Uptake and distribution of inhaled anaesthetics from Stoelting millers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have all the key content and images needed for a comprehensive answer. Let me now compose the full response directly from Miller's Anesthesia, Chapter 18.
Uptake and Distribution of Inhaled Anaesthetics
Miller's Anesthesia, 10th Edition - Chapter 18
Overview
Inhaled anaesthetics are both taken up and eliminated through alveolar blood-gas exchange, which allows drug dosage to be monitored in expired alveolar gases without requiring tissue-dependent metabolism for clearance. The fundamental goal is to establish and maintain an adequate partial pressure of anaesthetic in the CNS target tissues. This requires understanding how gas-phase compounds move through the circuit, alveoli, blood, and body tissue compartments.
1. Biophysical Properties: Partial Pressure, Hydrophobicity, and Partition Coefficients
Partial pressure is the thermodynamic force driving anaesthetic gas transfer between compartments. Anaesthetics move from regions of high partial pressure to low partial pressure, and equilibrium is achieved when partial pressures equalise across compartments. The partial pressure of an anaesthetic is usually reported as the percentage of the delivered gas mixture at 1 atm.
Partition coefficients describe how an anaesthetic distributes between two phases at equilibrium. The most clinically important are:
-
Blood/gas partition coefficient (λb/g): Describes how much anaesthetic dissolves in blood relative to the gas phase. A low λb/g (e.g., desflurane 0.45, sevoflurane 0.65) means less drug is "absorbed" by blood per unit of pressure - the alveolar partial pressure rises quickly, producing faster induction and emergence. A high λb/g (e.g., halothane 2.4, isoflurane 1.4) means blood acts as a reservoir that buffers and slows the rise in alveolar pressure.
-
Tissue/blood partition coefficients: Determine how anaesthetic distributes from blood into various tissue groups. Fat has particularly high tissue/blood coefficients for all volatile agents, making fat a large reservoir - though equilibration with fat is so slow it plays a relatively minor role during routine anaesthetics.
Key partition coefficients are summarised in the table below (Miller's Anesthesia, Table 18.1):
| Agent | Blood/Gas (λb/g) | Brain/Blood | Muscle/Blood | Fat/Blood |
|---|---|---|---|---|
| Desflurane | 0.45 | 1.3 | 2.0 | 27 |
| Sevoflurane | 0.65 | 1.7 | 3.1 | 48 |
| Isoflurane | 1.4 | 1.6 | 2.9 | 45 |
| Halothane | 2.4 | 1.9 | 3.4 | 51 |
| Nitrous oxide | 0.47 | 1.1 | 1.2 | 2.3 |
2. From Vaporiser to Alveoli: The Delivery Pathway
Fresh Gas Delivery
The volume of volatile anaesthetic (VA) delivered from the vaporiser is:
VA(t) = P_del × FGF × t
where P_del is the delivered anaesthetic partial pressure and FGF is fresh gas flow.
Breathing Circuit Wash-In
The speed at which gas from the anaesthesia machine replaces gas in the breathing circuit depends on FGF and the breathing circuit volume (V_circ). The process follows a single exponential:
- Time constant τ = V_circ / FGF
- If V_circ = 6 L and FGF = 6 L/min, τ = 1 min
- After 1τ: 63% of old gas replaced; after 3τ: ~95% replaced
Increasing FGF halves the time constant; doubling V_circ doubles it.
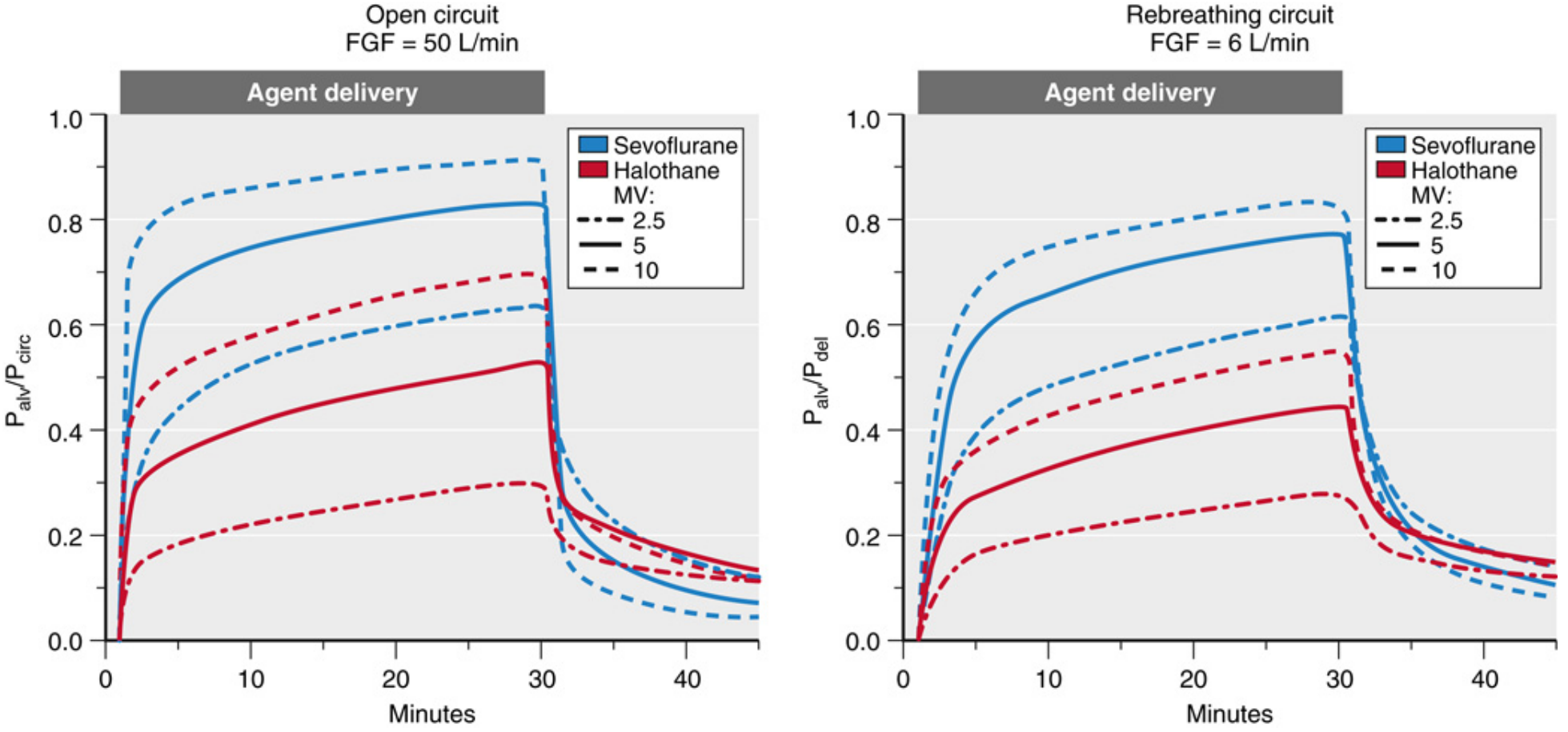
Alveolar Ventilation
Only alveolar ventilation (not total minute ventilation) participates in transpulmonary gas exchange. The alveolar anaesthetic partial pressure (P_alv or FA) is governed by:
dP_alv/dt = (V_alv / V_alv) × (P_circ - P_alv) - (Q / V_alv) × λb/g × (P_alv - P_MV)
The two opposing forces:
- Ventilation - drives P_alv toward P_circ (delivery)
- Pulmonary blood flow × solubility - removes anaesthetic from alveoli (uptake into blood)
Effect of ventilation (Fig. 18.4 below): Raising minute ventilation accelerates the rise of P_alv. The effect is greater for soluble agents (halothane) than insoluble agents (sevoflurane) because with insoluble agents, pulmonary uptake is already low and P_alv rises quickly regardless.
P_alv is of critical importance because:
- It is in rapid equilibrium with circulating blood and highly perfused tissues including the CNS target
- It can be measured in exhaled end-tidal gases - making end-tidal concentration a useful surrogate for brain concentration during steady state
3. Transpulmonary Uptake: Blood-Gas Exchange
The Fick Principle for Anaesthetic Uptake
Anaesthetic uptake into blood (rate of removal from alveoli) is:
dQ_gas/dt = Q × λb/g × (P_alv - P_MV)
where Q = cardiac output, λb/g = blood/gas partition coefficient, P_alv = alveolar partial pressure, P_MV = mixed venous partial pressure.
This equation explains three key clinical relationships:
| Factor | Effect on uptake | Consequence |
|---|---|---|
| Higher cardiac output (Q) | Increases uptake | Slows rise of P_alv; slower induction |
| Higher λb/g (more soluble) | Increases uptake | Slows rise of P_alv; slower induction |
| Higher P_MV | Reduces gradient | Slows uptake as anaesthetic accumulates in venous blood |
Effect of Cardiac Output
- High cardiac output (e.g., anxiety, thyrotoxicosis): More anaesthetic is removed from alveoli per unit time, slowing the P_alv rise and thus slowing induction. This effect is proportionally larger for soluble agents.
- Low cardiac output (e.g., shock): Conversely, low Q means less anaesthetic is taken up from alveoli; P_alv rises faster - an important risk for anaesthetic overdose. Halothane is most dangerous here because it reduces cardiac output the most, creating a positive feedback loop toward hemodynamic collapse.
4. Tissue Distribution: The Compartment Model
Tissue Groups
The body is modelled as four compartments based on perfusion and solubility:
| Group | Organs | % of Cardiac Output | Equilibration time |
|---|---|---|---|
| Vessel-Rich Group (VRG) | Brain, heart, liver, kidneys | ~75% | Minutes |
| Muscle | Skeletal muscle, skin | ~20% | Hours |
| Fat | Adipose tissue | ~5% | Many hours/days |
| Vessel-Poor Group | Bone, cartilage, tendons | ~1% | Very slow |
The Tissue Partial Pressure Rise
Each tissue compartment has its own effective "capacitance volume" = V_tissue × (tissue/blood partition coefficient). Larger effective volumes and lower blood flow means slower equilibration.
The figure below shows the characteristic pattern for sevoflurane:
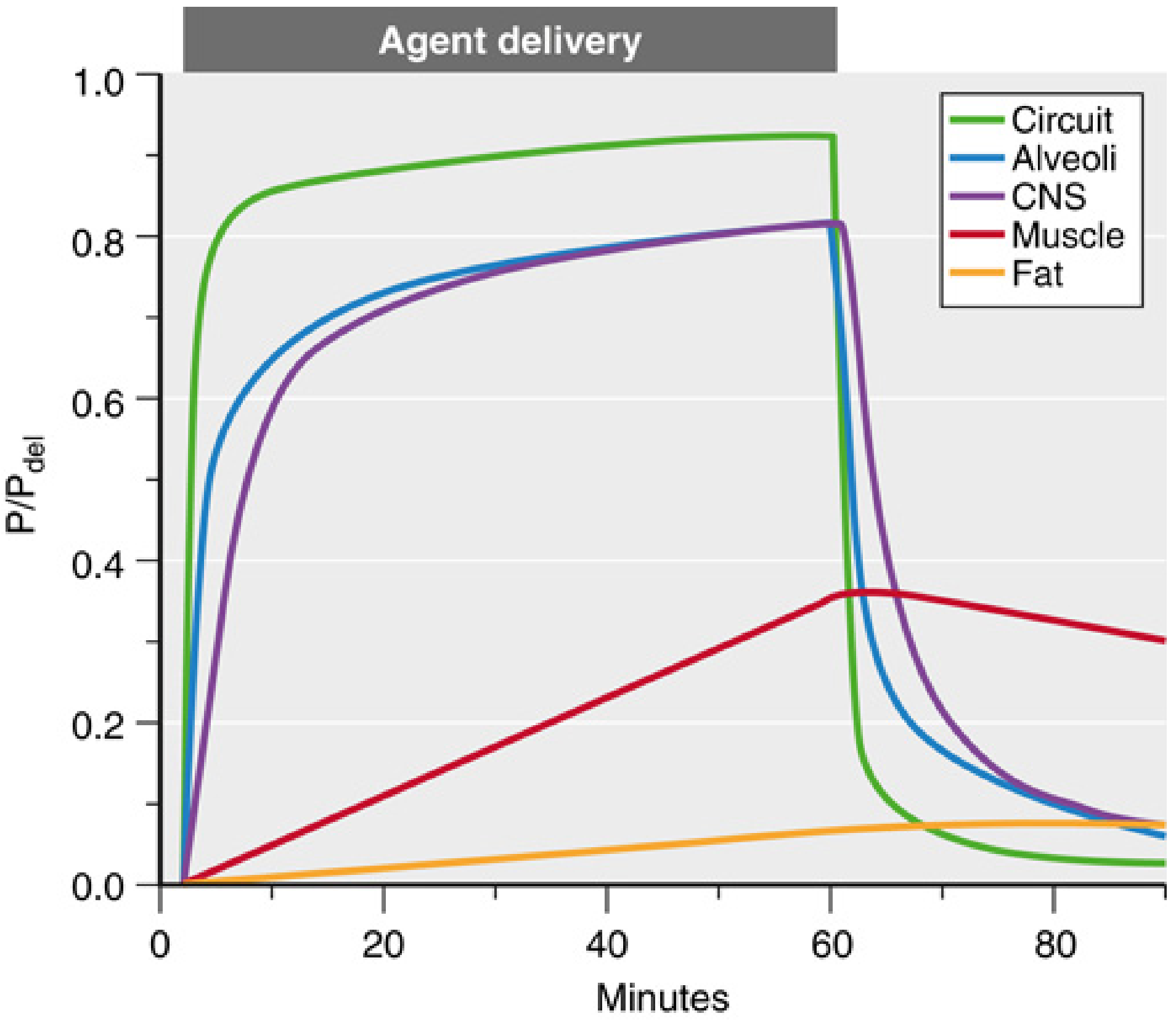
Key observations from this figure:
- CNS (VRG) equilibrates rapidly with P_alv - a lag of only a few minutes
- Muscle rises slowly and is still not at steady state after 60 minutes
- Fat rises so slowly it barely changes during a 1-hour anaesthetic
- After delivery stops, muscle continues to offload anaesthetic back into blood/alveoli, sustaining partial pressure and potentially prolonging emergence
Inter-Tissue Diffusion
In addition to blood-borne distribution, direct diffusion between adjacent tissues occurs at large interfacial surfaces - for example, anaesthetic diffuses from the highly perfused heart, liver, and kidneys into surrounding pericardial and abdominal fat.
Mixed Venous Partial Pressure (P_MV)
P_MV is the flow-weighted average of all venous outflows returning to the right heart. As P_MV rises during anaesthesia, the driving gradient for alveolar uptake (P_alv - P_MV) diminishes - uptake slows, and P_alv rises toward P_circ more easily. This is why the rate of P_alv rise accelerates over time.
5. Special Effects: Pulmonary Shunts, Concentration Effect, and Second Gas Effect
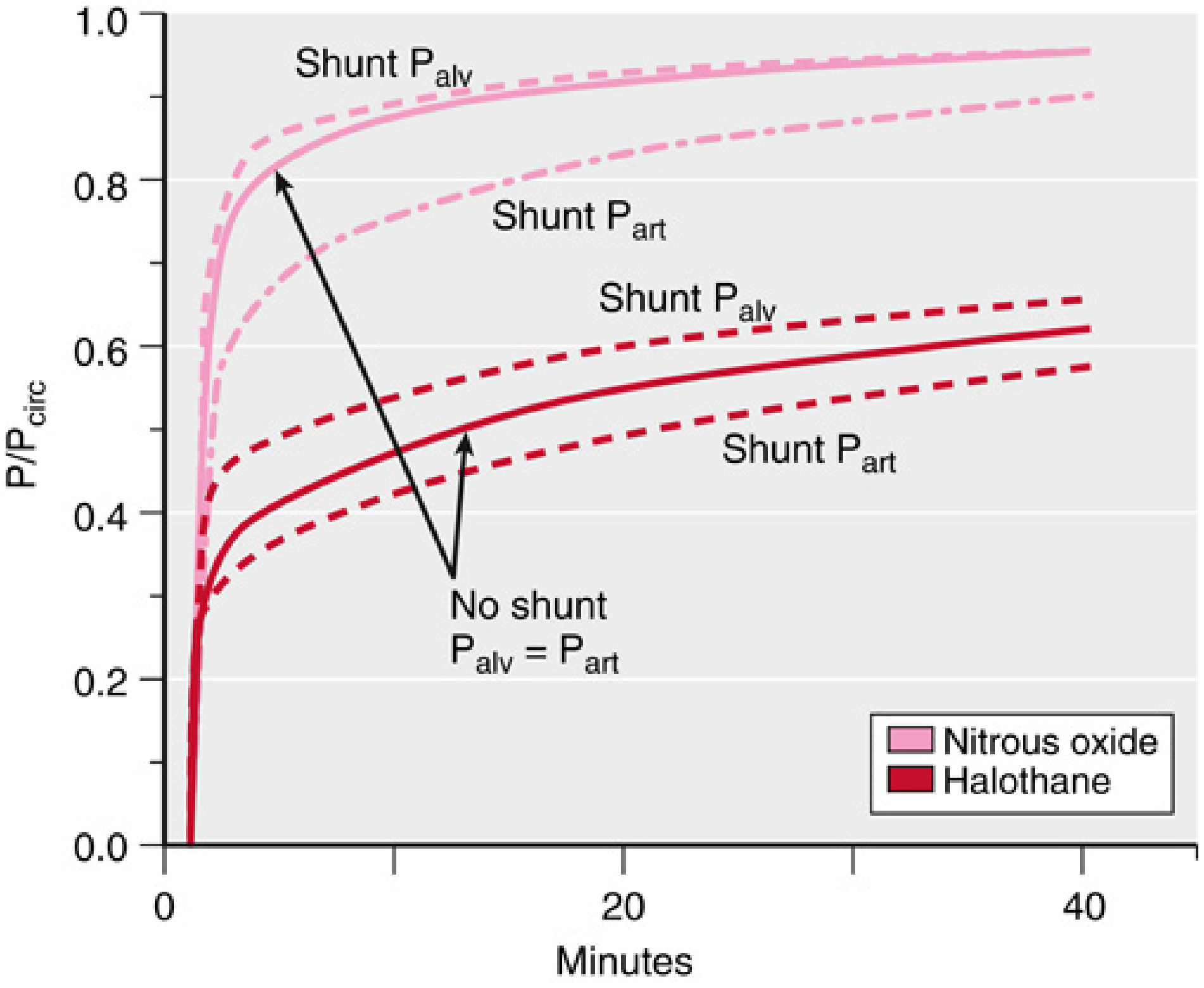
Right-to-Left Pulmonary Shunt
Shunted blood bypasses alveolar gas exchange:
- P_alv rises faster (less uptake from alveolar gas)
- But P_art rises more slowly (shunted mixed venous blood dilutes pulmonary venous blood)
- This discrepancy between P_alv and P_art is proportionally larger for insoluble agents (e.g., N2O) than for soluble agents
The Concentration Effect
When an anaesthetic is a large fraction of the inhaled mixture (e.g., N2O at 66%), its rapid uptake into blood reduces the volume of alveolar gas. This volume contraction concentrates the remaining gas, so the alveolar partial pressure of the anaesthetic falls less than expected. The result: P_alv / P_del rises faster than predicted from a simple model.
The Second Gas Effect
When N2O is inhaled at high concentrations, its rapid uptake reduces alveolar volume and effectively concentrates all other gases present ("second gases" such as isoflurane or O2). This increases their alveolar partial pressures and accelerates their uptake. Additionally, the reduction in expired gas volume creates a slight augmentation of effective inspiratory flow, further enhancing second-gas uptake.
6. Effect of Nitrous Oxide on Gas-Filled Spaces
Because N2O is used at high partial pressures and is far more soluble in blood than nitrogen (λb/g N2O = 0.47 vs N2 = 0.015), it diffuses into any air-containing body space much faster than N2 can diffuse out:
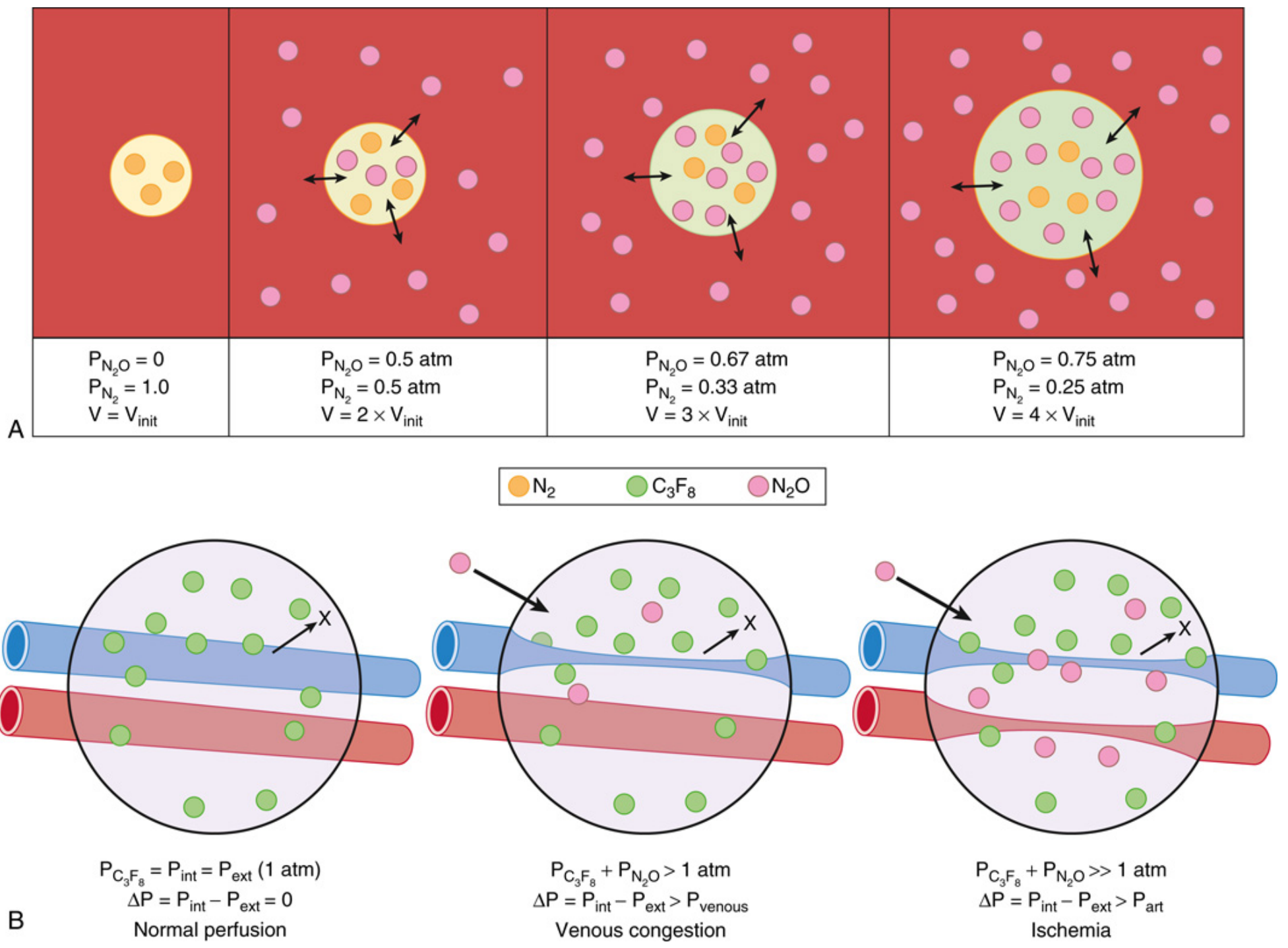
- Compliant spaces (e.g., intravascular air emboli, pneumothorax, GI tract): Volume expands up to 3-4x the original size
- Non-compliant spaces (e.g., middle ear, intravitreal gas after eye surgery with C3F8): Pressure rises, risking ischemia or barotrauma
- Clinically important: N2O is contraindicated when intravitreal gas bubbles are present (retinal surgery), in pneumothorax, and in bowel obstruction
7. Paediatric Considerations
Induction is faster in neonates and children due to:
- Higher MV/FRC ratio - alveolar partial pressure equilibrates with circuit more rapidly
- Greater proportion of cardiac output to VRG - brain equilibrates more rapidly
- Different tissue/blood partition coefficients contribute as well
The speed of induction creates greater overdose risk in neonates, especially if overpressure techniques (high inspired concentrations) are used. For example, a halothane vaporiser can deliver up to 5.75 MAC multiples vs 2.42 MAC multiples for sevoflurane.
Summary
The rise in alveolar anaesthetic partial pressure (FA/FI) is the net result of:
| Accelerates FA/FI rise | Slows FA/FI rise |
|---|---|
| High minute ventilation | Low ventilation |
| Low blood/gas solubility | High blood/gas solubility |
| Low cardiac output | High cardiac output |
| High P_MV (late in anaesthesia) | Low P_MV (early/induction) |
| Right-to-left shunt (P_alv, not P_art) | - |
| Concentration effect (N2O) | - |
The ultimate clinical target is the CNS partial pressure, which closely follows P_alv via the rapidly equilibrating vessel-rich group. Monitoring end-tidal anaesthetic concentration provides a reliable estimate of brain anaesthetic levels during steady state.
- Miller's Anesthesia, 10th Edition, Chapter 18 (Uptake and Distribution of Inhaled Anesthetics)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, Chapter 72 (paediatric aspects)
This is a shared conversation. Sign in to Orris to start your own chat.