I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Acute Peritoneal Dialysis
Definition
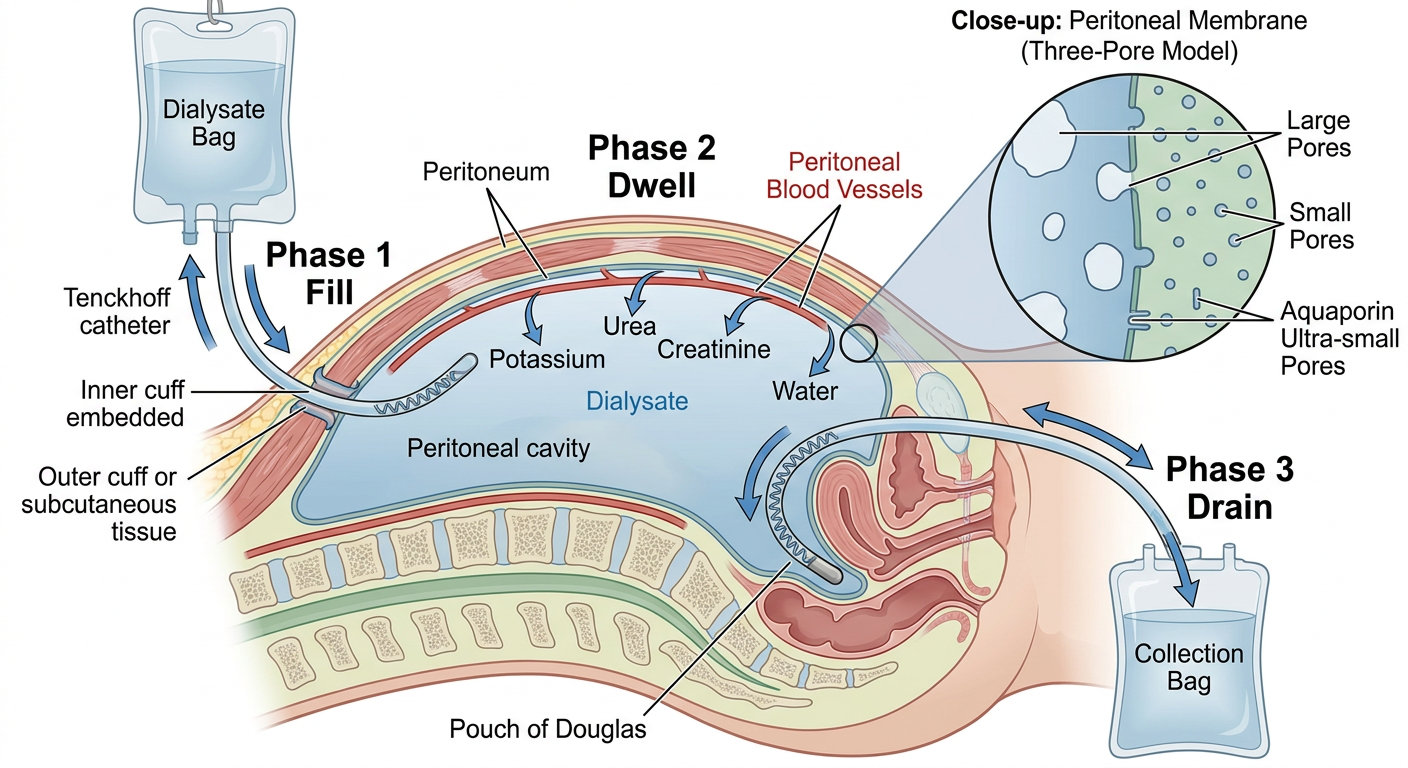
Peritoneal dialysis (PD) is a renal replacement therapy that uses the peritoneal membrane - the serous, semipermeable lining of the abdominal cavity - as a natural dialysis filter. Cleansing fluid (dialysate) is instilled into the peritoneal cavity via a catheter, where it absorbs waste products, excess electrolytes, and fluid from the peritoneal blood vessels by diffusion and osmosis. The spent fluid is then drained and discarded.
Acute peritoneal dialysis (APD) specifically refers to PD used for acute kidney injury (AKI) rather than end-stage kidney disease. It is an attractive modality for AKI because it is as effective as hemodialysis, requires far less infrastructure, and can be performed with solutions and catheters adapted to local resources - making it especially valuable in low-resource settings.
- Brenner and Rector's The Kidney, p. 3233
Physiological Basis
The peritoneal membrane functions on a three-pore model:
- Large pores (>150 Å) - transport proteins and large solutes
- Small pores (40-45 Å) - main route for small solute exchange (urea, creatinine, electrolytes)
- Ultra-small pores / aquaporins (2-5 Å) - water-only transport (free water removal)
The adult peritoneum has a surface area of 1.6-2.0 m², but microvilli increase total functional surface area up to 40 m². Solute transfer occurs by:
-
Diffusion - down concentration gradients from blood into dialysate
-
Convection (ultrafiltration) - water and solutes dragged across by osmotic pressure from dextrose in dialysate
-
Osmosis - free water movement through aquaporins
-
Brenner and Rector's The Kidney, p. 2094-2095
Apparatus and Access
1. Peritoneal Catheter (Primary Access)
The catheter is the cornerstone of PD. The most widely used is the Tenckhoff catheter, made of silicone rubber or polyurethane.
| Component | Details |
|---|
| Intraperitoneal portion | Straight, coiled, Ash (T-Fluted), or with silicone disc |
| Extraperitoneal portion | Straight or swan-neck design |
| Cuffs | Single or double Dacron cuffs; most common = double cuff, swan-neck, coiled Tenckhoff |
| Placement | Placed between visceral and parietal peritoneum near the pouch of Douglas |
Placement techniques:
- Blind (Seldinger) technique
- Surgical (open) placement
- Peritoneoscopic approach
- Laparoscopic placement
- Moncrief-Popovich technique
- Fluoroscopic ± real-time ultrasound guidance
The coiled catheter decreases pain during infusion and reduces migration risk. The swan-neck design reduces cuff extrusion and exit-site infection. The inner cuff is placed in the rectus muscle to prevent leaks; the outer cuff sits in subcutaneous tissue to prevent infection migration.
For acute/urgent PD, low-volume PD can begin within 24 hours of catheter placement if no other dialysis access is available; typically PD starts 2-4 weeks after placement to allow wound healing.
- Brenner and Rector's The Kidney, p. 2914; Campbell-Walsh Wein Urology, p. 2914
2. Dialysate Solutions
| Component | Details |
|---|
| Osmotic agent | Dextrose (glucose) at 1.5%, 2.5%, or 4.25%; or icodextrin (glucose polymer) |
| Buffer | Lactate (conventional) or bicarbonate (biocompatible solutions) |
| Electrolytes | Na⁺, K⁺, Ca²⁺, Mg²⁺ in physiologic concentrations |
| pH | Conventional: acidic (pH ~5.5); biocompatible: physiologic pH (neutral) |
-
1.5% dextrose - least ultrafiltration, used for maintenance
-
2.5% dextrose - moderate ultrafiltration
-
4.25% dextrose - maximum ultrafiltration, used for fluid-overloaded patients; more glucose absorption and hyperglycemia risk
-
Icodextrin - a glucose polymer minimally absorbed; maintains osmotic gradient for up to 18 hours in long dwells; color-coded commercially (yellow = 1.5%, green = 2.5%, red = 4.25%)
-
Washington Manual of Medical Therapeutics, p. 505
3. Cycler (Automated PD Machine)
In automated PD, a cycler machine performs preprogrammed exchanges overnight while the patient sleeps. It controls inflow volume, dwell time, and drainage automatically.
Procedure
Phases of Each PD Exchange ("Dwell Cycle")
- Fill (Infusion) - Dialysate flows by gravity or pump into the peritoneal cavity (typically 2-3 L for adults; 1.25-1.5 L/m² body surface area)
- Dwell - Fluid dwells in the peritoneum; diffusion and osmosis occur across the membrane (duration varies by modality)
- Drain - Used dialysate drains out by gravity via the catheter and is discarded
Key Prescription Variables
- Dwell volume (2-3 L typical)
- Dwell time
- Number of exchanges per day
- Dextrose concentration
Modalities
1. Continuous Ambulatory PD (CAPD) - Manual
- Patient manually performs 3-5 exchanges per day
- Each exchange takes 30-40 minutes
- Fluid dwells continuously; no machine required
- Overnight long dwell with slow equilibration
- Works at home, work, or while traveling
2. Automated PD (APD) / Continuous Cycling PD (CCPD)
- A cycler machine runs multiple exchanges overnight (typically 8-10 hours)
- A final fill remains in the peritoneum during the daytime
- Frees the patient from daytime exchanges
- Preferred for patients working during the day
3. Tidal PD (a variant of APD)
- A portion of dialysate always remains in the peritoneum ("tidal volume"), reducing pain from repeated complete drainage
4. Intermittent PD (IPD) - used for acute setting
- Exchanges performed periodically (e.g., several hours per day, not continuous)
- Traditional approach for acute PD in hospitalized patients
| Feature | APD | CAPD |
|---|
| Cost | Higher ($$$$) | Lower ($$) |
| Mechanical complications (hernia, leaks) | Lower risk (dry day option) | Higher risk |
| Catheter complications | Drain pain, alarms | Easier for "fussy" catheters |
| Assisted PD (elderly) | Easier (1-2 nurse visits/day) | More challenging |
| Cirrhosis/ascites | More challenging | Can control drain volume |
| Urgent start | Lower leak risk | Higher mechanical complications |
- National Kidney Foundation Primer, p. 611
Advantages of Acute PD
Clinical:
- Effective solute and fluid removal - comparable to hemodialysis for AKI
- Continuous therapy, more closely mimicking natural kidney function
- Gradual fluid removal reduces hemodynamic instability (better tolerated in hypotensive patients)
- Preserves residual kidney function longer than hemodialysis
- Needle-free - no vascular access needed
- Fewer dietary restrictions (less inter-dialytic build-up of K⁺, Na⁺, fluid)
- Reduced cardiovascular stress (no rapid extracorporeal fluid shifts)
Practical:
-
Requires far less infrastructure than hemodialysis - suitable for low-resource settings
-
Can use locally manufactured/adapted solutions and catheters
-
No need for anticoagulation (unlike hemodialysis with extracorporeal circuits)
-
Can be performed at home by patients or caregivers
-
Allows travel; supplies shipped directly
-
Can dialyze while sleeping (APD)
-
Can be started within 24 hours in urgent AKI if no other access available
-
Brenner and Rector's The Kidney, p. 3233
Disadvantages and Complications of Acute PD
Infectious Complications
| Complication | Details |
|---|
| Peritonitis | Most serious; up to 6% mortality per episode. Diagnosed by: cloudy effluent + dialysate WBC >100/µL (>50% neutrophils) + positive culture. Treat with intraperitoneal antibiotics (vancomycin or 1st-gen cephalosporin + 3rd-gen cephalosporin or aminoglycoside) |
| Exit-site infection | Erythema, tenderness, purulent drainage at catheter exit |
| Tunnel infection | Infection along subcutaneous catheter track |
Non-Infectious Complications
- Hernia formation - due to increased intra-abdominal pressure from fluid dwell
- Dialysate leaks - especially with early catheter use
- Back pain - from increased intra-abdominal pressure
- Catheter migration / obstruction - outflow failure requiring repositioning
- Hydrothorax - dialysate leaking into pleural space through diaphragmatic defects
- Hyperglycemia - from glucose absorption, especially with high-dextrose solutions
- Weight gain / abdominal distension - from glucose absorption
- Protein loss - significant protein lost in dialysate, contributing to malnutrition
- Ultrafiltration failure - especially in high peritoneal transporters on long-dwell regimens
Modality Limitations
-
Less efficient per session than conventional intermittent hemodialysis (compensated by continuous nature)
-
Must be performed daily (7 days/week) - schedule burden
-
Requires strict sterile technique training and patient compliance
-
Large patients may need extra therapy volume
-
Requires home storage space for supplies and machine
-
Some healthcare providers less familiar with PD than HD, leading to under-referral
-
Contraindicated or difficult in: recent abdominal surgery, extensive adhesions, active abdominal infection (relative), large body habitus, respiratory failure (intolerance of raised intra-abdominal pressure), severe malnutrition with very low serum albumin
-
Washington Manual of Medical Therapeutics, p. 505-506; Brenner and Rector's The Kidney
Special Considerations: Acute PD in AKI and Low-Resource Settings
Acute PD is particularly valued in resource-limited settings (Africa, Asia, parts of South America) because:
-
HD requires electricity, treated water, trained staff, and expensive machines
-
PD can be done with minimal equipment and locally adapted materials
-
The "Saving Young Lives" initiative specifically promotes sustainable acute PD programs in very low-resource settings, particularly for children with AKI
-
It has been used successfully in COVID-19 AKI when CRRT machines were overwhelmed, though it was sometimes difficult in the most critically ill patients requiring prone positioning
-
Brenner and Rector's The Kidney, p. 3233, 3982
Summary Table: Acute PD at a Glance
| Aspect | Details |
|---|
| Definition | Peritoneal membrane used as dialysis filter in AKI |
| Access | Tenckhoff catheter (double cuff, swan-neck, coiled) |
| Dialysate | Dextrose 1.5/2.5/4.25% or icodextrin; lactate or bicarbonate buffer |
| Exchange phases | Fill → Dwell → Drain |
| Modalities | Intermittent PD (IPD), CAPD, APD/CCPD |
| Key advantage | Low infrastructure, continuous, hemodynamically gentle |
| Key risk | Peritonitis (6% mortality/episode), ultrafiltration failure |