Explain me 10 common heart diseases with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings images
Finding Sources
Reading Web Page
https://www.healio.com/cardiology/learn-the-heart/ecg-review…
Finding Sources
Reading File
Reading File
Searching the Web
ECG images atrial fibrillation myocardial infarction heart block pericarditis WPW site:ecgwaves.com OR site:lifeinthefastlane.com
Loading Image
Searching the Web
ECG examples STEMI atrial fibrillation complete heart block pericarditis hypertrophic cardiomyopathy pulmonary embolism images wikimedia OR ecgwaves
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have rich textbook content and ECG images. Let me compile the comprehensive answer.
10 Common Heart Diseases: ECG Changes & Images
Here is a structured, clinically detailed guide to 10 major cardiac conditions and their hallmark electrocardiographic features, sourced from Harrison's Principles of Internal Medicine 22E, Ganong's Review of Medical Physiology, Braunwald's Heart Disease, and Tintinalli's Emergency Medicine.
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing transmural ischemia and myocardial death.
ECG Changes:
- Hyperacute T waves - the earliest change (tall, broad, symmetric T waves)
- ST elevation - convex ("tombstone") or straight upsloping, at least 1 mm in two contiguous limb leads or 2 mm in precordial leads
- Reciprocal ST depression - in leads opposite to the infarct
- Pathological Q waves - develop within hours to days (>40 ms wide, >25% of QRS amplitude), indicating necrosis
- T wave inversion - evolves as infarction progresses
- Lead localization:
- Anterior STEMI: V1-V4 (LAD occlusion)
- Inferior STEMI: II, III, aVF (RCA occlusion)
- Lateral STEMI: I, aVL, V5-V6 (LCx occlusion)
- Posterior STEMI: ST depression + tall R in V1-V2 (mirror image)
"Severe, acute ischemia lowers the resting membrane potential and shortens the duration of the action potential... current flows between normal and ischemic zones... producing ST elevations and sometimes, in the earliest stages of ischemia, tall, positive so-called hyperacute T waves." - Harrison's Principles of Internal Medicine 22E
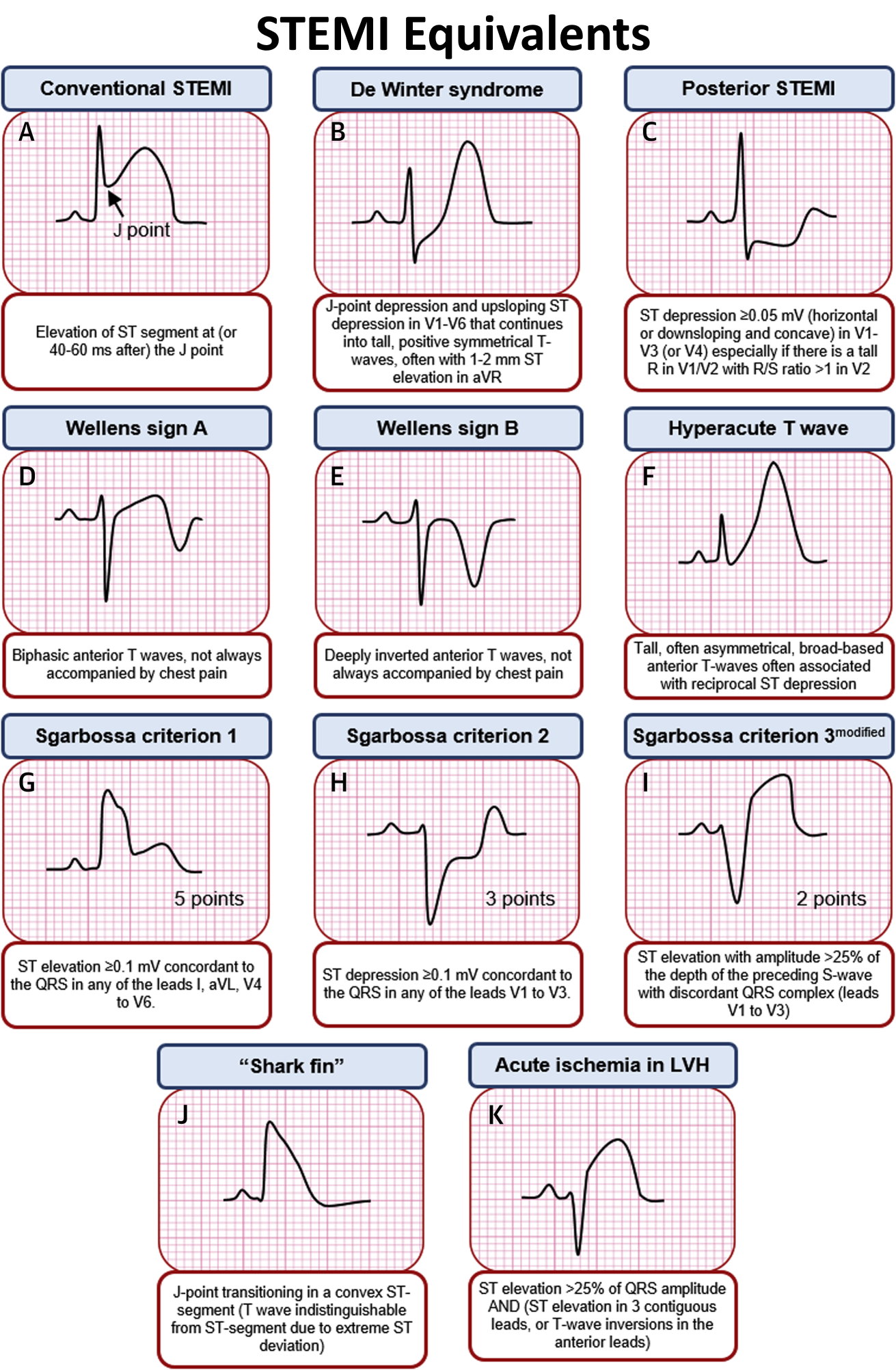
ST morphology guide (STEMI vs non-ischemic elevations):

STEMI equivalents (De Winter, Wellens, posterior patterns):
2. Non-ST Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
What it is: Partial coronary occlusion causing subendocardial ischemia without full-thickness infarction.
ECG Changes:
- ST depression - horizontal or downsloping (most specific for subendocardial ischemia); at least 0.5 mm in 2 contiguous leads
- T wave inversion - deep symmetric inversions, especially in anterior leads
- No pathological Q waves (by definition - no transmural necrosis)
- May be normal - up to 30% of NSTEMI patients have no ECG changes
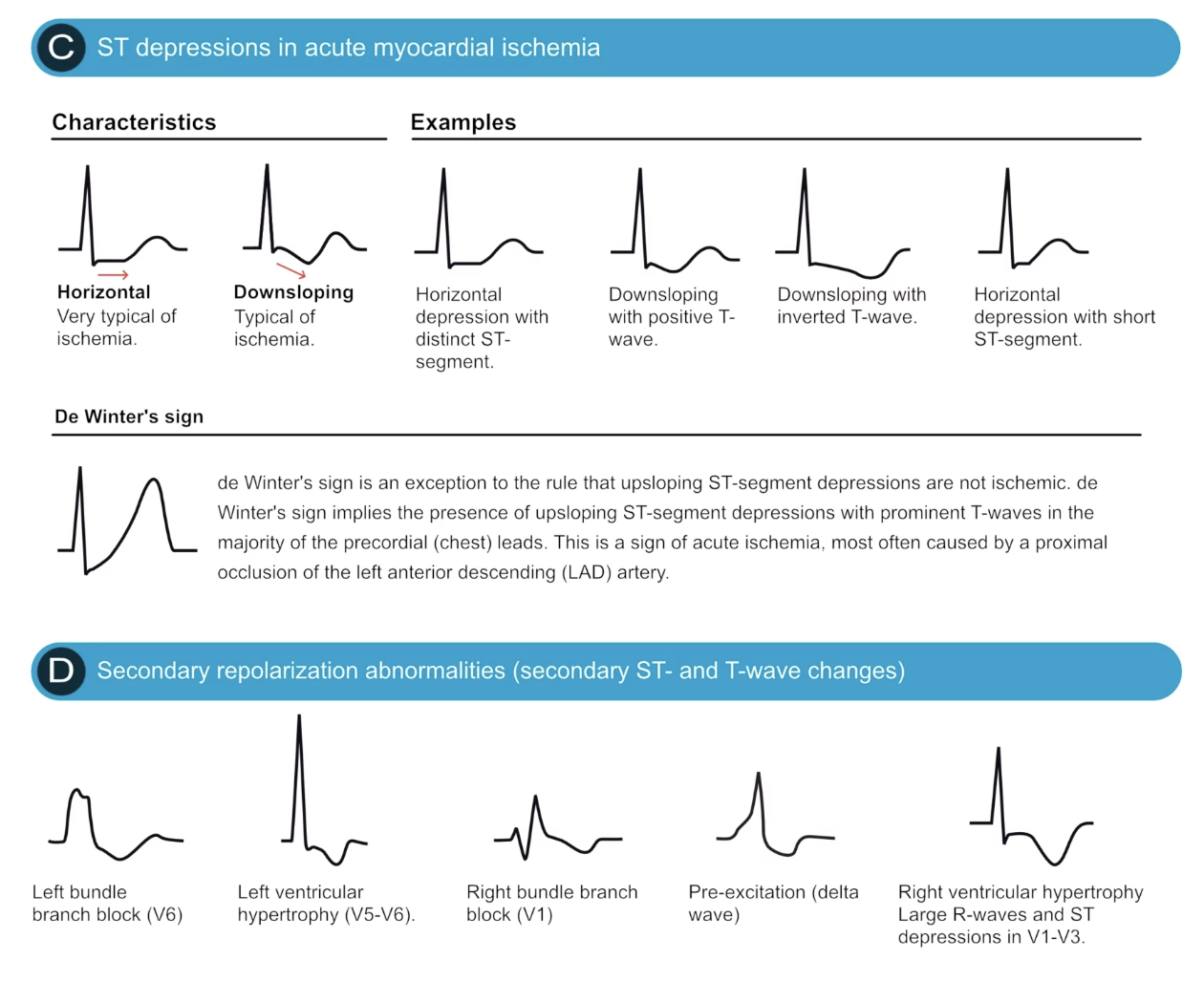
- De Winter's sign - upsloping ST depression with tall T waves in V1-V6 (LAD occlusion equivalent)
- Wellens' syndrome - deep symmetric T inversions or biphasic T waves in V2-V3 indicating critical LAD stenosis
ST depressions and secondary repolarization abnormalities:
T wave changes across conditions:

3. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized atrial electrical activity causing irregular ventricular response. The most common sustained cardiac arrhythmia.
ECG Changes:
- No distinct P waves - replaced by irregular fibrillatory baseline (f waves at 350-600 bpm)
- Irregularly irregular RR intervals - the hallmark finding
- Narrow QRS (unless aberrant conduction or bundle branch block present)
- Variable ventricular rate - typically 100-180 bpm if uncontrolled
- Undulating baseline best seen in V1
ECG features:
- Absent P waves + irregularly irregular rhythm = AF until proven otherwise
- Coarse AF: prominent fibrillatory waves (often seen in rheumatic heart disease)
- Fine AF: barely visible fibrillatory baseline (long-standing AF)
4. Atrial Flutter
What it is: Macro-reentrant atrial circuit (usually right atrium) producing regular atrial rate of ~300 bpm.
ECG Changes:
- Sawtooth flutter waves - regular, negative deflections at ~300 bpm, best seen in II, III, aVF
- 2:1 AV conduction most common - ventricular rate ~150 bpm
- Regular ventricular rhythm (unlike AF)
- Narrow QRS (unless BBB present)
- Carotid sinus massage or adenosine can temporarily increase AV block and reveal flutter waves
5. Complete (Third-Degree) Heart Block
What it is: Complete dissociation between atria and ventricles - no impulses pass through the AV node.
ECG Changes:
- Complete AV dissociation - P waves and QRS complexes are completely independent
- Regular P waves at normal or elevated atrial rate (60-100 bpm)
- Regular escape rhythm at slow ventricular rate:
- Junctional escape: 40-60 bpm, narrow QRS
- Ventricular escape: 20-40 bpm, wide QRS (>120 ms), bizarre morphology
- P wave "marches through" QRS - PR intervals constantly changing
- Bradycardia is prominent; symptoms include syncope (Stokes-Adams attacks)
6. Wolff-Parkinson-White (WPW) Syndrome
What it is: Ventricular pre-excitation via an accessory pathway (Bundle of Kent) bypassing the AV node, predisposing to re-entrant tachycardias.
ECG Changes (classic triad):
- Short PR interval (<120 ms) - impulse bypasses AV node delay
- Delta wave - slurred upstroke at start of QRS (slow accessory pathway conduction through ventricular muscle)
- Wide QRS (>120 ms) - due to pre-excitation + fusion
- Secondary ST-T changes - ST depression and T inversion opposite to delta wave polarity
- Pseudo-infarct patterns - negative delta waves can mimic Q waves
- During AVRT tachycardia: narrow complex (orthodromic, most common) or wide complex (antidromic)
- AF + WPW = extremely fast, irregular, wide-complex tachycardia - potentially fatal
WPW 12-lead ECG example:

7. Acute Pericarditis
What it is: Inflammation of the pericardial sac, causing ST elevations that must be differentiated from STEMI.
ECG Changes (4 stages):
- Stage 1 (acute): Diffuse concave ("saddle-shaped") ST elevations in most leads (I, II, aVL, aVF, V3-V6); PR segment depression (pathognomonic) in same leads; PR elevation in aVR
- Stage 2: ST segments normalize; T waves flatten
- Stage 3: Diffuse T wave inversions
- Stage 4: ECG returns to normal
Key differentiators from STEMI:
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST shape | Concave (saddle) | Convex (tombstone) |
| Lead distribution | Diffuse (all leads) | Regional (territory) |
| Reciprocal changes | Absent (except aVR) | Present |
| PR depression | Yes (pathognomonic) | No |
| Q waves | No | Yes (evolve) |
| ST:T ratio in V6 | >0.25 | <0.25 |
8. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular wall, commonly from chronic hypertension or aortic stenosis.
ECG Changes:
- High-voltage QRS:
- Sokolow-Lyon: S in V1 + R in V5 or V6 >35 mm
- Cornell: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- Left axis deviation (-30° to -90°)
- ST depression and T wave inversion in lateral leads (I, aVL, V5-V6) - the "strain pattern" (secondary repolarization abnormality)
- Left atrial enlargement - broad, notched P waves (P mitrale) or biphasic P in V1
- Prolonged QRS (up to 110 ms)
- Wide QRS transition zone
- In the T-wave panel above: "Left ventricular hypertrophy (V5-V6)" - symmetric T inversions, often very deep, with large R waves
9. Pulmonary Embolism (PE)
What it is: Obstruction of the pulmonary arteries, causing acute right heart strain.
ECG Changes:
- Most common: Sinus tachycardia (most frequent, but nonspecific)
- S1Q3T3 pattern (classic but present in only ~20%): S wave in lead I + Q wave in lead III + T inversion in lead III
- Right heart strain signs:
- New RBBB (complete or incomplete)
- Right axis deviation
- P pulmonale (peaked P waves in II indicating RAH)
- ST depression/T inversion in V1-V4 (right precordial strain)
- New atrial fibrillation or flutter
- Clockwise rotation of precordial leads (persistent S waves through V5-V6)
- Electrical alternans if pericardial effusion develops
- Normal ECG does NOT exclude PE
10. Hypertrophic Cardiomyopathy (HCM / HOCM)
What it is: Genetic disorder with asymmetric myocardial hypertrophy (often septal), causing dynamic LV outflow obstruction and diastolic dysfunction. Leading cause of sudden cardiac death in young athletes.
ECG Changes:
- LVH voltage criteria (similar to hypertensive LVH but often more pronounced)
- Deep, symmetric T wave inversions - most characteristic, especially in V1-V5; often the "giant negative T waves" of apical HCM (Yamaguchi variant: >10 mm inverted T waves in V4-V5)
- Pathological Q waves - narrow, deep Q waves in lateral leads (I, aVL, V5-V6) and inferior leads - due to hypertrophied septum, can mimic old MI
- Left atrial enlargement - broad P waves
- Nonspecific ST changes
- In the T-wave image above: "Hypertrophic cardiomyopathy - Symmetric T wave inversions, most commonly in V1-V3. Often very deep and accompanied by large R waves."
Overview of secondary repolarization patterns across conditions:
Quick Reference Summary Table
| Disease | Key ECG Finding | Leads Affected |
|---|---|---|
| STEMI | ST elevation + Q waves (evolving) | Regional (territory-based) |
| NSTEMI/UA | ST depression, T inversion | Contiguous leads |
| Atrial Fibrillation | Absent P waves, irregularly irregular | All leads |
| Atrial Flutter | Sawtooth flutter waves, 2:1 block | II, III, aVF |
| Complete Heart Block | AV dissociation, escape rhythm | All leads |
| WPW Syndrome | Short PR + delta wave + wide QRS | Dependent on pathway |
| Acute Pericarditis | Diffuse concave ST elevation + PR depression | All leads (saddle shape) |
| LVH | High voltage + strain pattern | Lateral (V5-V6, I, aVL) |
| Pulmonary Embolism | Sinus tachycardia + S1Q3T3 ± RBBB | V1-V4, I, III |
| HCM | Deep T inversions + septal Q waves | V4-V5 (apical), lateral |
Sources: Harrison's Principles of Internal Medicine 22E (ECG chapters); Ganong's Review of Medical Physiology 26E (cardiac electrophysiology); Braunwald's Heart Disease (cardiomyopathy); Tintinalli's Emergency Medicine (ACS, PE); ECG image panels from The Cardiovascular (ECGwaves.com) and GrepMed.
Clinical note: ECG interpretation must always be correlated with clinical context, symptoms, and biomarkers. No single ECG finding is pathognomonic in isolation. When in doubt, compare with prior tracings and involve a senior clinician.
This is a shared conversation. Sign in to Orris to start your own chat.