Explain to me the whole chapter on neck dissection. For a MS ENT student. Keep all key concepts. Avoid using abbreviations. Include diagrams.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Neck Dissection - A Comprehensive Guide for the MS ENT Student
Source: Cummings Otolaryngology Head and Neck Surgery, Chapter 118; Scott-Brown's Otorhinolaryngology; K.J. Lee's Essential Otolaryngology
1. DEFINITION AND PURPOSE
Neck dissection is a surgical procedure designed to remove metastatic cancer involving the cervical lymph nodes. It is the most effective therapy to eradicate metastatic cancer involving the cervical lymphatics.
Since its early use, the procedure has evolved from radical extirpation to focused removal based on biologic risk and patterns of spread - consequently, its morbidity has been substantially reduced.
2. HISTORICAL PERSPECTIVE
- 1880 - Kocher: First concept of removing lymph nodes from the submandibular triangle for tongue cancer. He used a Y-shaped incision extending from the mastoid to the level of the omohyoid.
- Packard: Around the same time, also advocated removal of surrounding nodes for lingual cancer.
- Jawdynski (Polish surgeon): First formal description of what we now call the radical neck dissection.
- Crile (most credited): Demonstrated that head and neck metastases spread primarily through cervical lymphatics rather than hematogenously. His en bloc resection from the mandible to the clavicle became the basis of the radical neck dissection. Notably, Crile himself recommended preservation of the internal jugular vein and sternocleidomastoid muscle in patients with no palpable nodes, foreshadowing the modern concept of selective dissection.
- Suarez (1963) and Bocca: Advocated the functional neck dissection - removing all cervical lymph nodes while preserving the sternocleidomastoid muscle, internal jugular vein, and spinal accessory nerve, showing comparable oncologic results.
- Robbins et al. (1991/2002): American Head and Neck Society standardized the current classification system.
3. CERVICAL LYMPH NODE LEVELS
The lymph nodes in the neck are grouped into six major levels, numbered I through VI, with sublevels A and B for levels I, II, and V.
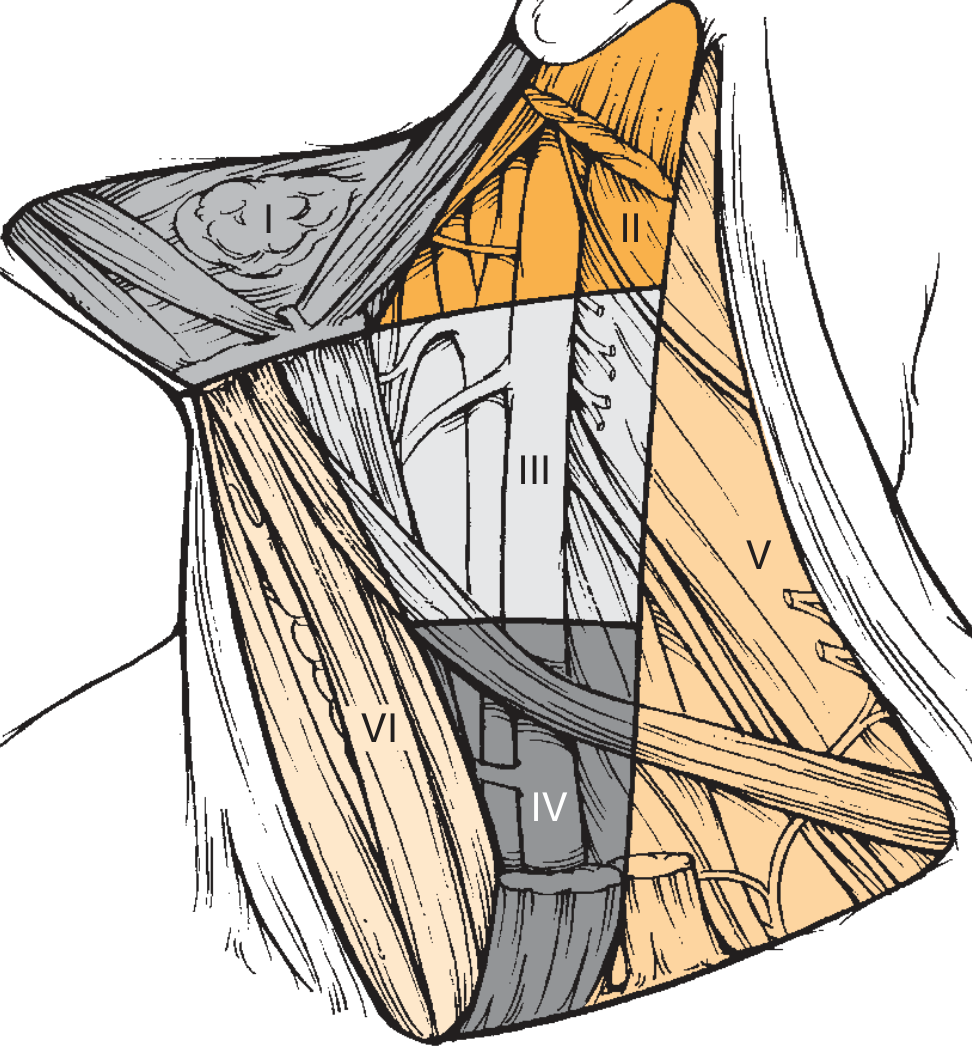
Fig. 118.1 - The six levels of the neck. (Cummings Otolaryngology)
Level I - Submental and Submandibular Nodes
- Level IA (Submental): Nodes within the submental triangle. Boundaries: anterior belly of both digastric muscles and the hyoid bone.
- Level IB (Submandibular): Nodes within the submandibular triangle. Boundaries: anterior and posterior bellies of the digastric muscle and the body of the mandible.
- The submandibular gland is removed during dissection to ensure complete removal of all nodes within this triangle.
- Note: Perifacial nodes (Nodes of Stahr, buccinator nodes) lie outside this triangle, superior to the mandibular body. These are at risk for lip, buccal mucosa, anterior nasal cavity, and cheek cancers.
Level II - Upper Jugular Nodes
- Located around the upper third of the internal jugular vein, adjacent to the spinal accessory nerve.
- Superior border: Skull base
- Inferior border: Carotid bifurcation (surgical) / hyoid bone (clinical)
- Lateral border: Posterior border of the sternocleidomastoid
- Medial border: Stylohyoid muscle
- Level IIA: Nodes anterior to the vertical plane defined by the spinal accessory nerve (most commonly involved by head and neck cancers)
- Level IIB: Nodes posterior to the spinal accessory nerve (less commonly involved in clinically node-negative patients)
Level III - Middle Jugular Nodes
- Located around the middle third of the internal jugular vein.
- Superior border: Carotid bifurcation (surgical) / inferior aspect of hyoid body (clinical/radiologic)
- Inferior border: Junction of the omohyoid with the internal jugular vein (surgical) / inferior border of cricoid arch (clinical/radiologic)
- Lateral border: Posterior border of the sternocleidomastoid
- Medial border: Lateral border of the sternohyoid muscle
Level IV - Lower Jugular Nodes
- Located around the lower third of the internal jugular vein.
- Superior border: Junction of the omohyoid with the internal jugular vein
- Inferior border: Clavicle
- Lateral border: Posterior border of the sternocleidomastoid
- Medial border: Lateral border of the sternohyoid
Level V - Posterior Triangle Nodes
- Located in the posterior triangle, around the lower half of the spinal accessory nerve and the transverse cervical artery.
- Level VA: Superior - around the spinal accessory nerve
- Level VB: Inferior - around the transverse cervical vessels and supraclavicular nodes
- Boundaries: Posterior border of the sternocleidomastoid (anterior), anterior border of the trapezius (posterior), and the clavicle (inferior).
Level VI - Anterior Compartment (Central Compartment) Nodes
- Pretracheal and paratracheal nodes, precricoid (Delphian) node, and perithyroidal nodes including the lymph nodes along the recurrent laryngeal nerves.
- Boundaries: Hyoid bone (superior), suprasternal notch (inferior), medial border of carotid sheaths bilaterally (lateral).
Level VII (proposed)
- Superior mediastinal nodes below the suprasternal notch down to the innominate artery.
- Relevant for thyroid cancer with mediastinal spread.
4. PATTERNS OF NODAL SPREAD BY PRIMARY SITE
A key concept for the MS ENT student is understanding which levels are at risk based on the primary tumor site. This is the scientific rationale for selective neck dissection.
Landmark studies by Lindberg (1972) and Shah (retrospective study of radical neck dissection specimens) established these patterns:
| Primary Site | Levels Most at Risk |
|---|---|
| Oral cavity (tongue, floor of mouth, buccal mucosa) | I, II, III |
| Oropharynx (tongue base, tonsil) | II, III, IV |
| Hypopharynx (piriform sinus) | II, III, IV |
| Supraglottic larynx | II, III, IV |
| Glottic larynx (T1/T2) | Very low risk of nodal spread |
| Thyroid gland | VI (central), then II-V (lateral) |
| Nasopharynx | II, V (and retropharyngeal nodes) |
| Lip | I |
| Skin of face/scalp | I, II, parotid nodes |
Important principle (Shah's observation): When positive nodes are found outside the expected levels, disease is almost always also found in the levels of highest risk for that primary site. Skipping to unexpected levels in isolation is uncommon.
5. FACTORS INFLUENCING NODAL METASTASIS
The risk of lymph node metastasis is determined by:
- Histology: Squamous cell carcinoma has high propensity; well-differentiated tumors may have slightly lower risk
- Perineural invasion: Increases risk significantly
- Lymphovascular invasion (invasion of the tumor's microcirculation): Increases risk
- T stage: More advanced tumors carry a higher likelihood of nodal spread
- Primary site subsite: Piriform sinus, supraglottic larynx, and oral tongue have higher metastatic rates than buccal mucosa
6. TERMINOLOGY - TYPES BY INDICATION
| Term | Definition |
|---|---|
| Therapeutic neck dissection | Performed when metastatic cervical lymphadenopathy is clinically evident (palpable or radiologically detectable) |
| Elective neck dissection | Performed when there is no clinical or radiologic evidence of nodal disease, but the risk of occult microscopic metastasis is high enough to justify surgery |
| Planned neck dissection | Performed 6-8 weeks after completion of radiotherapy or chemoradiotherapy, regardless of clinical response, when the probability of residual disease is high |
| Salvage neck dissection | Performed when metastatic disease is clinically evident after previous treatment. Can be: Early salvage (persistent disease after chemoradiation) or Late salvage (recurrent disease - worse prognosis) |
When is elective neck dissection indicated?
The likelihood of occult disease must be high, AND the likelihood of successful surveillance and salvage must be low. As a general principle, a greater than 15-20% risk of occult nodal disease is commonly used as the threshold to justify elective neck dissection.
7. CLASSIFICATION OF NECK DISSECTION
The American Head and Neck Society classification is based on the premise that the Radical Neck Dissection is the standard procedure, and all others are modifications of it.
7A. Radical Neck Dissection (Standard)
Structures removed: All ipsilateral cervical lymph nodes (Levels I-V) + Sternocleidomastoid muscle + Internal jugular vein + Spinal accessory nerve (Cranial Nerve XI).
What it does NOT include by default: Postauricular nodes, suboccipital nodes, perinodal nodes (except tail of parotid), perifacial/buccinator nodes, retropharyngeal nodes, paratracheal nodes.
Indication: Extensive lymph node metastases with extracapsular extension involving the spinal accessory nerve and/or internal jugular vein. Rarely used today.
Incisions used:
- Hockey stick incision (most common)
- Boomerang incision
- McFee (double transverse horizontal incision) - good for previously irradiated necks
- Apron incision (bilateral hockey stick) - for bilateral neck dissection
7B. Modified Radical Neck Dissection
All lymph nodes of levels I-V are removed, but one or more of the three nonlymphatic structures (sternocleidomastoid, internal jugular vein, spinal accessory nerve) is preserved.
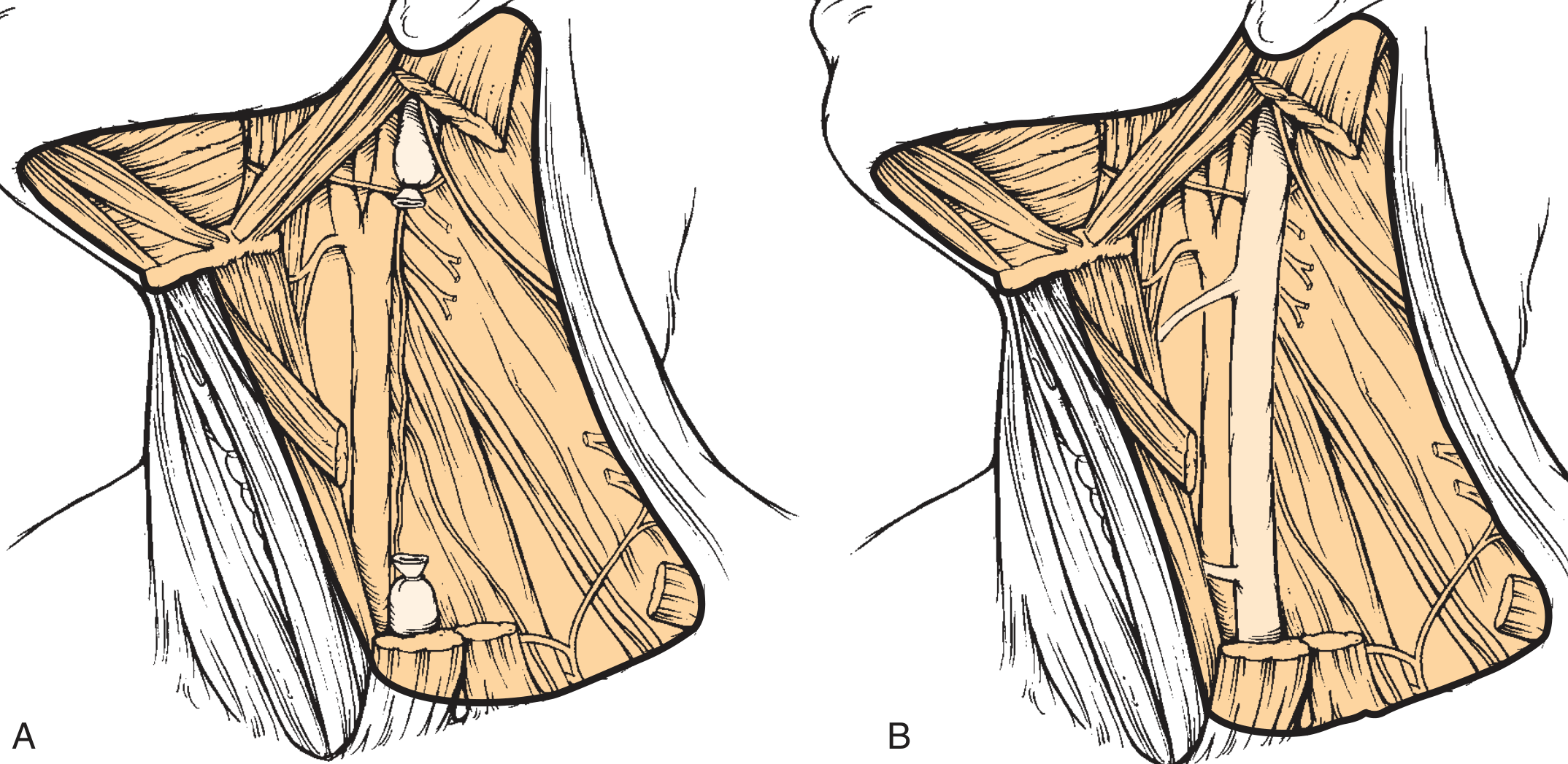
Fig. 118.8 - Modified radical neck dissection variants (Cummings Otolaryngology)
Three types are recognized:
- Type I: Preserve spinal accessory nerve only (sternocleidomastoid and internal jugular vein removed)
- Type II: Preserve spinal accessory nerve + internal jugular vein (sternocleidomastoid removed)
- Type III: Preserve all three structures (also called "functional neck dissection" per Bocca) - equivalent to what is often called Modified Radical Neck Dissection Type III
Rationale: Preserving the spinal accessory nerve avoids the serious morbidity of shoulder drop and chronic pain from denervation of the trapezius. Recurrence rates are comparable to radical neck dissection in selected cases.
7C. Selective Neck Dissection
Only one or more lymph node groups are removed, based on the primary site's known drainage patterns, while at least one of the groups normally removed in a radical neck dissection is preserved. The three nonlymphatic structures (sternocleidomastoid, internal jugular vein, spinal accessory nerve) are always preserved.
Named variants by primary site:
| Variant | Levels Removed | Used For |
|---|---|---|
| Supraomohyoid neck dissection | I, II, III | Oral cavity cancers |
| Lateral neck dissection | II, III, IV | Oropharynx, larynx, hypopharynx |
| Posterolateral neck dissection | II, III, IV, V (+ postauricular and suboccipital) | Posterior scalp, skin cancers |
| Central (anterior) compartment dissection | VI | Thyroid cancer, subglottic tumors |
Rationale (Lindberg and Shah studies): The topographic distribution of lymph node metastases is predictable in previously untreated squamous cell carcinoma. Removing only the at-risk levels achieves the same therapeutic value as more extensive dissection with less morbidity.
When to use selective vs radical/modified radical:
- Selective for clinically node-negative necks at significant risk, and for carefully selected node-positive (N1) disease without extracapsular spread
- Modified radical for node-positive disease without involvement of the nonlymphatic structures
- Radical only when the sternocleidomastoid, internal jugular vein, or spinal accessory nerve are directly invaded by tumor
7D. Extended Neck Dissection
Any of the above procedures extended to remove either additional lymph node groups or nonlymphatic structures not routinely included.
Examples of extension:
- Retropharyngeal nodes: Added when primary tumor involves the pharyngeal walls, tongue base, tonsil, or soft palate. Ballantyne found 44% incidence of retropharyngeal node involvement in posterior pharyngeal wall carcinomas.
- Superior mediastinal nodes (Level VII)
- Parotid nodes
- Hypoglossal nerve (Cranial Nerve XII), levator scapulae muscle, or carotid artery - when dictated by tumor extent
Carotid artery resection: Controversial. Carries 30% mortality and 45% cerebral complication rate historically. Only considered when frank carotid wall invasion is present and preoperative testing (balloon occlusion test with cerebral blood flow measurement) confirms tolerance. Saphenous vein grafts preferred over prosthetic grafts for reconstruction.
8. SURGICAL TECHNIQUE - RADICAL NECK DISSECTION (Step-by-Step)
Positioning
- Supine, roll under shoulders to extend the neck
- Skin prepped and draped to expose both sides of neck, face (mentum, mastoid processes, earlobes), and clavicles/suprasternal notch
Incision Planning
Incisions must:
- Allow full exposure of levels I-V
- Preserve maximum blood supply with broadly based flaps
- Avoid trifurcations overlying the carotid sheath
Preferred incisions: Hockey stick, boomerang, McFee. For bilateral neck dissection: apron incision.
Flap Elevation
- Skin flaps elevated in the subplatysmal plane
- Superior flap raised to the inferior border of the mandible
- Inferior flap to the clavicle
- The marginal mandibular branch of the facial nerve must be identified and preserved (runs just below and then loops above the inferior border of the mandible)
Key Surgical Steps (Radical Neck Dissection)
- Identify and ligate the external jugular vein at the superior and inferior extents
- Divide the sternocleidomastoid at its superior insertion (mastoid) and inferior insertion (sternum and clavicle)
- Expose the internal jugular vein - ligate and divide at superior (near skull base) and inferior (near clavicle/subclavian junction) ends
- Identify and sacrifice the spinal accessory nerve (in radical neck dissection)
- Dissect the nodal contents en bloc - from mandible to clavicle, sweeping the fatty areolar tissue with its enclosed nodes off the deep cervical fascia and deep cervical muscles
- Preserve during the dissection:
- Common, internal, and external carotid arteries
- Vagus nerve (Cranial Nerve X)
- Phrenic nerve (lies on the anterior surface of the anterior scalene muscle - must identify and protect)
- Hypoglossal nerve (Cranial Nerve XII) - unless disease requires its removal
- Lingual nerve
- Brachial plexus
- Thoracic duct on the left (ligate carefully if encountered to prevent chylous fistula)
- Submandibular triangle dissection: Remove the submandibular gland with its enclosed nodes
- Wound closure: Suction drains placed, platysma and skin closed in layers
9. COMPLICATIONS OF NECK DISSECTION
Intraoperative
| Complication | Notes |
|---|---|
| Hemorrhage | Internal jugular vein, external carotid vessels |
| Air embolism | From internal jugular vein injury |
| Chylous leak | Thoracic duct injury on the left; lymphatic duct on the right |
| Nerve injury | Spinal accessory, marginal mandibular facial, hypoglossal, lingual, phrenic, vagus, brachial plexus |
Postoperative
| Complication | Notes |
|---|---|
| Chylous fistula | Thoracic duct injury; presents as milky fluid in drain increasing with feeds. Managed with pressure, low-fat diet (medium chain triglycerides), or re-exploration |
| Facial/cerebral edema | Bilateral internal jugular vein ligation causes cerebral venous hypertension - avoid bilateral simultaneous internal jugular vein ligation |
| Shoulder dysfunction | Spinal accessory nerve sacrifice - trapezius denervation causes shoulder drop, chronic pain, and winging of scapula |
| Carotid artery rupture | Most feared lethal complication. Risk factors: salivary fistula, previous radiotherapy, malnutrition, diabetes. Management: manual pressure, proximal and distal ligation. Take "carotid precautions" in high-risk patients |
| Blindness | Rare - from ophthalmic vein thrombosis secondary to bilateral internal jugular vein ligation |
| Hematoma | Drain management essential |
| Wound infection | More common in previously irradiated patients |
| Pharyngocutaneous fistula | Particularly after combined surgery with pharyngeal resection |
| Phrenic nerve injury | Ipsilateral diaphragm paralysis |
Carotid precautions (for high-risk exposure): Keep compatible blood available, keep surgical instruments at bedside, educate nursing and house staff on signs and immediate management.
10. EXTRACAPSULAR SPREAD - A CRITICAL PROGNOSTIC FACTOR
Extracapsular spread (ECS) refers to tumor extension through the lymph node capsule into the surrounding soft tissue. It is one of the most important adverse prognostic factors in head and neck cancer:
- Macroscopic extracapsular spread: 44% recurrence rate (Carter et al.)
- Microscopic extracapsular spread: 25% recurrence rate
- Multiple nodes positive (4 or more): Dramatically worse 4-year survival
- Multiple levels involved: 71% recurrence vs 36.5% with single level (Strong)
Implication: Extracapsular spread is a major indication for postoperative adjuvant radiotherapy or chemoradiotherapy following neck dissection.
11. OUTCOMES BY TYPE OF NECK DISSECTION
| Procedure | Node-Negative Recurrence | Node-Positive Recurrence |
|---|---|---|
| Radical neck dissection | 3-7% | Variable with extent of extracapsular spread |
| Modified radical neck dissection | 4-7% (no longer used for N0) | 0-20% |
| Supraomohyoid (SND I-III) - N0 | 5.8% (Byers); 5% (Medina) | 10% (single node, no ECS); 24% (multiple/ECS) |
| Lateral neck dissection (SND II-IV) - N0 | 3.9% | 7.3% |
12. NECK DISSECTION AFTER CHEMORADIATION
One of the most complex clinical scenarios in head and neck oncology:
- Treatment with chemoradiotherapy may achieve organ preservation but makes the neck difficult to evaluate clinically and radiologically
- A planned neck dissection is done 6-8 weeks after completing chemoradiotherapy when the risk of residual disease is high
- Assessment uses Positron Emission Tomography / Computed Tomography (PET/CT) imaging - but this is unreliable before 3 months post-treatment
- For N0 or N1 disease with complete clinical response after chemoradiation: neck dissection is indicated only if persistent regional disease is evident
- For N2 or N3 disease: the current debate is whether to perform planned neck dissection in all cases or only in those with a poor response. Current evidence increasingly supports reserving neck dissection for those with PET-CT confirmed persistent disease after 12 weeks
- A late salvage neck dissection (for recurrent disease after complete response) carries a worse prognosis than an early salvage procedure (for persistent disease)
13. SENTINEL LYMPH NODE BIOPSY
A modern alternative to elective neck dissection in selected cases (mainly melanoma and increasingly oral cavity squamous cell carcinoma):
Principle: The first lymph node to receive drainage from a primary tumor (the "sentinel node") is the most likely node to contain occult metastasis. Its histological status predicts the status of the remaining nodes.
Technique:
- Lymphoscintigraphy (1-24 hours preoperatively): Technetium-99m-labeled sulfur colloid or Technetium-99m Tilmanocept (binds to CD206 receptors on macrophages and dendritic cells) injected intradermally at the primary site
- Two-dimensional nuclear imaging or SPECT/Computed Tomography to map draining sentinel nodes
- Intraoperative: Isosulfan blue dye injected at primary site + handheld gamma probe used to detect the radioactive sentinel node
- The sentinel node (typically 3-4 nodes removed until the gamma probe reading drops to less than 10% of the highest reading from removed nodes) is excised
- Pathology: Standard sectioning + H&E staining + immunohistochemistry with HMB-45, S-100, and Melan-A (for melanoma)
Indications (melanoma): T2-T3 tumors (depth 1-4 mm), Clark level IV or V, or ulcerated lesions, with clinically negative nodes.
If positive: Completion neck dissection is considered (though the role is debated - improves regional control and provides staging but may not improve overall survival per the Multicenter Selective Lymphadenectomy Trial - MSLT-II data).
14. CLASSIFICATION SUMMARY TABLE
| Procedure | Lymph Node Levels | Sternocleidomastoid | Internal Jugular Vein | Spinal Accessory Nerve |
|---|---|---|---|---|
| Radical neck dissection | I-V | Removed | Removed | Removed |
| Modified radical neck dissection Type I | I-V | Removed | Removed | Preserved |
| Modified radical neck dissection Type II | I-V | Removed | Preserved | Preserved |
| Modified radical neck dissection Type III (Functional) | I-V | Preserved | Preserved | Preserved |
| Supraomohyoid (selective) | I-III | Preserved | Preserved | Preserved |
| Lateral (selective) | II-IV | Preserved | Preserved | Preserved |
| Posterolateral (selective) | II-V + suboccipital | Preserved | Preserved | Preserved |
| Central compartment (selective) | VI | Preserved | Preserved | Preserved |
| Extended | I-V + additional | Variable | Variable | Variable |
15. MODERN TRENDS AND EVOLVING CONCEPTS
- Super-selective neck dissection: Removing only the single level most at risk, further reducing morbidity without compromising oncologic results
- Robotic and endoscopic (minimally invasive) neck dissection: Transaxillary or retroauricular approaches for thyroid cancer and parotid tumors, avoiding visible neck scars
- Sentinel lymph node biopsy expanding role: Now recommended for early oral cavity squamous cell carcinoma (T1-T2 N0) in many guidelines
- Deintensification in human papillomavirus-positive oropharyngeal cancer: Ongoing trials to see whether less aggressive neck treatment is appropriate in this excellent-prognosis group
- Positron Emission Tomography-guided management: Replacing planned neck dissection in many N2/N3 cases after chemoradiation, reserving surgery for incomplete responders
QUICK REVIEW - HIGH-YIELD EXAM POINTS
- The Radical Neck Dissection removes levels I-V + sternocleidomastoid + internal jugular vein + spinal accessory nerve
- The six levels are based on the Memorial Sloan Kettering Group classification
- Most important complication: Carotid artery rupture (lethal)
- Most common morbidity of classical radical neck dissection: Shoulder drop from spinal accessory nerve sacrifice
- Chylous fistula: Left-sided (thoracic duct) >> right-sided (right lymphatic duct)
- Bilateral internal jugular vein ligation must be avoided or staged - risk of fatal cerebral edema and blindness
- Oral cavity drains to levels I, II, III; pharynx/larynx to levels II, III, IV
- Extracapsular spread mandates adjuvant radiotherapy or chemoradiotherapy
- A planned neck dissection is done 6-8 weeks after chemoradiation
- Salvage for recurrent disease has a worse prognosis than salvage for persistent disease
- The phrenic nerve lies on the anterior scalene - must protect it during level IV dissection
Primary Reference: Cummings Otolaryngology Head and Neck Surgery, Chapter 118 (Ronen, Samant, Robbins); Scott-Brown's Otorhinolaryngology Head & Neck Surgery; K.J. Lee's Essential Otolaryngology, Chapter on Neck Dissection.
This is a shared conversation. Sign in to Orris to start your own chat.