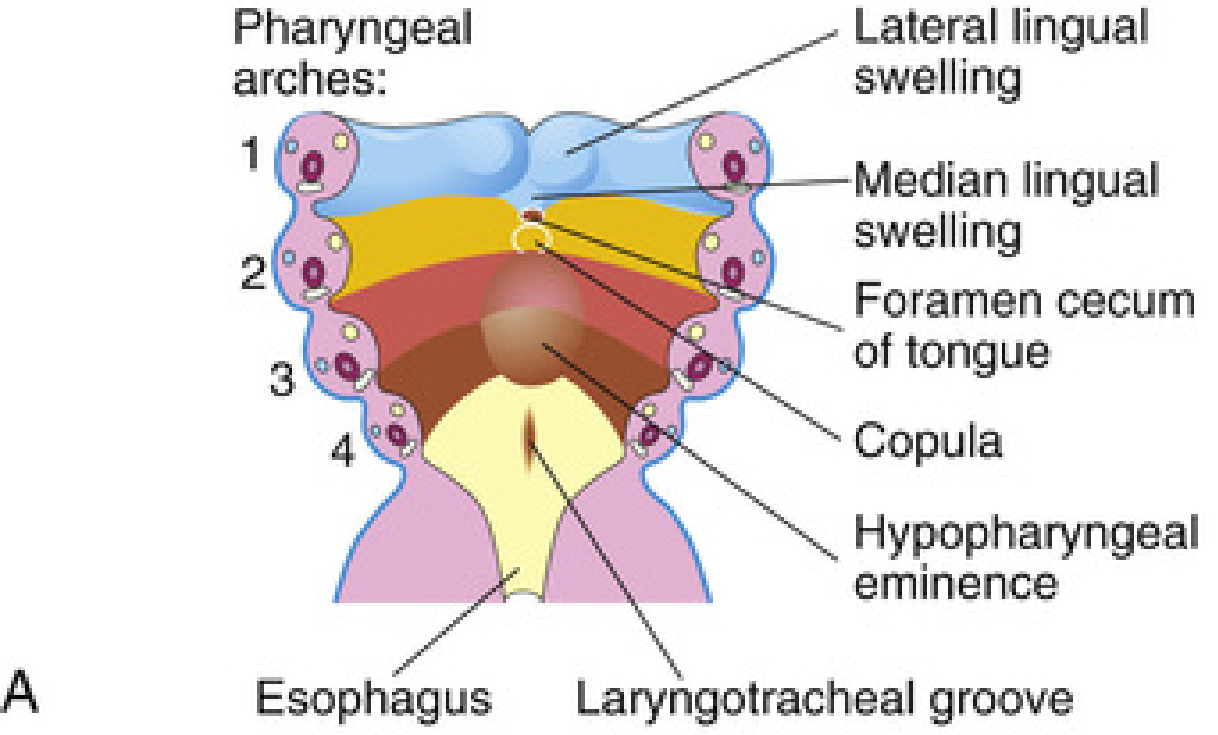
The floor of the primitive pharynx showing pharyngeal arches 1-4, with the lateral lingual swellings (blue, arch 1), median lingual swelling/tuberculum impar, foramen cecum, copula/hypobranchial eminence (arches 2-4), and the laryngotracheal groove caudally.
Step 4: Epiglottal Swelling
- A third median swelling formed by the posterior part of the 4th arch
- Marks development of the epiglottis
- The laryngeal orifice lies immediately behind this swelling, flanked by the arytenoid swellings
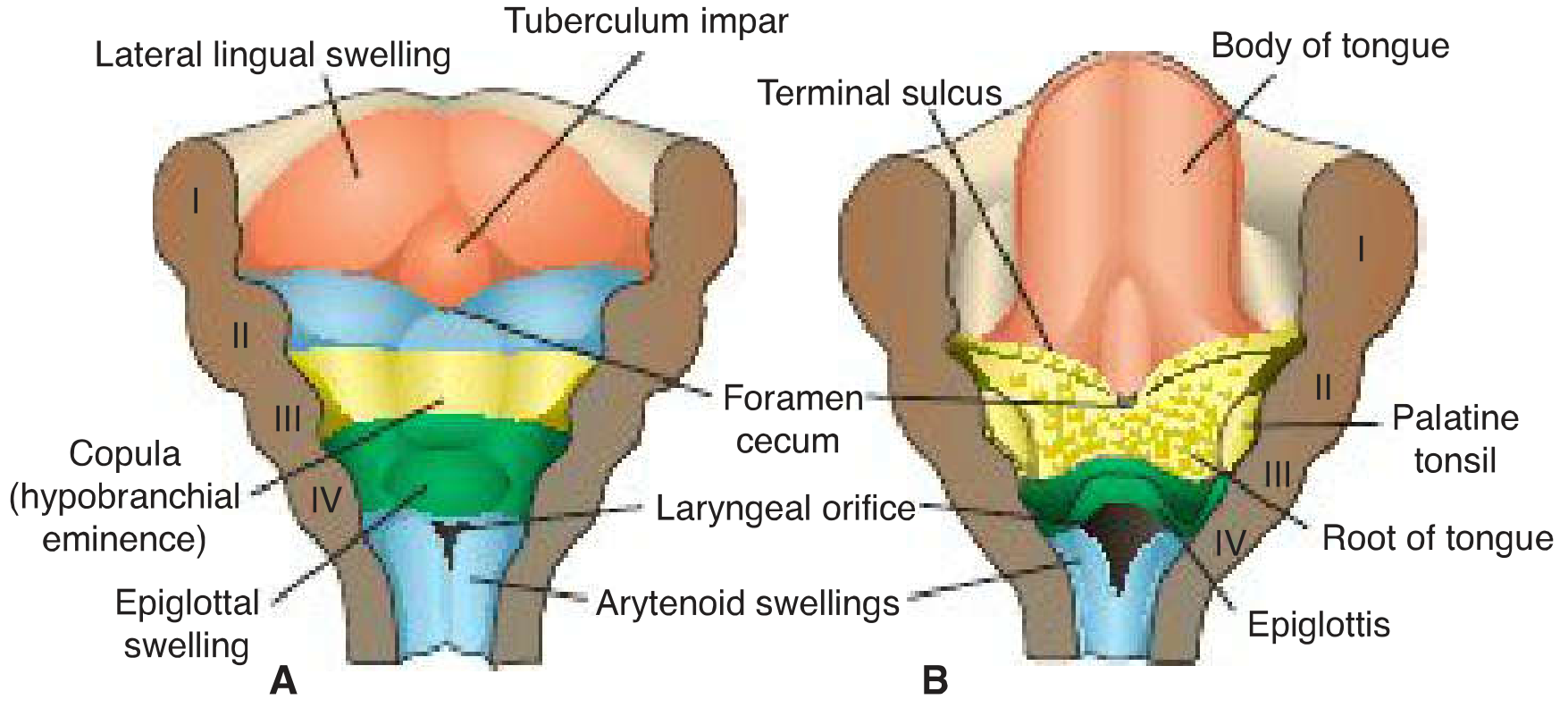
Summary Diagram of Derivatives
Left panel (early): tuberculum impar, lateral lingual swellings, copula (hypobranchial eminence), epiglottal swelling. Right panel (later): body of tongue, terminal sulcus, foramen cecum, root of tongue, palatine tonsil, epiglottis.
Adult Tongue: What Each Swelling Becomes
| Embryonic Swelling | Pharyngeal Arch | Adult Structure |
|---|
| Lateral lingual swellings + tuberculum impar | 1st arch | Anterior 2/3 (body/oral part) |
| Copula (2nd arch part) | 2nd arch | Overgrown - no recognizable derivative |
| Hypobranchial eminence (cranial part) | 3rd + 4th arch | Posterior 1/3 (root/pharyngeal part) |
| Epiglottal swelling | 4th arch | Epiglottis + extreme posterior tongue |
Nerve Supply - Explained by Development
Because the nerve supply follows the arch of origin, the tongue's innervation is a direct map of its embryology:
| Region | Sensory (General) | Sensory (Taste/Special) | Arch |
|---|
| Anterior 2/3 | CN V3 (lingual branch of mandibular) | CN VII (chorda tympani) | 1st arch |
| Posterior 1/3 | CN IX (glossopharyngeal) | CN IX | 3rd arch |
| Extreme posterior + epiglottis | CN X (superior laryngeal branch of vagus) | CN X | 4th arch |
Key fact: CN IX supplies the posterior 1/3 (not CN VII) because 3rd arch tissue overgrows 2nd arch tissue - the 2nd arch (CN VII territory) contribution disappears.
Muscle Development
- Most tongue muscles are derived from myoblasts migrating from occipital somites (2nd to 5th occipital myotomes) - NOT from pharyngeal arch mesenchyme
- The hypoglossal nerve (CN XII) accompanies these myoblasts during migration and innervates all intrinsic + most extrinsic tongue muscles
- Palatoglossus is the exception - innervated by CN X (vagus) via the pharyngeal plexus, reflecting its palatal origin
- Some muscles may also differentiate in situ within the tongue
- Cranial neural crest cells migrate into the developing tongue and give rise to connective tissue and vasculature
Boundary Between Anterior and Posterior Tongue
- The line of fusion of the two embryological parts is marked by the terminal sulcus - a V-shaped groove on the dorsum of the tongue
- At the apex of the V lies the foramen cecum - the site where the thyroid diverticulum originated and descended to become the thyroid gland
- If the thyroglossal duct fails to obliterate (normally by 6 weeks), a thyroglossal duct cyst results - it runs from foramen cecum down to the thyroid, passing through or near the hyoid bone
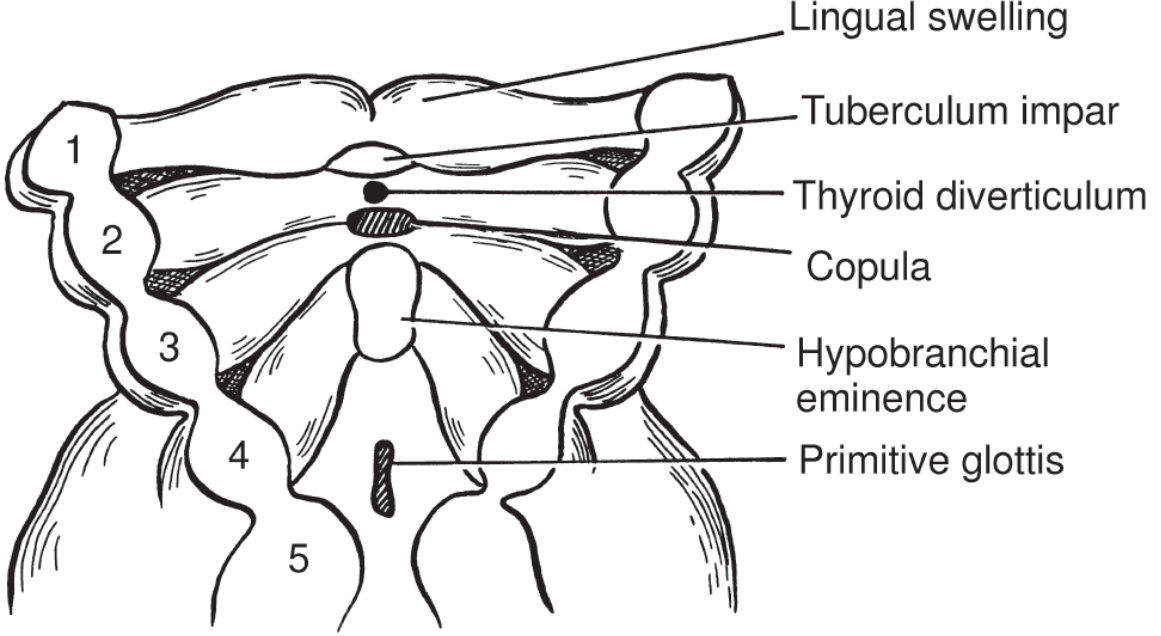
The spatial relationship between tongue swellings and the thyroid diverticulum at 4 weeks.
Papillae and Taste Buds - Timeline
| Structure | Timing | Nerve |
|---|
| Vallate (circumvallate) papillae | End of 8th week (also by 8th-20th wk) | CN IX |
| Foliate papillae | End of 8th week | CN IX |
| Fungiform papillae | Shortly after vallate; by 11th week | CN VII (chorda tympani) |
| Filiform papillae | 10-11 weeks (early fetal period) | Touch sensation only (no taste) |
| Taste buds | Weeks 11-13 | CN VII, IX, X |
- Taste buds form by inductive interaction between tongue epithelium and invading gustatory nerve fibers
- Fetal taste responses to bitter substances are detectable at 26-28 weeks
Molecular Signals
- Myogenic regulatory factors - guide muscle development
- Wnt/Notch signaling pathway - pattern formation
- PAX3 and PAX7 (paired box genes) - specification of myogenic precursors
Clinical Correlation: Ankyloglossia (Tongue-Tie)
Failure of normal dissolution of the lingual frenulum results in ankyloglossia - the tongue tip is tethered to the floor of the mouth, restricting tongue movement.
Key Points to Remember
- Tongue development begins at the end of week 4
- Tuberculum impar = first swelling to appear; median, triangular, from 1st arch
- Lateral lingual swellings = distal tongue buds; overgrow tuberculum impar → form anterior 2/3
- Hypobranchial eminence (copula of His) = from 2nd, 3rd, 4th arches; cranial part → posterior 1/3 of tongue
- 2nd arch (copula) is overgrown by 3rd arch tissue - that's why posterior tongue is CN IX, not CN VII
- Foramen cecum = remnant of thyroid descent; sits at the apex of terminal sulcus
- Tongue muscles = from occipital myotomes; innervated by CN XII
- Terminal sulcus = boundary between anterior 2/3 and posterior 1/3
Sources: The Developing Human (Moore), Langman's Medical Embryology, K.J. Lee's Essential Otolaryngology, Cummings Otolaryngology